
Abstract
Background:
The effect of an oral antibiotic preparation prior to colorectal surgery was first examined and exalted in the 1973 paper by Nichols et al. Since this commencement, enthusiasm for the oral antibiotic regimen has waxed and waned reflecting the literature focused on this topic over the past 40 years. Polling colorectal surgeons of define current practices has been performed at intervals throughout the years and has demonstrated a trend to decline in the practice. The most recent publication surveying U.S. practices was in 2010, which reported a minority, 36%, use of oral antibiotics prior to elective colorectal surgery; a marked downtrend from the 88% use described in 1990. Since this last survey, the colorectal surgery community has performed considerable research examining the benefit of oral antibiotic and mechanical bowel preparation. This manuscript evaluates the current use of oral antibiotics in colorectal surgery in the U.S. and how practice trends have developed in response to current recommendations in the literature.
Methods:
An electronic survey was created and distributed to U.S. colorectal surgeons to evaluate current opinions and practice trends. A total of 359 American Society of Colon and Rectal Surgeons members responded. A review of the recent literature pertaining to pre-operative bowel practices and outcomes was performed to compare with current practices.
Results:
A significant majority (83.2%) of respondents use pre-operative oral antibiotics routinely, and 98.6% routinely use mechanical bowel preparation. The use of a combination of parenteral antibiotics, oral antibiotics, and mechanical bowel preparation is reported by 79.3%. The most commonly employed oral antibiotic regimen is neomycin and metronidazole. The most common mechanical bowel preparation is polyethylene glycol (PEG). The most common parenteral antibiotics are cefazolin and metronidazole. There was no statistically significant difference in this practice by geographic region, Board-certified status, or practice setting.
Conclusion:
The majority of colorectal surgeons employ a combination of oral antibiotics, mechanical bowel preparation, and parenteral antibiotics prior to colorectal surgery. This is consistent across geographic regions, despite Board certification status or practice setting, and is reflective of the recommendations based on recent literature.
Oral antibiotics with poor enteral absorption were discovered in the mid-1900s [1–4] but were not recognized for their value in elective colorectal procedures until the 1970s. Shortly thereafter, intravenous (IV) antibiotics came into practice for preventing surgical site infections (SSIs) during elective colorectal procedures [5]. During this time interval, surgeons relied primarily on mechanical bowel preparation (MBP) to reduce the colonic bacterial load prior to surgery [6]. Nonetheless, site infection rates remained unacceptably high.
In an effort to decrease the high incidence of infectious complications, Nichols et al. examined the effect of an oral antibiotic preparation prior to colorectal surgery, reporting their findings in a landmark 1973 paper. This study concluded that the combined use of peri-operative oral antibiotics and MBP significantly reduced the colonic bacterial burden and resulted in significantly fewer incisional infections compared with MBP alone [7]. These findings were supported by a 1978 Veterans Affairs cooperative randomized trial in which the use of oral neomycin and erythromycin was linked to fewer infections and anastomotic leaks than were oral placebo and IV antibiotics [8]. Further support for oral antibiotic preparation came from a 1990 study that demonstrated the combination of mechanical bowel preparation with neomycin and erythromycin to be the most effective at suppressing both the intra-luminal and mucosal surface-associated microflora compared with mechanical preparation with and without parenteral cefoxitin [9]. Thus, a new practice was introduced that was adopted by the majority, and from the late 1970s to the 1990s, routine bowel preparative technique comprised MBP followed by oral neomycin and erythromycin [5].
Since this commencement, enthusiasm for the oral antibiotic regimen has waxed and waned, a reflection of the literature produced over the past 40 years researching myriad effects of oral antibiotics on septic sequelae and anastomotic complications.
The polling of colorectal surgeons to define current practices has been performed at roughly ten-year intervals, with the most recent publication surveying U.S. practices dated 2010, which revealed a dramatic decrease in the use of oral antibiotic preparation to a minority 36% [10]. Since this last survey, the colorectal surgery community has produced abundant literature examining the benefit of oral antibiotic and mechanical bowel preparation. Despite these data demonstrating the important role of peri-operative oral antibiotics and advocating routine use, there remains no official gold standard for this practice. The purpose of our study was to assess the current trends of American Society of Colon and Rectal Surgeons (ASCRS) members regarding bowel preparation prior to colorectal surgery.
Methods
An electronic survey was created and distributed to U.S. colorectal surgeons in an effort to evaluate current opinions and practice trends regarding bowel preparation before elective colorectal surgical procedures. A database of 3,206 E-mail addresses of ASCRS members was created. Of these addresses, 428 accessed the survey and were found to be active. Qualtrics Research Core software was used to create a 13-question survey comprising demographics, caseload, and both mechanical and antibiotic preparative techniques. Demographic data included four items regarding surgeons' geographic location, number of years in practice, and Board eligibility in colorectal surgery. Caseload data were obtained from three items regarding the majority of their cases, either general or colorectal surgery, the number of procedures performed on the colon and rectum each year, and the percentage of colorectal cases performed either laparoscopically or robotically. Bowel preparative technique was the focus of this survey, and these data were obtained from six items that addressed the use of oral and parenteral antibiotics, preferred mechanical cleansing procedures, as well as the motivation to use a bowel preparation. Individuals who did not use an oral antibiotic preparation answered an additional item in explanation (Fig. 1).
