
Abstract
Background:
Infection of vascular grafts is a life-threatening complication in cardiovascular surgical procedures. This experimental study tested the efficacy and possible harmful effects of daptomycin pre-treatment in vivo in prevention of vascular graft infection caused by Staphylococcus aureus.
Methods:
Polyethylene terephthalate (PET) patches (5 × 7 mm) were sewn on the infra-renal abdominal aorta of 32 New Zealand White rabbits. Before implantation, patches either were pre-treated for 15 min with daptomycin in one group (n = 13) or left untreated in the other group (n = 13) before contamination with 100 mcL bacterial solution (1 × 1010 colony-forming units [CFU] per mL). Six animals with uninfected patches without (n = 3) or with (n = 3) daptomycin pre-treatment served as controls. On postoperative day seven, all patches were explanted, washed with phosphate buffered saline, and sonicated to release viable adherent bacteria. The CFUs were quantified and aortic tissues were histologically examined. In addition, bacterial adherence on the patches was analyzed using scanning electron microscopy (SEM).
Results:
In the daptomycin pre-treatment group, significantly reduced numbers of CFUs on the patches were observed, compared with non–pre-treated patches (3.21 × 102 ± 1.02 × 103 mL−1 vs. 5.18 × 105 ± 1.05 × 106 mL−1; p < 0.001). Peri-vascular abscesses were visible in all rabbits with S. aureus infected patches, whereas no signs of inflammation were found in the daptomycin pre-treatment group or the control groups.
Conclusions:
Daptomycin showed excellent in vivo antibacterial activity against vascular graft infection caused by S. aureus, compared with non–pre-treated grafts, resulting in a significant reduction in bacterial infection and prevention of abscess formation. No harmful effects of the antibiotic pre-treatment could be observed.
In cardiovascular surgical procedures, bacterial colonization and infection of implanted medical devices and vascular grafts is a feared complication because of the life-threatening consequences. Infection rates range 1%–6%, and mortality rates vary between 20% and 75%, depending on the type and location of implants [1–4].
Infections can be divided into early and late vascular graft infections. In early vascular graft infection, Staphylococcus aureus is the predominant species in about 60% of cases, whereas in late infections, S. epidermidis and gram-negative bacteria such as Escherichia coli and Pseudomonas aeruginosa play a leading role [5–8]. An early infection on a medical implant is mainly caused by bacterial inoculation at the time of operation. Initial bacterial adhesion precipitates biofilm formation on the implant surface.
Despite well-established peri-operative preventive strategies like topical disinfection, asepsis, and administration of systemic antibiotic prophylaxis [9], bacterial colonization still takes place. Intravenous antibiotic agents are often unable to reach an appropriate topical concentration on a medical implant and to penetrate a pre-existing biofilm, which protects the embedded bacteria [10]. Consequently, local antibiotic pre-treatment was introduced, and several studies have reported promising results [10–15].
Daptomycin is a cyclic lipopeptide and inserts into the bacterial membrane, leading to potassium release, depolarization, inhibition of protein and nucleic acid synthesis, and, consequently, causing cell death [16,17]. Rifampin is still considered the gold standard for antibiotic pre-treatment or impregnation [18], but daptomycin alone and in combination with rifampin was able to increase the efficacy and even reduce the incidence of rifampin resistance in vivo [12, 13]. In a comparative in vitro study, we could demonstrate that rifampin is an effective antimicrobial agent, but is toxic when exposed to endothelial cells [15].
In our previous work [10,15,19, 20], we have shown that antibiotic pre-treatment before inoculation with bacteria is an effective strategy to reduce bacterial colonization and infection of medical implants. Our department has therefore adopted an internal standard operating procedure that requires soaking of all cardiovascular implants (e.g., vascular prostheses, pacemaker casings and electrodes, heart valves, ventricular assist devices) in antibiotic solution before implantation.
