
Abstract
Background:
Monopolar transurethral resection of prostate (m-TURP) remains the gold standard for benign prostate obstruction (BPO). Recently developed laser surgical technique provides fewer peri-operative complications with equivalent outcomes. Diode laser vaporesection (DiLRP) offers better hemostasis, shorter catheterization duration, and shorter hospital stay, however, deep thermal penetration might cause prolonged prostatic urethra inflammation and subsequent complications. We conducted a retrospective study to compare the pyuria duration and post-operative urinary tract infection sequelae (POUTIs) between DiLRP and m-TURP.
Methods:
From July 2011 to September 2015, we retrieved medical records for patients with lower urinary tract symptoms resulting from prostate obstruction who underwent m-TURP and DiLRP. Demographic characteristics were recorded from a computerized database. The duration of pyuria after operation was compared by Kaplan-Meier analysis and risk factors were evaluated by Cox regression analysis.
Results:
One hundred twelve patients underwent DiLRP and 81 underwent m-TURP performed by the same surgeon during the same period. The mean age of the patients was 72 ± 7.3 years in the DiLRP group and 70 ± 7.6 years in the m-TURP group (p = 0.069). There was a higher percentage of anticoagulant used in the DiLRP group than in the m-TURP group (18.5% vs. 7.4%, p = 0.028). Operation time was longer but post-operative normal saline irrigation interval was shorter in DiLRP compared with m-TURP, respectively (62.8 ± 20.6 vs. 47.4 ± 22.1 minutes, p < 0.001; 2.1 ± 0.3 vs. 2.5 ± 0.9 days, p < 0.001). The post-operative infections were statistically significantly higher in the DiLRP group, including epididymitis (10.2% vs. 1.2%, p = 0.013) and POUTIs-related hospitalization (8.3% vs. 1.2%, p=0.031).The DiLRP resulted in longer pyuria period (16 vs. 12 weeks, p = 0.0014), with factors including operative method by DiLRP (hazard ratio [HR]: 1.828, p = 0.003) and age (HR: 0.665, p = 0.040).
Conclusions:
According to our study, DiLRP associated with more POUTIs is possibly caused by a longer pyuria period. Further larger prospective studies are necessary for the evaluation of the association between post-operative pyuria and POUTIs.
Benign prostate hyperplasia (BPH) represents one of the most common etiologies for aging males with lower urinary tract symptoms (LUTS) [1]. For those who have had a poor response to other medical treatments, the transurethral resection of the prostate (TURP) is still considered the gold standard surgical treatment for BPH [2]. Despite technical improvements, TURP continues to carry a risk of intra- and post-operative complications, especially bleeding and dilutional hyponatremia (transurethral resection [TUR] syndrome). According to studies over past decades, blood transfusion rates for TURP have been 2%–7.1% and early surgical revision rates have been 3%–5% [3]. Although the prevalence of TUR syndrome is rare, it can potentially be a life-threatening complication [3]. As a result, TURP is not recommended for patients who are using anticoagulant drugs or have a prostate heavier than 100 mg [1,4].
To reduce peri-operative morbidity and length of hospital stay, laser prostatectomy has been developed as an alternative therapy [5]. Currently available laser devices include the green light laser, holmium laser, thulium laser, diode laser, and potassium titanyl phosphate/neodymium:yttrium-aluminum-garnet (KTP/Nd:YAG) laser [6]. The diode laser is a relatively new device that provides simultaneous energy absorption by water and hemoglobin. It provides the deepest penetration [8], thus resulting in a combination of excellent hemostasis and efficient tissue ablation [7–10].
There have been randomized controlled trials that have shown the diode laser to be safe and feasible for performing TURP [11–13]. However, many studies have reported more complications after diode laser surgery, such as dysuria, the passing of sloughed tissue, and re-operation because of bladder neck contracture (BNC) than with other energy devices [14,15]. Despite this, there has been no objective evidence found demonstrating a correlation between deep thermal injury from diode lasers and associated complications. Previous studies have evaluated the evolution of pyuria after TURP, which was considered as evidence of prostate fossa remodeling and inflammatory process after prostate surgery [16]. However, there have been no studies exploring the association between pyuria and laser prostatectomy. In this study, we compared the post-operative urinary tract complications in diode laser vaporesection of the prostate (DiLRP) and monopolar transurethral resection of prostate (m-TURP). We also investigated the duration of post-operative pyuria after DiLRP and m-TURP and analyzed the risk factors for prolonged pyuria after surgery.