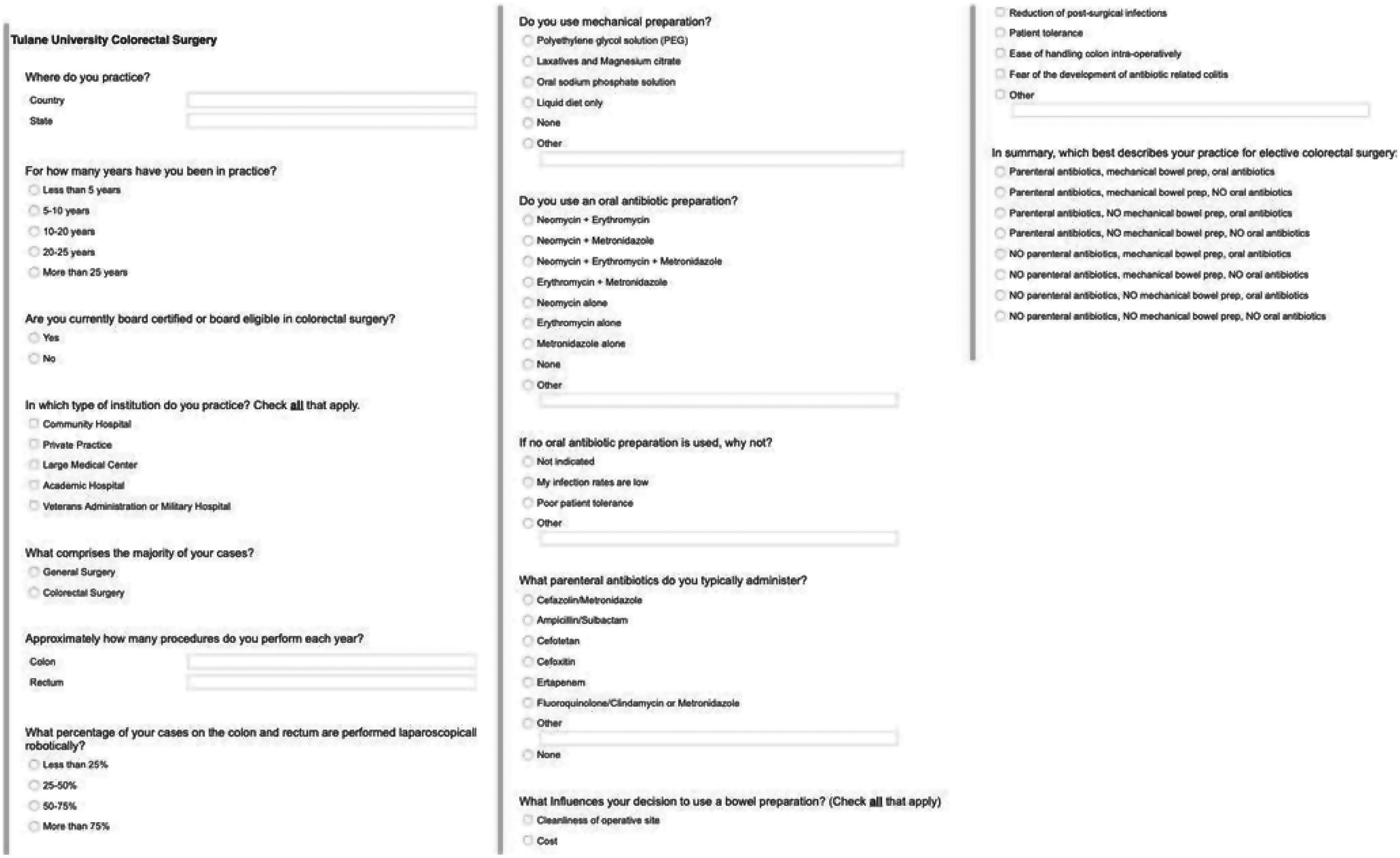
Sample of electronic survey distributed to U.S. colorectal surgeons.
“Oral antibiotic use” is defined for our purposes as the administration of oral antibiotics at intervals prior to surgery. “Mechanical bowel preparation,” in turn, is defined as purgative cleansing of the bowel, without use of oral antibiotics. Combined used of oral antibiotics and mechanical bowel preparation will be specified as such.
The questions were formatted as either multiple choice or open ended. The participants were encouraged to type a response next to the option “other” if none of the answer choices applied to their current practice.
The Pearson χ2 test and Fisher exact test were implemented in analyses. A p value <0.05 was considered statistically significant. All statistical analyses were conducted using SAS software (2013. SAS/ACCESS® 9.4 Interface to ADABAS; SAS Institute Inc., Cary, NC).