The aim of this study was to evaluate the efficacy of daptomycin pre-treatment of vascular prostheses with respect to prevention of peri-operative graft infection in vivo. S. aureus was chosen as the infectious agent, because it is the predominant gram-positive micro-organism involved in early vascular graft infection. Particular attention was given to investigating the amount of bacteria and biofilm formation on the graft surface, possible harmful effects of antibiotic pre-treatment on graft and surgical site healing, and whether local antibiotic pre-treatment could prevent bacterial infection up to one week post-implantation.
Methods
Bacterial strain
For this experimental study, we used a pathogenic for humans S. aureus subsp. aureus DSM 20231 strain (type methicillin-sensitive). It was subcultured on tryptic soy broth (Oxoid, Hampshire, UK), according to the recommendations of the German Collection of Microorganisms and Cell Cultures GmbH (www.dsmz.de). The 1 × 1010 colony-forming units per milliliter (CFU/mL) were used for graft contamination.
Antibiotic agent
Sterile solution preparation of daptomycin 50 mg/mL (Cubicin® 500 mg, Novartis Pharma GmbH, Nurnberg, Germany) was performed according to manufacturer's instructions for intravenous (IV) application in humans (500 mg daptomycin +10 mL 0.9% NaCl +2 mL 0.23 mmol/mL CaCl2 was added additionally for solution stability). The antibiotic concentration in the prepared solution was 41.66 mg/mL. The solution was prepared fresh for each experimental day and was used for soaking all patches on that day.
The minimal inhibitory concentration (MIC) of daptomycin for the S. aureus strain was evaluated using the daptomycin DAP MIC test strip (Liofilchem, Italy).
Vascular grafts
Commercially available knitted double-velour vascular grafts made of fine polyester fibers (polyethylene terephthalate [PET]) and impregnated with absorbable bovine gelatin (Uni-Graft®, B. Braun Aesculap, Tuttlingen, Germany) were used. The grafts were processed to 5- × 7-mm patches under aseptic conditions before implantation.
Animals
For this in vivo study, 32 female New Zealand White rabbits ([Crl:KBL[NZW], Charles River Laboratories Int., Kisslegg, Germany), weight range 2,000–2,500 g, where used, because of their transferability in terms of biochemical reactions against an infection. All animals received care in accordance with the German animal protection legislation, approved by the local Institutional Animal Care and Research Advisory Committee and permitted by the Animal Welfare Service of the Lower Saxony State office for Consumer Protection and Food Safety (Niedersaechsisches Landesamt fuer Verbraucherschutz und Lebensmittelsicherheit, Dez. Tierschutz, Oldenburg, Germany. AZ 10/0058).
Each rabbit was held in an individual cage of a ground size of 5,460 cm2 and a height of 60 cm. During the entire study, the animals were kept at our laboratory under veterinary supervision at a room temperature of 20°C ± 1°C and humidity of 50% ± 3% with active ventilation systems and received a standard diet of 100 g daily as well as hay and water ad libitum. The room was illuminated for 14 h every day, and the active ventilation system was providing fresh air continuously.
Surgical protocol
Pre-medication before operation was performed using a 10% ketamine hydrochloride solution 25 mg/kg (WDT, Garbsen, Germany), 5 mg/animal midazolam hydrochloride (ratiopharm GmbH, Ulm, Germany), and 0.1 mg/animal glycopyrronium bromide (Riemser Arzneimittel AG, Greifswald, Germany).
Anesthesia was induced via IV application of 0.1–0.2 mL of propofol 10 mg/mL (B. Braun, Melsungen, Germany). After endotracheal intubation with a 2.5 mm silicone tracheal tube (Mallinckrodt Medical, Athlone, Ireland), inhalative anesthesia was maintained with 2% isoflurane (cp-pharma, Burgdorf, Germany).
After median laparotomy, the infra-renal portion of the abdominal aorta was visualized under sterile conditions. In the antibiotic pre-treatment group, the patches were soaked and left in the prepared daptomycin solution inside a small surgical bowl for 15 min before implantation and inoculation. This period was adopted from our clinical practice and previous in vitro experiments.
The prepared 5- × 7-mm PET patches were then sewn at four points to the adventitial layer, using polypropylene 6-0, covering up the upper half of the vessel (Fig. 1). After IV application of 100 IU/kg heparin solution, sutures were placed both on the patch and the adventitial layer, and a bulldog clamp was placed for approximately 2 min cranially of the patch to stop proximal blood flow.