Patients and Methods
Study population
The Institutional Review Board of Chung Shan Medical University Hospital approved this retrospective cohort study. A single-center database was used to retrieve records from July 2011 to September 2015. We included patients with an initial diagnosis of LUTS caused by prostate obstruction who underwent either m-TURP or DiLRP. The surgical indications adhered to the international BPH guidelines of the European Association of Urology (EAU) [17]. To minimize surgical technique bias and hospital care variability, all surgeries and post-operative care of the enrolled patients were performed or supervised by an experienced urologist. The collected demographic characteristics included the history of the underlying disease, use of anticoagulants or antibiotic agents before the operation, history of transrectal ultrasound (TRUS) biopsy, prostate-specific antigen (PSA) level, estimated prostate size, peri-operative and post-operative details, and hospitalization period. Because of the increased risk of post-operative urinary tract infection (UTI), most patients with pyuria prior to the operation received prophylactic antibiotic treatments [18]. The urine analyses of all enrolled subjects demonstrated no pyuria before operation.
Surgical techniques
All patients were put in the lithotomy position and given a low-pressure irrigation system with a 24-French resectoscope sheath (OES Pro Resectoscope, Olympus, Germany) and suprapubic trocar cystostomy. Monopolar transurethral resection of prostate was performed under spinal anesthesia, and the procedure was performed in the standard manner as described by Hartung et al. [19]. A cutting current of 150 W was used for resection and 70 W for coagulation (HSG-400 HF generator, Olympus, Germany). Diode laser vaporesection was performed under general anesthesia using a 980-nm wavelength diode laser (MEDILAS D200, Dornier MedTech, Germany or Evolve, biolitec, Germany) in a continuous wave mode. A 600-mcm end-firing laser fiber (BareFiber, FiberTech, Germany) was engaged and energy power was set at 100–110 W. The initial incision was made in the 5 to 7 o'clock position from the bladder neck to the verumontanum. The medial lobe was resected and pushed until there was minimal attachment of the adenoma to the bladder neck. The bilateral lateral lobes and anterior lobe were then resected in a similar manner. A bipolar TURP was followed to cut the attached lobes into pieces.
At the end of both procedures, a 22-French three-way urethra catheter with a 30–50 mL indwelling balloon was placed for continuous bladder irrigation with normal saline. All patients were treated with a prophylactic antibiotic of cefazolin 1 g intravenously one hour before operation. The urethra catheter was routinely removed on post-operative day two.
Post-operative urinary tract complications
Post-operative urinary tract complications included BNC, urethral stricture, and post-operative urologic tract infection sequelae (POUTIs). Once the diagnoses of BNC and urethral stricture were confirmed by cystoscopy, they were revised (such as by sounding dilate, urethrotomy, or bladder neck incision) as soon as possible. We defined four events as POUTIs: UTI, epididymitis, acute bacterial prostatitis, and hospitalization because of urologic infection. The definition of UTI was an episode of post-operative clinical symptoms that favored a diagnosis of UTI, fever (body temperature >38.5°C), or hypothermia (body temperature <36°C) associated with bacteriuria with a quantitative count of ≥105 colony forming units of bacteria per cubic milliliter (CFU/mL) in one urine specimen [20,21]. Epididymitis was diagnosed by a gradual onset of a painfully swollen epididymis with no history of direct trauma. A scrotal ultrasound was performed to facilitate a differential diagnosis of epididymitis, however, ultrasonography was not mandatory for a confirmation of the diagnosis [22]. Acute bacterial prostatitis was diagnosed by edematous and a tender prostate by digital rectal examination. If the patient presented with concomitant high fever and bacteremia, pathogen resistance to an oral antibiotic would meet our hospitalization criteria.
Post-operative pyuria duration
The urinary analyses after surgery were checked and recorded until the pyuria resolved or the patient was lost to follow-up. Pyuria was defined as meeting one or more of the following conditions: (1) the presence of 10 or more white cells (CFU/mL) in a urine specimen; (2) positive result on gram staining of an unspun urine specimen; or (3) a urinary dipstick test positive for leukocyte esterase [23]. Pyuria duration was defined as from the day of surgery to the day of the first urine test that revealed clean urine. Pyuria persisting for more than six months or a recurrence after initial pyuria had resolved were excluded from the analysis. The potential risks of prolonged pyuria were analyzed by a Cox regression model.