Results
Three hundred fifty-nine individuals completed the survey, for a response rate of 85% of active E-mails.
Demographics
The majority of respondents self-described as Board certified or Board eligible (91.5%), with colorectal surgery comprising the majority of their practice (90.2%). Twenty-six percent of participants reported greater than 25 years of practice (Table 1). Board certification status demonstrated no significant effect regarding utilization of a combination of parenteral antibiotics, oral antibiotics, and mechanical bowel preparation before surgery.
Characteristics of Respondents
Survey participants were asked to enter their state of practice, which was then categorized into regions: West, Midwest, North, and South, the breakdown of which was 18.9%, 23.6%, 23.6%, 33.8%, respectively. No significant difference in surgical practice, colorectal surgery versus general surgery, was noted among regions.
Regional comparison also was performed for the operative approach. Respondents were asked to classify the percent of their operations performed with minimally invasive approaches. Statistical significance was noted in a comparison of regions among surgeons who noted >75% minimally invasive approaches, with the West having a significantly greater percentage than the rest of the country; 75% versus 48.4%–61.5% (p = 0.01) (Table 2).
Practice Site, Procedure, and Bowel Preparation by Region
Abbreviation: MBP = mechanical bowel preparation; VA = Veterans Affairs.
Practice setting
A choice of practice setting, including academic hospital, community hospital, large medical center, private hospital, and VA hospital, was queried. The most common response among participants was “academic hospital” (Fig. 2). When comparing practice settings among regions, there was no statistically significant difference between regions (Table 2). When comparing utilization of a combination of parenteral antibiotics, oral antibiotics, and mechanical bowel preparation among different practice settings, there was no statistically significant difference (Table 3).
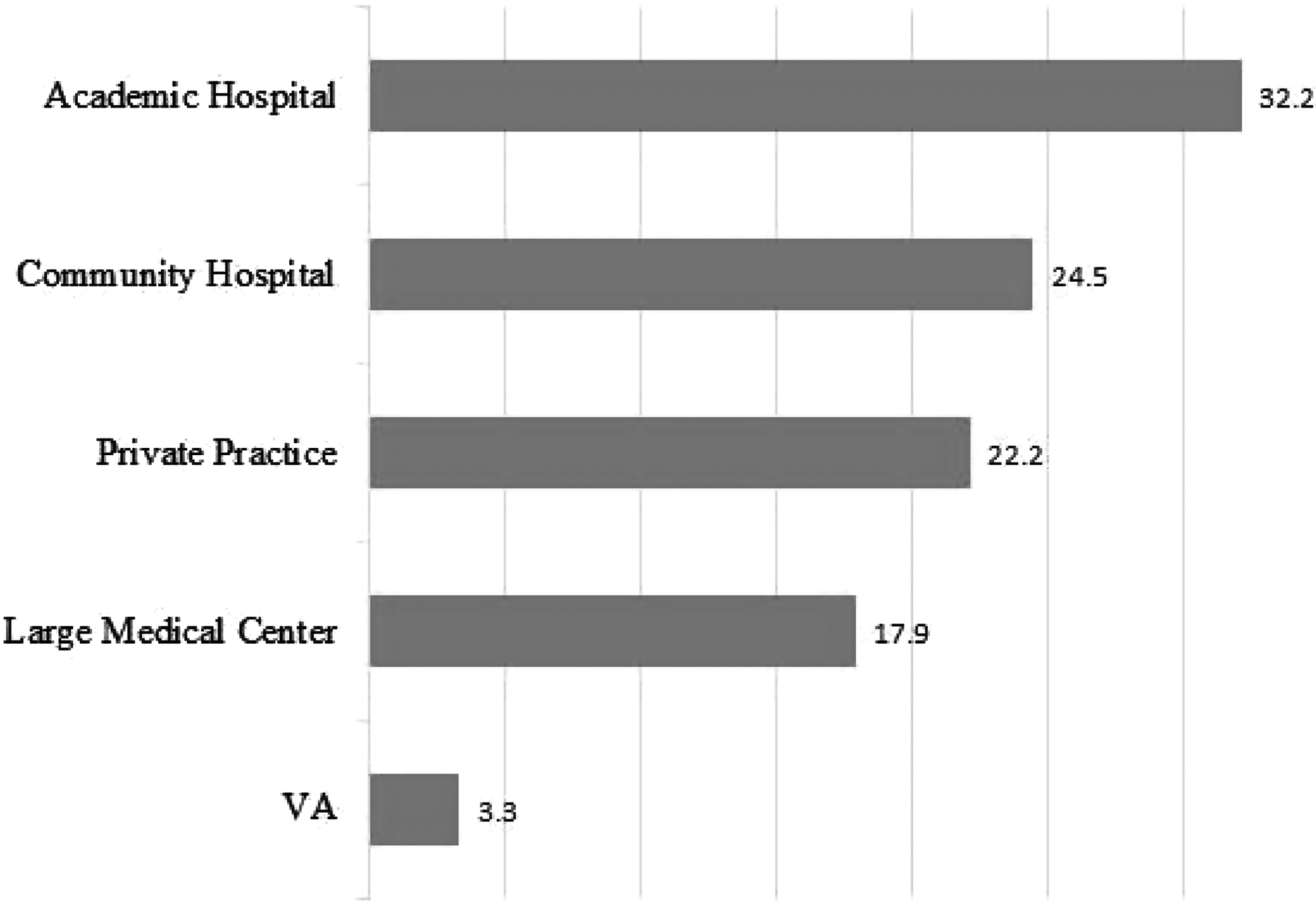
Respondent practice settings.