Intraoperative view of the four-point fixated polyethylene terephthalate patch on the infra-renal abdominal aorta of a rabbit. Color image is available online.
Then, the patch was lifted, and a 2-mm incision was made into the abdominal aorta to ensure blood contact on the lower patch surface. The patch was then fixated with four knots until the incision was covered up fully and perfusion was released. Pulse was checked cranially and caudally to ensure intact lower limb perfusion. In both intervention groups, 100 mcL of the prepared bacterial solution was then inoculated directly onto the patch using a tuberculin syringe.
Six rabbits served as control groups. In one of the control groups (n = 3), a native PET patch was implanted without daptomycin pre-treatment, and in the other group (n = 3), a pre-treated PET patch without bacterial contamination was implanted.
Finally, the peritoneum was adapted over the patch; the abdominal muscle layer was closed using Polypropylene 5-0 and the skin using Mersilene 4-0. Carprofen (Pfizer GmbH, Berlin, Germany) 2 mg/kg was given for pain control post-operatively and on the next two days once daily. Weight and rectal temperature were surveyed on a daily basis. The surgical incision site was checked daily.
All animals were euthanized after explantation of the grafts under sterile conditions seven days after implantation.
Figure 2 shows a schematic overview of the experimental study protocol.
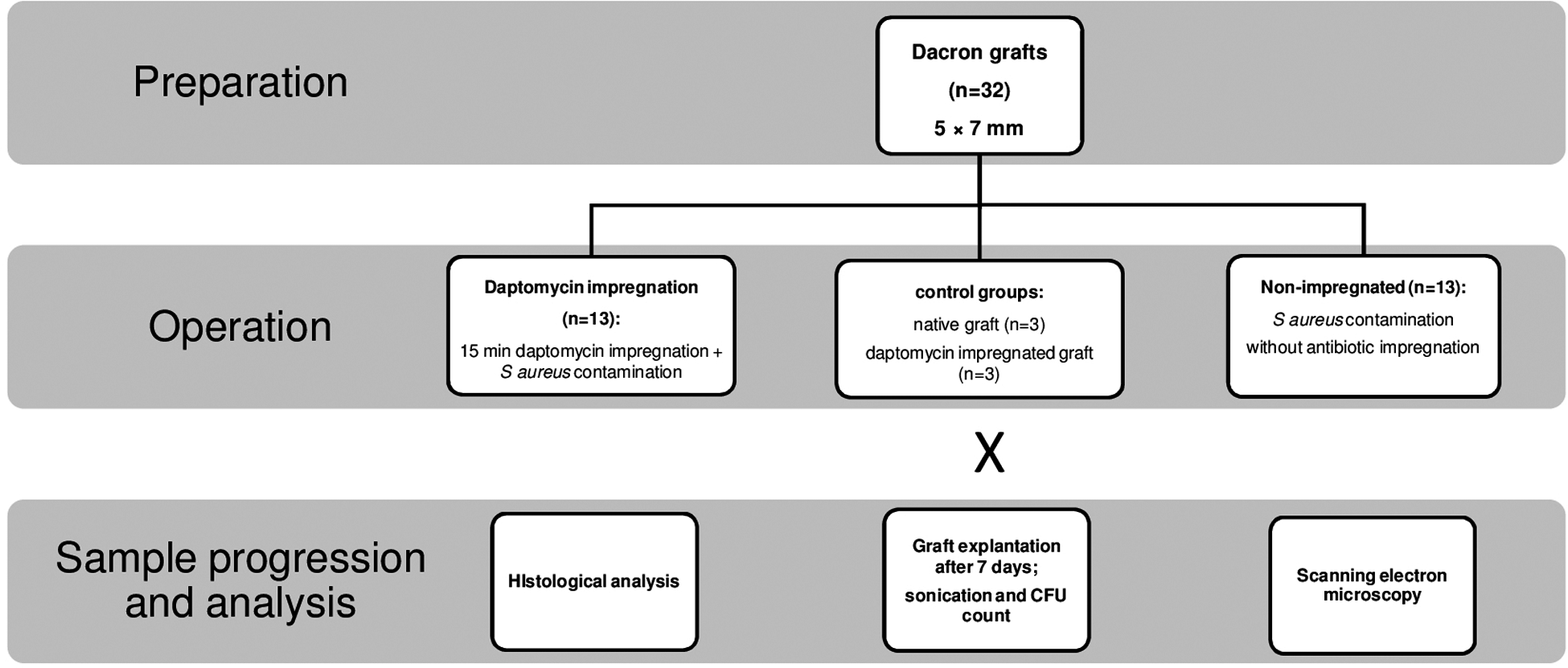
Schematic overview of the experimental study protocol. CFU = colony-forming unit.