Statistical analysis
Student t-test, Fisher exact test, and χ2 test were applied for continuous or discrete data analysis. We used Kaplan-Meier curves to estimate the duration of post-operative pyuria. Factors that may be associated with prolonged pyuria were analyzed using a Cox regression model. Factors with a p < 0.05 were considered as confounders. The confounders and well-known prognostic factors in the literature were analyzed further using a multivariable Cox regression. Hazard ratio (HR) and 95% confidence interval (CI) were calculated. All statistical analyses were conducted using the SPSS statistical software program (version 15.0; SPSS Inc., Chicago, IL). All statistical tests were two-sided, and values of p < 0.050 were considered statistically significant.
Results
In total, 189 patients who met the inclusion criteria during the indicated period were enrolled in this study. Of these, 81 underwent m-TURP and 108 underwent DiLRP.
Between the two groups, there were no statistically significant differences in age, body mass index (BMI), diabetes mellitus, hypertension, and prostate size. Anticoagulant agent use was higher in the DiLRP group (18.5% vs. 7.4%, p = 0.028). Before the operation, 31 (38.2%) of the patients in the m-TURP group and 39 (36.1%) of the patients in the DiLRP group had an indwelling catheter because of urinary retention, but there was no statistically significant difference between the groups.
Among the patients of the DiLRP group, a longer operative time (61.8 minutes vs. 47.4 minutes, p < 0.001) was noted, but it had a shorter catheterization time (3.1 days vs. 3.5 days, p < 0.001) and hospital stay (3.2 days vs. 3.5 days, p = 0.002). The details of patient characteristics and peri-operative details are summarized in Table 1.
Baseline Characteristics and Peri-Operative Detail According to Surgical Type of One Hundred Eighty-Nine Patients
Data were presented by mean ± SD (range) or n (%).
p value obtained by Student t-test or χ2 test.
m-TURP = monopolar transurethral resection of prostate; DiLRP = diode laser vaporesection of prostate; TRUS = transrectal ultrasound biopsy; PSA = prostate-specific antigen; SD = standard deviation.
Post-operative urinary tract complication
The incidence of BNC was higher in the DiLRP group (9.3% vs. 3.7%), but there was no statistical significance. Urethra stricture was higher in the DiLRP group (5.6% vs. 2.5%), which was also without statistical significance. Regarding POUTIs, the incidence of epididymitis and urologic infection-related hospitalization were higher in the DiLRP group (10.2% vs. 1.2%, p = 0.013 and 8.3% vs. 1.2%, p = 0.031, respectively). Although UTI was more common in the DiLRP group (11.1% vs. 4.9%, p = 0.131), the difference was not statistically significant. Only three patients presented with acute prostatitis (two in the DiLRP group, one in the m-TURP group) and there was no statistical difference between the groups. Of the patients who were hospitalized because of urologic infection, nine patients had received DiLRP (eight patients had pyelonephritis and one patient had epididymitis) and one patient had received m-TURP (pyelonephritis). The details of the post-operative urinary tract complications are shown in Table 2.
Post-Operative Urologic Tract-Associated Complication According to Surgical Type
χ2 test.
BNC = bladder neck contracture; PN = pyelonephritis.
Risk factors of post-operative pyuria
The Kaplan-Meier curves for pyuria resolution in the DiLRP and m-TURP groups are shown in Figure 1. A comparison indicates no difference in the post-operative pyuria curve between the two groups over the first five weeks. However, after the fifth week post-surgery, the recovery from pyuria was higher in the m-TURP group. After the fifth week, patients who had received m-TURP had a quicker pyuria resolution than those who had received DiLRP. The patients in the DiLRP group had a longer pyuria duration as compared with the m-TURP group (16 vs. 12 weeks, p = 0.0014).