Board Status and Practice Site of Respondents
Choice of antibiotics
Survey participants were able to select a variety of factors influencing their decision to implement a bowel preparation. The most frequently selected factor was “reduction of post-surgical infections.” Respondents also were able to fill in their own answer regarding which factors influenced their bowel preparation habits. Frequently cited factors were hospital compliance guidelines and institutional enhanced recovery after surgery (ERAS) programs, the plan for a defunctioning ostomy, and the potential for on-table endoscopy for localization. For those not implementing oral antibiotic preparation before surgery, respondents were able to cite reasons such as “not indicated,” “poor patient tolerance,” and “my infection rates are low,” with the latter predominating at 32.8% among this subgroup.
Most respondents (83.2%) routinely use pre-operative oral antibiotics. A variety of antibiotics, both single agent and combinations, were available options on the survey. The most frequently selected was neomycin and metronidazole, at 58.4%, followed by neomycin and erythromycin at 15.4% (Fig. 3). This remained consistent between regions. Some respondents (16.8%) reported omission of oral antibiotics, ranging from 3.1% in the Midwest to 15.4% in the West.
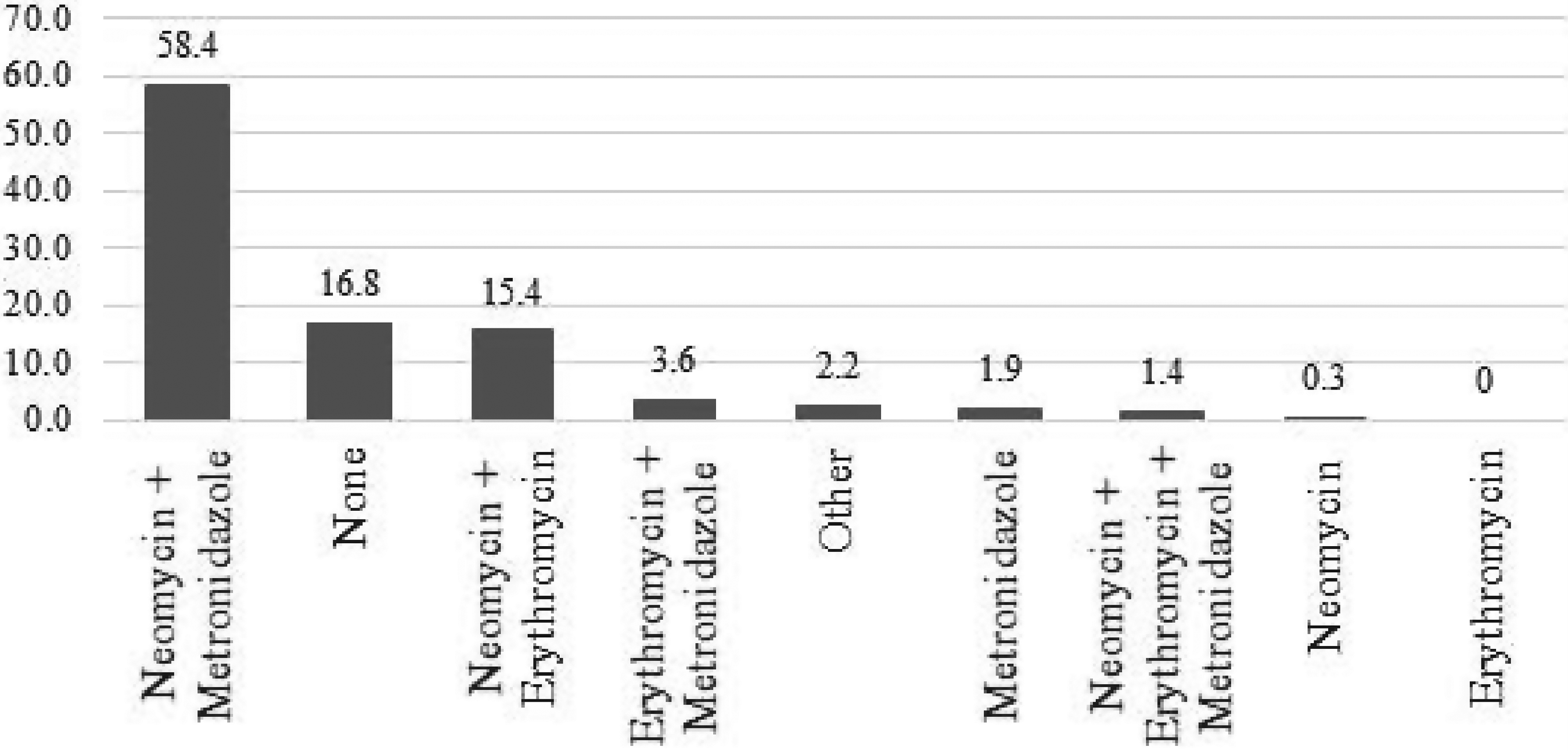
Oral antibiotic preparation utilized by respondents.