Sample cultivation and bacterial count
After explantation, all patches were harvested in sterile 5 mL phosphate buffered saline (PBS) in 15 mL Falcon™ tubes and underwent sonication (Elma, Singen, Germany) at 40 kHz, 180 W, and 37°C for 20 min to release viable adherent bacteria. Afterward, six decimal dilution steps took place, and 100 mcL of the diluted solutions were plated onto tryptic soy agar (TSA) plates, after incubation for 24 h at 37°C. The CFUs per 100 mcL for the solution before dilution and all the diluted solutions were counted using the Gel Doc Gel Documentation System (Bio-Rad, Munich, Germany).
Scanning electron microscopy (SEM)
The patches for SEM were fixed in 2.5% glutaraldehyde and sodium cacodylate buffer (0.2 M, pH 7.3), dehydrated with an increasing ethanol series and critical point—dried with a CPD 030 dryer (BAL-TEC GmbH, Schalksmühle, Germany). They were coated with gold palladium using a Polaron E5400 SEM sputtering system, and biofilm formation was examined with the SEM (FEI Quanta 400) at Laser Zentrum Hannover, Germany.
Histology
During explantation of the PET patches, 2 cm pieces of the aorta under the patch and the surrounding tissue were harvested from one animal of each of the four groups and prepared for histology. Fixation was performed with formaldehyde, after paraffin embedding and hematoxylin and eosin staining.
Statistical analysis
All analyses were performed and graphs were created with GraphPad Prism V7.04 (GraphPad Software, Inc., San Diego, CA). Quantitative culture results are presented as arithmetic mean ± standard deviation and range. Comparisons between the groups were performed using the Mann-Whitney-test. Differences at p < 0.05 were considered statistically significant.
Results
Daptomycin pre-treatment significantly reduces bacterial graft contamination
The MIC of daptomycin for the bacterial strain used in the experiments was 0.5 mcg/mL. The mean amount of the impregnated antibiotic agent within each graft was 23 ± 2 mg, measured by the weight of each graft before and after the soaking process. Bacterial count in the solution was 3.21 × 102 (± 1.02 × 103, range: 0.0–3.69 × 103 CFU/mL) for the pre-treated, and 5.18 × 105 (± 1.05 × 106, range: 3.0 × 103 – 3.80 × 106 CFU/mL) for the non–pre-treated patches, respectively. Differences between the two groups were statistically significant (p < 0.001). These results are presented in Figure 3.