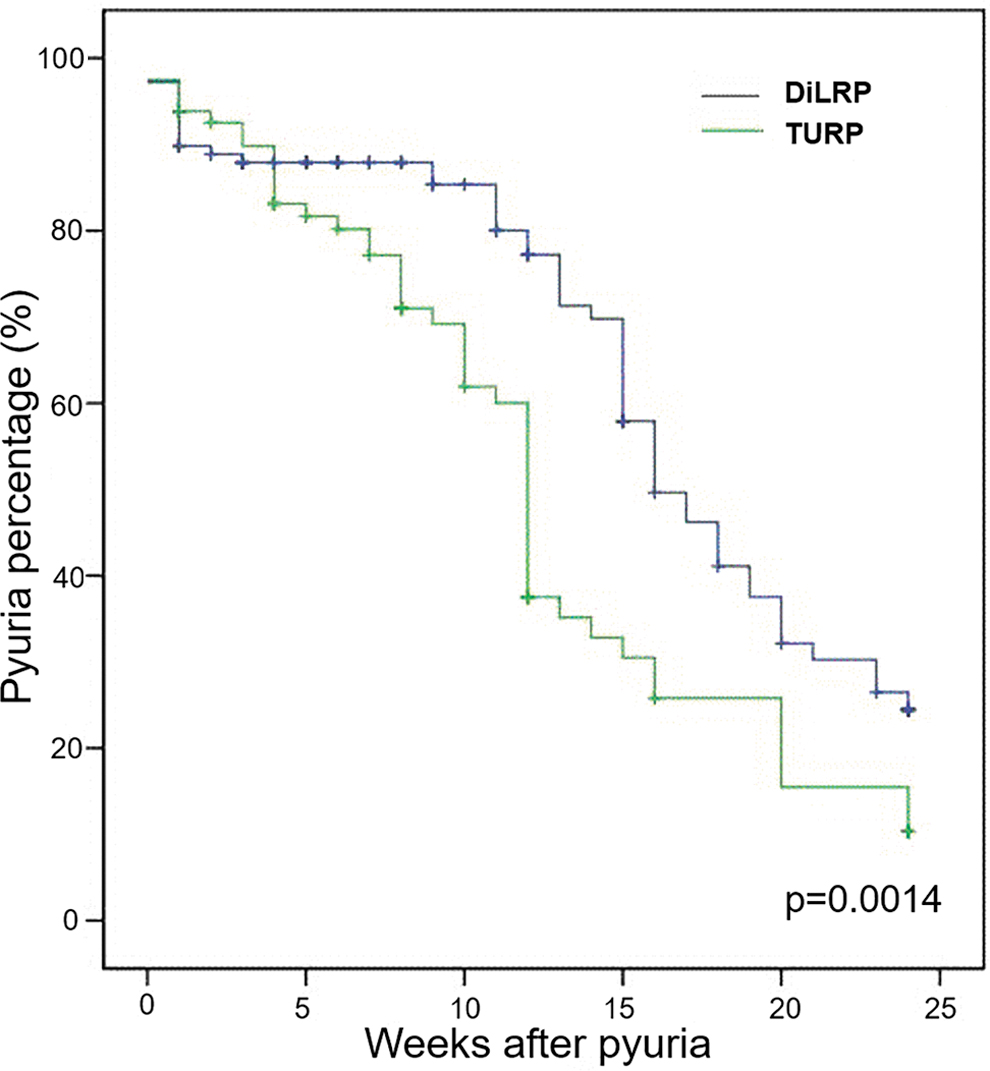
Kaplan-Meier curve analysis compares post-operative pyuria duration according to surgical type. Median time of pyuria in the DiLRP group was 16 weeks (95% CI 14–18). Median time of pyruia in m-TURP was 12 weeks (95% CI 11–13), p = 0.0014. DiLRP = diode laser vaporesection of prostate; m-TURP, monopolar transurethral resection of prostate; CI = confidence interval. Color image is available online.
In a univariable analysis by a Cox regression model, the risk factors included: operative method (DiLRP/m-TURP, HR = 1.824, 95% CI: 1.227–2.710) and age (≤71/>71 years old, HR = 0.967, 95% CI: 0.943–0.992). Other risk factors, including diabetes mellitus, hypertension, BMI, pre-operative anticoagulant, antibacterial prophylaxis, pre-operative pyuria, history of TRUS biopsy, PSA, and resected prostate weight, revealed no statistical differences (Table 3). The multivariable analysis also identified operative method (DiLRP/m-TURP, HR = 1.828, 95% CI: 1.235–2.707) and age (≤71/>71 years old, HR = 0.665, 95% CI: 0.450–0.982) were both important risk factors for prolonged pyuria. In order to verify that the results were not affected by other confounding factors, we used a verification analysis. We added a factor of p < 0.1 from the univariable analysis (pre-operative anticoagulant) into the multivariable analysis and we added risk factors published in previous studies (resected prostate weight, diabetes mellitus) [8,16]. The results remained unchanged. The details are shown in Table 3 and Table 4.