Use of a mechanical bowel preparation was described by 98.6%. The most common selection was polyethylene glycol (PEG), chosen by 62.7% of respondents (Fig. 4).
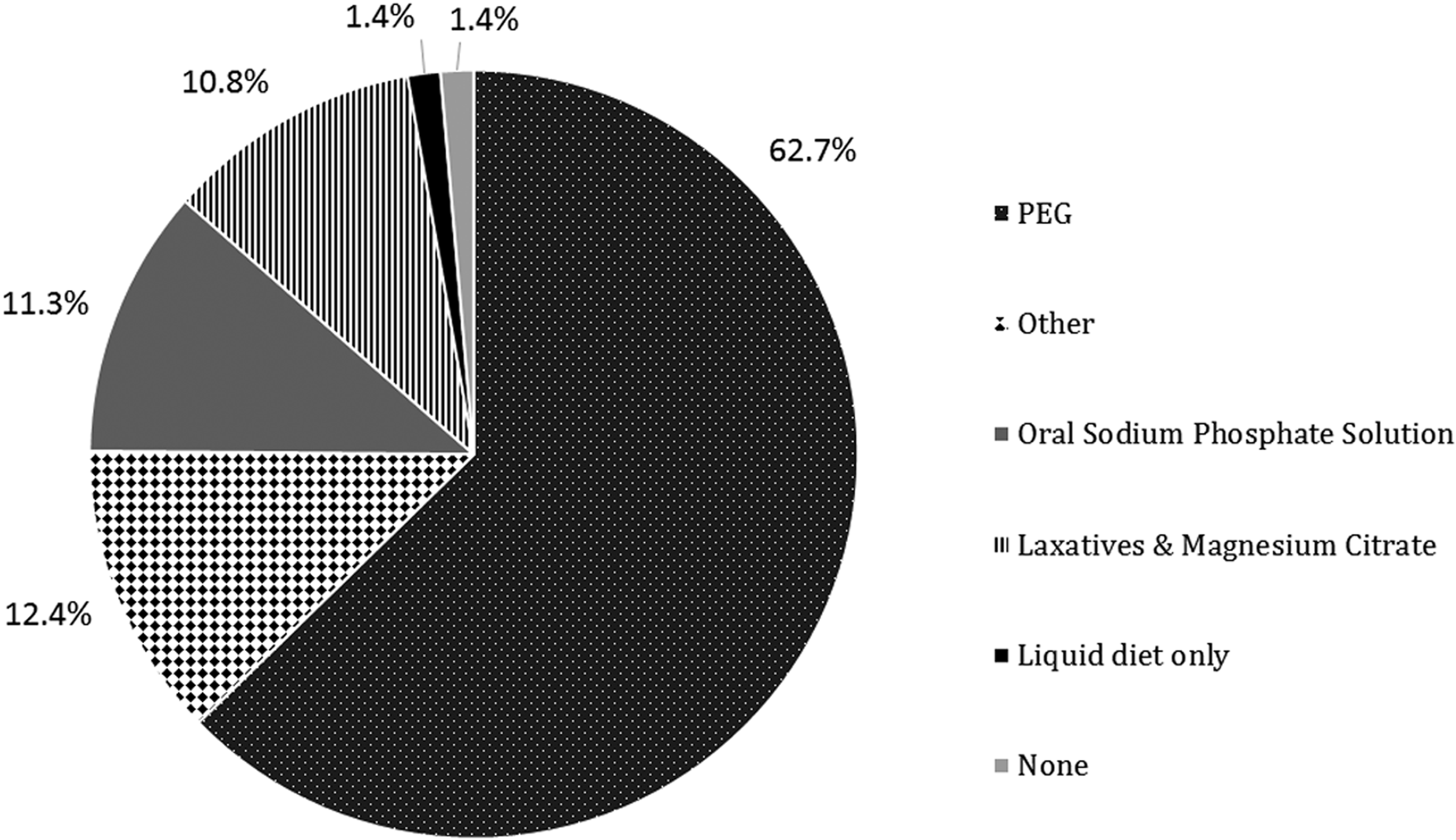
Mechanical bowel preparation utilized by respondents.
The survey reflected the most common parenteral antibiotics to be a combination of cefazolin and metronidazole (43.8%), with ertapenem (24.1%), cefoxitin (11.1%), and cefotetan (6.3%) following in succession (Fig. 5). A few respondents (9.4%) selected “other.” Each of these respondents further explained this answer with their preferred regimen, 24 of whom cited use of ceftriaxone and metronidazole, which comprised 6.6% of the total sample. When comparing by region, the South was found to prefer ertapenem over cefazolin-metronidazole, 37.6% and 33.3%, respectively.