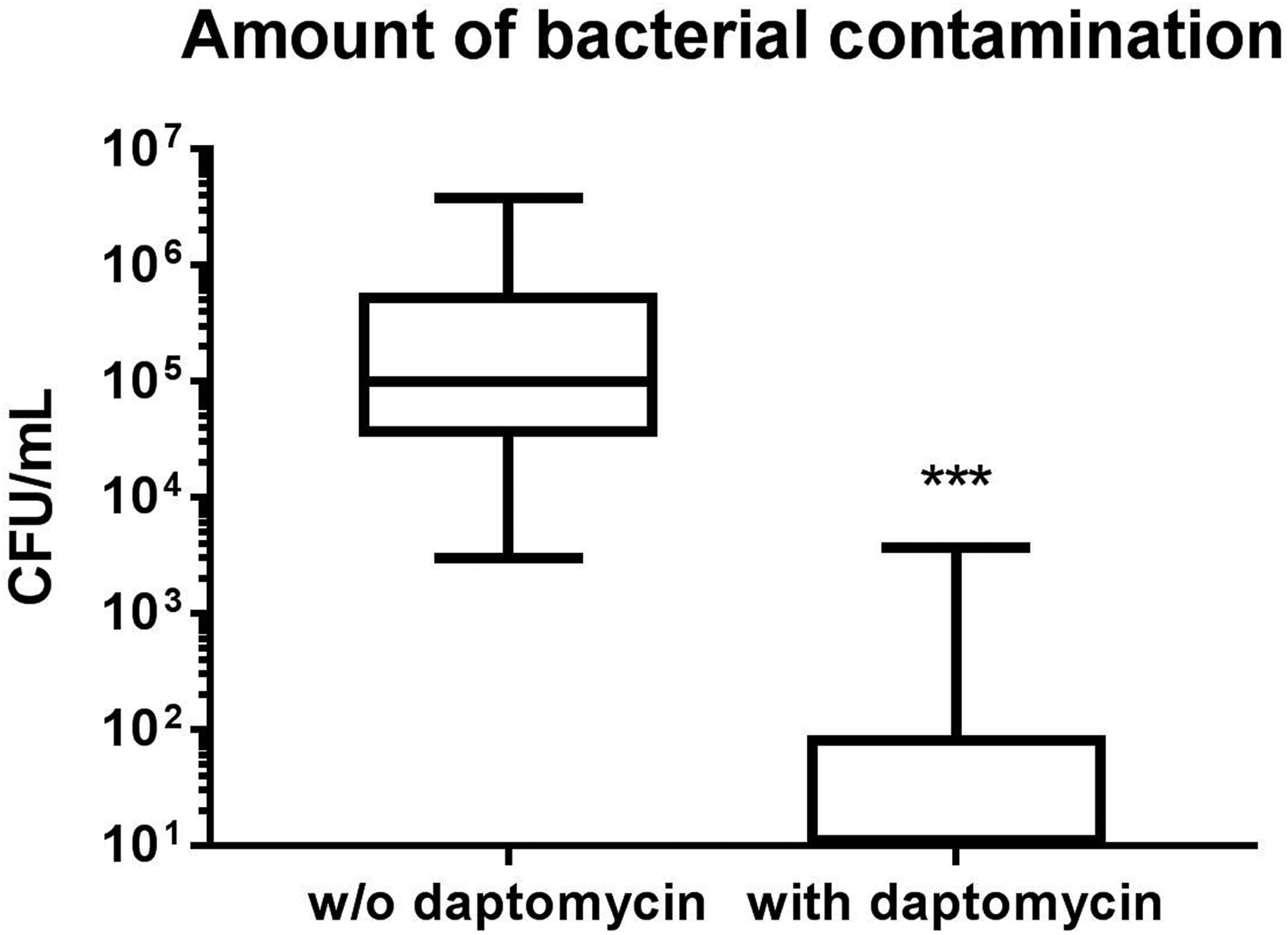
Concentration of bacteria in phosphate buffered saline after sonication of the non–pre-treated and the pre-treated patches from the experimental groups. CFU = colony-forming unit.
In the daptomycin pre-treatment experimental group, eight of 13 animals (61.5%) had no microbiologically detectable contamination of the implanted patches (PBS solution from the explanted samples showed no detectable released bacteria on the TSA plates). In the non–pre-treatment experimental group, all animals presented with a detectable purulent bacterial infection.
Negative in vitro controls (n = 8, PBS only) remained sterile. From both animal groups that served as in vivo controls, the samples remained negative for micro-organisms throughout sample progression.
Daptomycin prevents abscess formation
During the study, abscesses developed in all animals in the non–pre-treatment and S. aureus contaminated group. Figure 4 shows the macroscopic aspects of the patches in the four different groups at the time of explantation, seven days after the initial surgical procedure. The native patches were covered with aortal and para-aortal tissue. No inflammation around the patch was visible. Examination after explantation did not detect any bacterial infection (Fig. 4A). The same occurred with the patches that were pre-treated before implantation, but not contaminated (Fig. 4B). The healing process around the patches was normal, and no abscesses or any inflammatory processes were visible. Microbiologic analysis showed no viable bacteria on the patches.