Hazard Ratio of Prolonged Pyuria and Multivariable Cox Regression with Adjustments for Different Factors
Multivariable analyses control by risk factors reported by other studies.
Multivariable analyses control by factors that p < 0.1 in univariable analyses.
HR = hazard ratio; CI = confidence interval; operative method = TURP vs. LASER; DM = diabetes mellitus.
Hazard Ratio of Prolonged Pyuria and Multivariable Cox Regression with Adjustments for Operative Method and Age
Univariable analyses p < 0.05.
Multivariable analyses p < 0.05.
HR = hazard ratio; CI = confidence interval; BMI = body mass index; DM = diabetes mellitus; HTN = hypertension; Pre-UA = urinalysis before operation; Pre-anticoagulant: use of anticoagulant before operation; TRUS = transrectal ultrasound biopsy, PSA = prostatic-specific antigen; Post-Qmax = maximun flow rate after operation.
Discussion
To our knowledge, this retrospective cohort study was the first study to illustrate prolonged pyuria after DiLRP compared with m-TURP. We have further demonstrated that operative method and age are independent risk factors for prolonged post-operative pyuria. In addition, we have shown that DiLRP has a greater potential risk for POUIs, including post-operative epididymitis and urologic infection-related hospitalization.
The diode laser has recently been introduced as a device for the treatment of BPH and generates monochromatic wavelengths of 940, 980, or 1470 nm. These wavelengths produce high simultaneous energy absorption in water and hemoglobin, thus offering high tissue ablation with excellent hemostasis. Previous studies have confirmed that diode laser surgery is equally as effective as other methods and feasible for the treatment of benign prostatic hypertrophy. Two randomized control trials compared diode laser vaporization of the prostate with m-TURP and found similar operative times and an improvement in functional outcomes at the 12-month follow-up. The diode laser vaporization of the prostate also had a shorter post-operative catheter placement time (88.9 vs. 20.1 hours, p = 0.0001) and hospital stay (59.9 vs. 25.8 hours, p = 0.0001) [11,12]. Another two randomized control trials compared diode laser enucleation of the prostate with bipolar transurethral resection of prostate (b-TURP). In addition to the above benefits, the diode laser was more effective in reducing blood loss during surgery [13,24]. There were two meta-analysis studies comparing m-TURP, b-TURP, and different laser devices for BPH. Both studies also suggested that the diode laser had the shortest post-operative indwelling catheter time and a functional outcome comparable to the other devices [6,25]. Because of the tissue cauterization and hemostasis abilities of the diode laser, it is recommended by the EAU for patients who are using anticoagulants [26].
Although diode lasers have been proven to be safe and effective in many studies, their deeper energy penetration is likely to be associated with greater thermal damage. In previous in vivo and ex vivo studies, the coagulation depths of different surgical devices have been well investigated. The diode laser has the deepest coagulation depth, with a depth of approximately 5 mm. The coagulation depth for other devices is 0.2 mm for m-TURP and b-TURP, 0.2 mm for thulium laser, 0.4 mm for holmium laser, and 0.84 mm for green light laser [21,27,28]. Deeper thermal damage is thought to be the cause of post-operative complications. In other words, there will be more necrotic tissue peeling in the short and medium term after surgery, which can cause voiding obstruction and LUTS. Occasionally, some patients may even experience acute urinary retention, requiring surgery to remove necrotic tissue. Deep tissue damage to the bladder neck can lead to subsequent bladder neck stenosis, which may also require re-operation [29]. Chiang et al. compared diode laser surgery and green light laser surgery and found that more patients needed re-operation for BNC after diode laser surgery (9.1% vs. 2.4%). The proportion of urethral stricture was also higher (5.5% vs. 2.4%) [14].
In addition, there were more patients (1.8% vs. 0%) who developed urethral stones during the recovery process, which may be related to deep thermal damage and prolong the re-epithelialization of the urethra [14]. Another study showed relatively higher BNC rates requiring re-operation in DiLRP compared with b-TURP (18.2% vs. 1.6%, p < 0.05) [15]. Chen et al. [30] reported that 14.5% of patients had a large amount of necrotic tissue exfoliation after diode laser surgery, which needed further intervention. In our study, the BNC and urethra stricture rates were 9.3% versus 3.7% and 5.6% versus 2.5% between the DiLRP and m-TURP groups, respectively, but there was no statistical significance, which is inconsistent with previous studies. Some of the literature has also mentioned that diode laser surgery has more post-operative temporary urinary incontinence, frequency, dysuria, scrotal edema, and perineal pain [14,31–33]. All of these symptoms may be caused by deep thermal damage, resulting in post-operative inflammation and swelling of the tissue.