Parenteral antibiotics utilized by respondents.
The use of a combination of parenteral antibiotics, oral antibiotics, and mechanical bowel preparation was 79.3% for the whole sample, while 14.1% reported use of parenteral antibiotics and mechanical bowel preparation without the administration of oral antibiotics. There were 2.5% employing parenteral and oral antibiotics without the use of a mechanical bowel preparation, and 3% reported use of parenteral antibiotics alone. The responses were assessed across regions as well. Consistent with the overall sample, the majority of respondents reported use of the combination, and there was no statistically significant difference in practice between regions (Fig. 6).
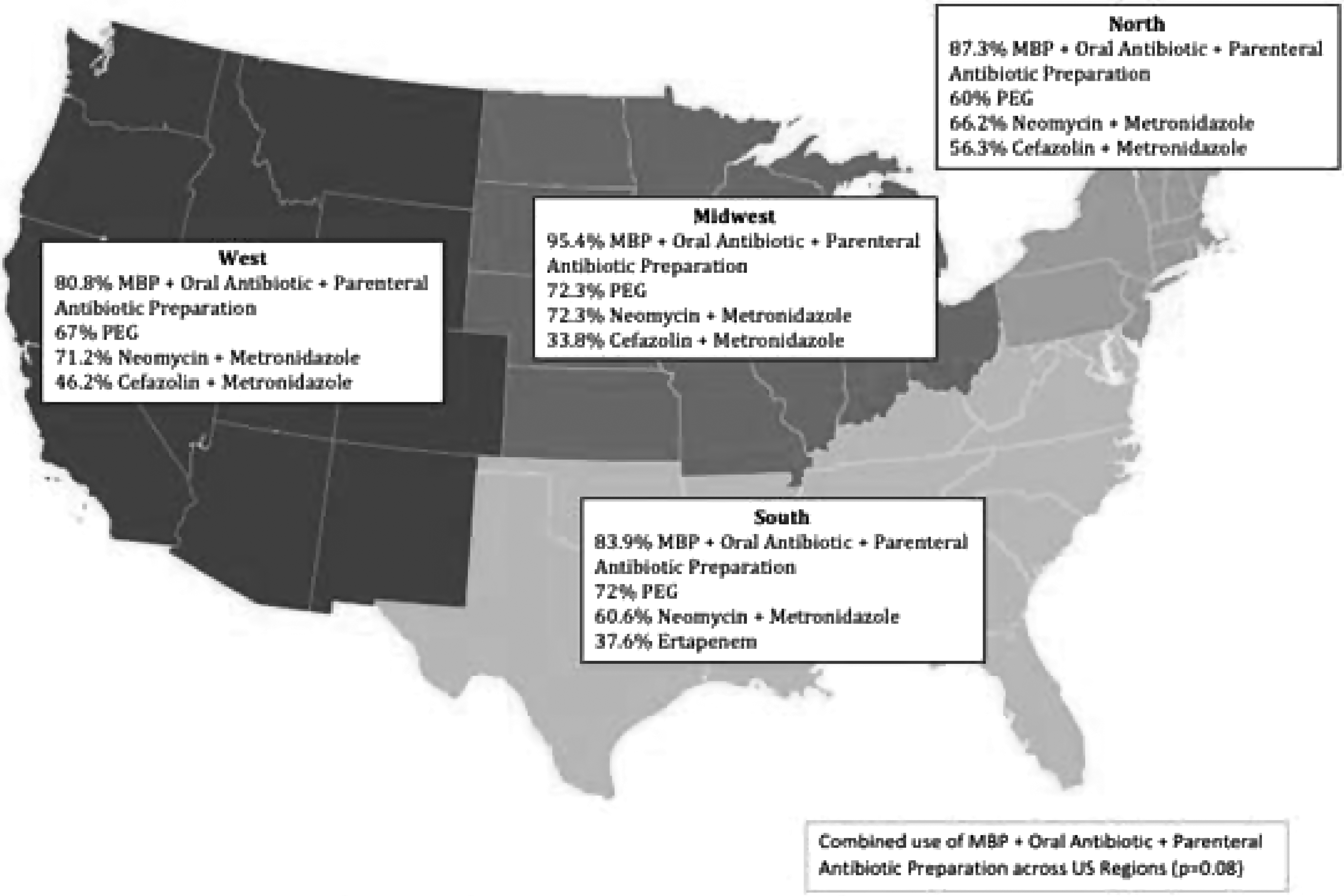
Map of U.S. regions with respective bowel preparation trends. Percent of respondents describing routine use of combined mechanical, oral, and parenteral antibiotics, as well as preferred regimens are described per region.
Discussion
Reducing the contamination of the peritoneum by colonic microflora during colorectal surgery is a well-accepted practice to reduce infectious and anastomotic complications. Although this practice is well-accepted in the literature, the optimal bowel preparation for elective colorectal procedures remains controversial.