Macroscopic aspects of the four different groups at the time of patch explantation: (
In the group where the patch underwent pre-treatment before bacterial contamination (Fig. 4C), daptomycin was able to prevent the development of pus-filled abscesses, as occurred in every animal of the non–pre-treated and infected patches (Fig. 4D).
Histologic examination of the aortal and para-aortal tissue of the four groups (Fig. 5) showed normal aortal cell characteristics in the animals that received a native patch implantation (Fig. 5A) or a daptomycin pre-treated patch (Fig. 5B). In the specimen of daptomycin pre-treated animals, histologic evidence of relevant neutrophil granulocyte invasion or otherwise inflammation was absent (Fig. 5C), whereas signs of abscess formations in all the histologic specimens of non–pre-treated infected patches, including diffuse granulomatous infiltration, edema of the surrounding tissue and dilatation of capillaries were observed (Fig. 5D).

Histologic examination of aortic tissues of the four groups after patch explantation: (
In the SEM analysis, normal cells—e.g., erythrocytes—were not harmed by daptomycin pre-treatment and could be seen throughout the histologic sections and the SEM images (Fig. 6A–C). Massive staphylococcal colonization on the non–pre-treated graft surface was visible (Fig. 6D), whereas in the pre-treatment group, biofilm and abscess formation could be prevented.
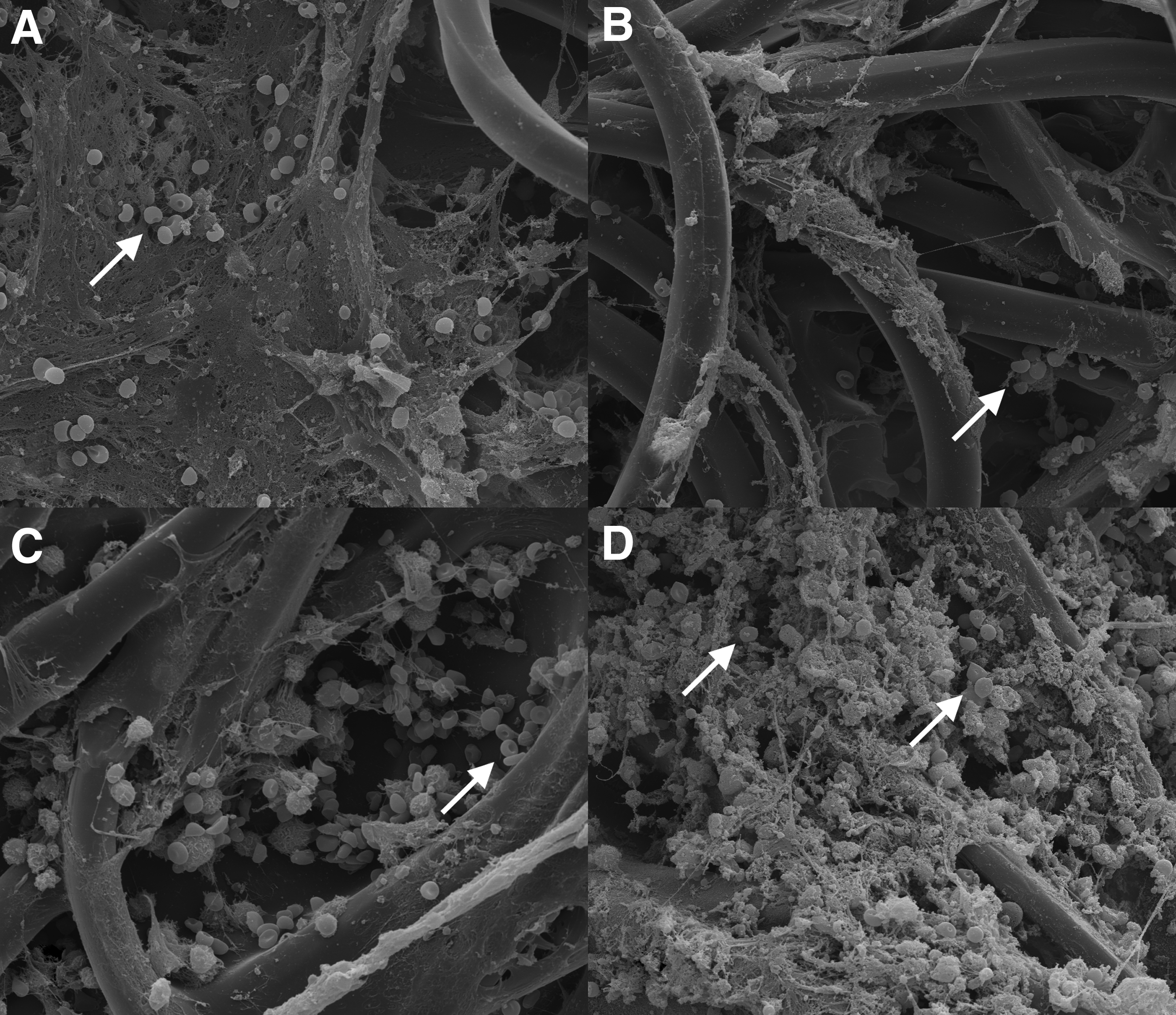
Scanning electron microscopy images of the four groups at 2,000 × magnification:
Every operated animal in this study was able to participate for the entire time period. None of the animals had developed an increase of body temperature longer than one day or significant weight loss >20% during the post-operative course.
Discussion
Vascular graft infection is a severe complication in cardiovascular surgical procedures with implications for patient morbidity, death, and costs [21]. Therefore, this study was conducted to test the antibiotic agent daptomycin in a model of vascular graft infection by S. aureus in rabbits. Clinically used double-woven velour vascular grafts were pre-treated with daptomycin, and the influence of antibiotic pre-treatment on the bacterial adhesion and growth on the graft surface was analyzed.
To evaluate our in vitro experiences with antibiotic pre-treatment, we chose a rabbit model of vascular graft infection over a period of seven days. This simulates the effect of pre-treatment on delayed contamination consistent with the clinical occurrence of early graft infection in the peri-operative or early post-operative phase.