Post-operative infection is also an important issue that may decrease patient satisfaction and prolong antibiotic therapy, thus increasing costs and the length of hospital stay [34]. A prolonged inflammatory reaction could be a risk factor for urologic infection [35]. A previous study reported that patients receiving diode laser surgery had a higher rate of post-operative epididymitis (9.1% vs. 1.2%), and this result was the same as in our study [14]. In our study, epididymitis was higher in the DiLRP group (10.2% vs. 1.2%, p = 0.013). Although the rate of UTI was not statistically different between the two groups, the proportion was higher in the patients receiving DiLRP (11.1% vs. 4.9%). Of note, the UTIs requiring hospitalization were higher in the DiLRP group (8.3% vs. 1.2%, p = 0.031), indicating that infection is more severe after diode laser surgery.
Despite the deep thermal injury of the diode laser, there is currently no objective evidence in the literature to confirm the correlation between diode laser surgery and urinary tract complications. Pyuria refers to the white blood cells in the urine, which usually means that the urinary tract is in an inflamed state and is often reflected in the symptoms of urinary tract irritation or painful urination in the patient [36]. There have been studies using post-operative pyuria as evidence of tissue repair and inflammatory response [8,9,16]. Previous studies have found that mean pyuria persistence after m-TURP ranges from 58 to 266 days [8–10,16]. Previous studies have also analyzed the risk factors that have resulted in longer pyuria duration after m-TURP, including heavier resected prostate tissue, diabetes, pre-operative pyuria or bacteriuria, post-operative hypoproteinemia, older age, and pre-operative catheter placement [8,16]. However, two studies found that only resected prostate tissue weight and diabetes were independent risk factors for post-operative pyuria [9,10]. In our study, the median duration of pyuria in the m-TURP group was 12 weeks (84 days), which was consistent with previous studies [8–10, 16]. In contrast, pyuria persistence after DiLRP was significantly longer and of up to 16 weeks (p = 0.0014). In our multivariable analysis, we found the main risk factor was an operative method of DiLRP (HR = 1.824, 95% CI: 1.227 ∼ 2.710) and another was old age (HR = 0.665, 95% CI: 0.450 ∼ 0.982). This result can be attributed to the fact that the coagulation depth of the diode laser is dozens of times greater than that of the m-TURP, and this may also explain the high prevalence of other post-operative complications after diode laser surgery.
Resected prostate weight, which has commonly been regarded as a risk factor in previous studies, was not among the risk factors found in our multivariable analysis; a possible explanation may be that some of the prostate tissue was vaporized by the diode laser, resulting in an underestimation of the resected prostate weight. As seen in previous studies [9,10,17], post-operative pyuria is a surrogate of tissue repair and inflammation. Because aging is associated with increased inflammation, many tissues in older patients are probably in a chronically inflamed state [37]. Our data support age as another independent risk factor for post-operative pyuria, which is consistent with the current evidence in the literature.
Some limitations to the current study need to be mentioned. First, because of the retrospective study design, an inherent bias is inevitable. Second, more patients in the DiLRP group took an anticoagulant agent before surgery (18.5% vs. 7.4%, p = 0.028). However, there is no evidence that the use of an anticoagulant agent or cardiovascular disease increases the risk for UTIs or prolongs post-operative pyuria. Furthermore, according to real-world guidelines, laser prostate surgery is recommended for patients who are at a higher risk for bleeding, such as those on anticoagulant drugs. Finally, the small sample size of this study might unavoidably skew the results. Additional larger and prospective randomized studies are needed.
Conclusion
Our findings confirm good functional improvements after both m-TURP and DiLRP, as was the case in the previous literature. Age is an independent risk for post-operative pyuria. With its deep thermal penetration, DiLRP might also prolong pyuria and cause associated complications. The risk of POUIs was higher in the patients who had received DiLRP.
Funding Information
No financial support was received.
Footnotes
Author Disclosure Statement
No competing financial interests exist.