The 1972 study by Nichols et al. compared the concentration of colonic and ileal aerobic and anaerobic bacteria after a variety of oral antibiotic preparations were administered with mechanical bowel preparation, as well as the concentration in the un-prepared colon. The results showed the largest suppression of both aerobes and anaerobes to be a result of treatment with neomycin and erythromycin. This study was performed by needle aspiration of the terminal ileum, cecum, and transverse colon of consenting patients undergoing an elective cholecystectomy. A stool sample also was utilized [11]. In a 1977 study, Nichols et al. reported on a group of volunteers who underwent mechanical bowel preparation in addition to the neomycin–erythromycin antibiotic preparation. This study showed maximum blood and fecal erythromycin concentrations were present when the antibiotics were given at 1
The benefit of neomycin–erythromycin in reducing the colonic bacterial load was further illuminated in the early 1990s when oral antibiotics were demonstrated to reduce both the luminal and the mucosal bacteria of the colon significantly [13]. The need for MBP prior to elective colorectal surgery began getting called into question at this time, as emergency surgery in an unprepared colon was observed to result in consistently good outcomes [14–19]. Consequently, oral antibiotics were omitted in many studies of elective colon surgery for the purpose of creating statistical significance and led to a decline in oral antibiotic usage in colorectal procedures at the turn of the 21st Century.
A subsequent steady decline in routine use of oral antibiotics among North American colorectal surgeons is reflected in the results of previous surveys of ASCRS members. A 1990 review of current U.S. and Canadian practices demonstrated an 88% use of mechanical and oral antibiotic bowel preparation prior to surgery, with the Nichols preparation predominating [20]. Similarly, in their 1997 survey, Nichols et al. found that 86.5% of surgeons used a combination of oral antibiotics and mechanical bowel preparation, with most surgeons using neomycin and erythromycin [21]. However, by 2003, routine use of oral antibiotic preparation dropped to 75%, as indicated by Zmora, et al. [22], followed by an even sharper decline to 36% reported in a 2010 survey. This survey also noted 55% of participants reporting never using an oral antibiotic preparation [10].
Comparison of our findings with the most recent survey, in 2010, demonstrates that colorectal surgeons have again embraced routine use of pre-operative oral antibiotics, with a rise from 36% to 83.2% (Fig. 7). This increase likely is reflective of recent research investigating outcomes after colorectal surgery as it relates to pre-operative bowel preparation. Scarborough et al. used the 2012 ACS–NSQIP participant use files to review the impact of oral and mechanical bowel preparation on infectious sequelae and anastomotic complications. They concluded that there was benefit to the co-administration of mechanical and oral antibiotic bowel preparation; however, their analysis reflects an overall minority 31.7% of their sample utilizing oral antibiotics [23]. Kiran et al. likewise examined the 2012 files and demonstrated a 27.5% use of combined oral antibiotic and mechanical bowel preparation in the sample they examined and deduced that the combined preparation was associated with a reduction in SSI, anastomotic leak, and ileus [24]. In a similar vein, Klinger et al. examined the 2012–2015 pooled ACS National Surgery Quality Improvement Program (NSQIP) files and demonstrated 37.9% use of combined mechanical and oral antibiotic preparation. This study demonstrated a significant reduction in incision complications, including infection and dehiscence, and anastomotic leak with combined preparation. The investigators also noted a lower rate of SSI using a combined preparation compared with oral antibiotic alone [25].
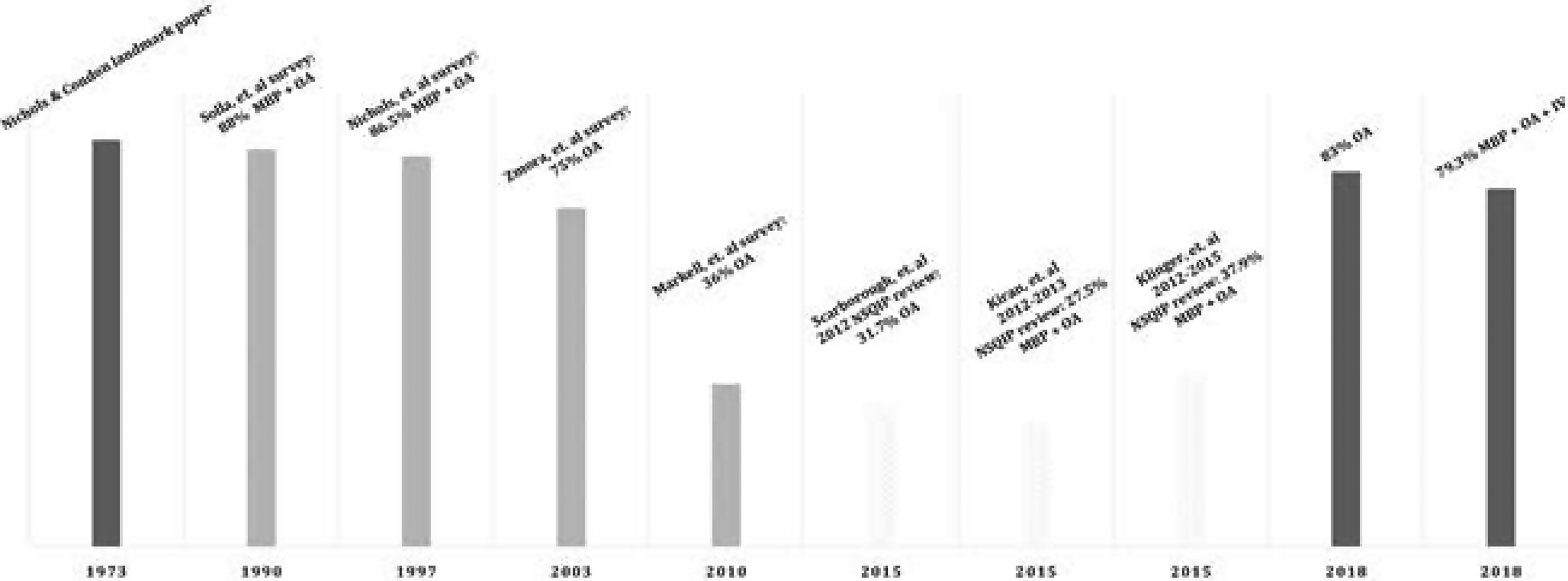
Trend of 50 years of surveys and publications on percent usage of oral antibiotics by surgeons in elective colorectal surgery.