The most frequent cause of vascular graft infection remains contamination of the graft during implantation or in the peri-operative period, with S. aureus and S. epidermidis being the most common causative agents [22]. In this context, biofilm formation remains the most relevant feature for the pathogenicity of bacteria colonizing surgical implants, because it protects them from host defence mechanisms and systemic antibiotic agents. To address this issue, it is clinical practice to administer peri-operative systemic antibiotic agents [23], to maintain aseptic conditions during operation, and, as a newer feature, to use local antibiotic impregnation [24–26].
Antibiotic pre-treatment of vascular grafts before implantation for local antibiotic release is a useful method for the reduction or even prevention of vascular graft infection. This is especially important during and in the first days after implantation of foreign material, because antibiotic pre-treatment has a protective effect on the graft surface until it is fully covered with fibroblasts and incorporated into the surrounding tissue.
Pre-treatment with antibiotic solution should meet several important criteria [27]. The agent should have a lasting effect against the bacteria most commonly involved in vascular graft infections. The concentration used topically at the graft surface should exert a protective effect, without causing any toxic or allergic reactions in the surrounding tissue. It is essential for the impregnation agent not to disturb the healing process after graft implantation and, on the other hand, prevent bacterial adhesion on the graft surface.
We could demonstrate in vitro that antibiotic impregnation is effective in preventing infection of cardiovascular implants [10,15,19,20] and have tested different antibiotic agents against gram-positive and gram-negative bacteria, leading to a standard operating procedure in our department of soaking all cardiovascular implants in antibiotic solution before implantation.
Other groups have reported similar findings in different in vivo models: Goëau-Brissonnière et al. [26] established a vascular graft infection with S. epidermidis in dogs. After one week, infected infra-renal aortic grafts were replaced with replacement grafts, some of which were pre-treated with rifampin. They reported that all rifampin pre-treated replacement grafts had normal incorporation and were infection-free, while all untreated grafts were infected.
Cirioni et al. [18] tested daptomycin alone and in combination with rifampin against S. aureus infected PET grafts in rats. Both antibiotic agents were effective, and when combined, the authors concluded that daptomycin was especially valuable in preventing staphylococcal biofilm formation, and that rifampin served as an anti-staphylococcal antibiotic enhancer.
Darouiche et al. [25] showed in a rabbit model that subcutaneously placed minocycline/rifampin-coated vascular grafts have lower rates of staphylococcal device colonization and device-related infection than uncoated grafts. Aboshady et al. [28] developed a method of bonding three antimicrobial agents (rifampin, minocycline and chlorhexidine) to a vascular prosthesis against an infection with S. aureus, implanted in the abdominal aorta, and evaluated them in a porcine model. Compared with non-treated grafts, those bonded with antimicrobial agents were free of infection even eight weeks after implantation. The authors state that combining three antimicrobial agents that work with different mechanisms of action might reduce the risk for the development of resistances and might prolong the antibacterial activity even longer than eight weeks.
As mentioned earlier, rifampin has been used widely as an antimicrobial agent by numerous working groups for many years, proving to be effective alone or in combination with other antibiotic agents or antimicrobial agents, but mainly evaluated in vitro or in animal studies. We chose not to use rifampin in our experimental study, because we only performed a gram-positive infection, and it was not widely used in our department as an impregnation agent; we had evaluated it several years ago in vitro [15] and could prove that it was cytotoxic against endothelial cells and assumed that this might affect graft incorporation, when implanted in humans.
This is a finding that was supported recently by Moussavian et al. [29]. They studied the tissue incorporation of PET grafts coated with rifampin and showed that early peri-graft vascularization and incorporation were significantly affected by rifampin coating.
Daptomycin has been reported to be highly effective against gram-positive bacterial infections, also being able to inhibit organisms embedded in biofilms. It was approved in 2003 for the non-topical management of skin infections caused by gram-positive bacteria, including methicillin-resistant S. aureus, and in 2006 for the management of bacteremia [30].
We were able to establish an infection with S. aureus in each rabbit of our study that has not received a pre-treated graft. These infections were macroscopically visible through abscess formations on and around the patch and were confirmed with the microbiologic analysis after patch explantation. Antibiotic pre-treatment before implantation prevented abscess formation in all infected animals, confirming the excellent efficacy of daptomycin as an impregnation agent against gram-positive vascular graft infection in vivo.
Limitations
The animal model used in the present study may not be comparable directly with graft implantation into a blood vessel, especially because we have not created proximal and distal anastomoses, which are critical areas for the development of insufficiency of anastomoses or necrosis of the surrounding tissue. Furthermore, an infection in rabbits might not be comparable directly to the conditions in humans.
We did not establish a bacterial colonization with other bacterial strains on our vascular grafts. This limits our study results in terms of proving the same activity against different bacteria, nor did we test different antibiotic agents in vivo, which is another limitation of our study.
Further studies are required to test different prosthetic materials and different antibiotic impregnation agents, both in vitro and in vivo. Prophylaxis of vascular graft infection must be assessed in well-designed case-control studies, and their cost-effectiveness must be evaluated.
Conclusion
Our results show that antibiotic pre-treatment is a feasible option for the prevention of bacterial colonization on medical implants. Antibiotic pre-treatment does not interfere with surgical procedures, and daptomycin did not harm surgical site healing processes or the surrounding tissue. It is effective, simple, and quickly applicable to make it appropriate in the clinical setting.
The method presented in this study used only material available in the operating room, especially the antibiotic solution, which was prepared at the concentrations of generally available preparations, mimicking the clinical settings as much as possible. Furthermore, we believe that antibiotic pre-treatment should be evaluated further, especially in human conditions, and included into routine clinical practice whenever medical implants are used during surgical or interventional procedures.
Footnotes
Acknowledgments
We thank Heiner Gebauer from Laser Zentrum Hannover for help with the SEM-images and Dr. Erin Boyle for linguistic editing of the article.
Author Disclosure Statement
No competing financial interests exist.