Interestingly, our survey reports the most common oral and parenteral antibiotic regimens employed by U.S. colorectal surgeons to be, respectively, neomycin–metronidazole and cefazolin–metronidazole. In contrast, most other studies examining antibiotic practices prior to elective colorectal resection, including the 2013 Deierhoi study, reported neomycin–erythromycin and cefoxitin to be the most common oral and parenteral antibiotics [26].
The change in parenteral antibiotic preference follows recent literature that suggests IV cefazolin–metronidazole and IV ertapenem are associated with lower rates of SSI [27]. Although ertapenem is U.S. Food and Drug Administration approved for use in elective colorectal surgery, and we did note regional preference for ertapenem in this study, many experts advise against routine use of the drug for this purpose [28].
The discrepancy in oral antibiotic preference is much harder to define. Secondary analyses in two studies have demonstrated similar efficacy when an oral aminoglycoside is combined with either erythromycin or metronidazole [29,30].
Despite the evidence in the literature supporting combined oral and IV antibiotic regimens, as well as practice guidelines developed by the ASCRS strongly recommending the use of MBP with oral antibiotics for elective colorectal resections [31], surgeons are not universally accepting of this practice. One single-institution study showed that the addition of oral antibiotics to IV antibiotics and MBP for elective colorectal surgery provides no additional protection against SSI while contributing to poor patient tolerance in terms of nausea and vomiting [32]. Although this is contrary to the practice parameters stating that use of MBP without oral antibiotics is not recommended [31], gastrointestinal symptoms are a known side effect of erythromycin and could partly explain the shift in oral antibiotic preference from neomycin–erythromycin to neomycin–metronidazole [32].
However, the greater expense of erythromycin compared with metronidazole is proposed to be the main influence over antibiotic regimens prescribed by surgeons, with the former costing markedly more, 40-fold the price of oral metronidazole [33, 34]. Anecdotally, follow-up with several responders found that price was the main reason for the use of metronidazole rather than erythromycin.
Our study not only provides an update of current practice trends, it also demonstrates that these trends are consistent regardless of region of practice, which has never before been analyzed. However, there are several limitations to our study. A key one is that we analyzed a small sample of 363 total respondents. Although this is within the range of previous surveys, which studied 334–515 responses, it comprises a small percentage of the total colorectal surgeons in the U.S. In addition, our survey was concise, with only thirteen questions, and the benefit of brevity must be weighed against the drawback of lacking more detailed open-ended questions. Finally, we elected to survey only members of the ASCRS, which does not reflect the trend of colorectal surgeons who are not members of the society, nor the general surgeons performing colorectal procedures.
Footnotes
Conclusions
The results of this survey summarize the current practice trends of U.S. members of the ASCRS regarding pre-operative bowel preparation. Coincident with the ASCRS practice parameters, the results of our survey conclude that the majority of colorectal surgeons employ a combination of oral and parenteral antibiotics and mechanical bowel preparation prior to colorectal surgery. This is consistent across U.S. regions, with no difference according to Board certification status or practice setting, and is reflective of current recommendations based on the recent literature. Divergent from previous surveys, our findings demonstrate oral metronidazole to predominate over erythromycin. To our knowledge, no studies have been conducted comparing the two oral antibiotics. To further complicate this matter, no studies seem to have been done to define the optimal administration doses and times of metronidazole to have an optimal effect on the colonic mucosal flora. In an effort to define a specific antibiotic regimen, further investigation into the effect of metronidazole on intra-luminal and mucosal associated bacteria is suggested.
Author Disclosure Statement
No competing financial interests exist.