
Abstract
Background:
The burden of surgical infections in low- and middle-income countries (LMICs) remains poorly defined compared with high-income countries. Although there are common infections necessitating surgery prevalent across the world, such as appendicitis and peptic ulcer disease, other conditions are more localized geographically. To date, comprehensive assessment of the burden of surgically treatable infections or sequelae of surgical infections in LMICs is lacking.
Methods:
We reviewed the literature to define the burden of surgical infections in LMICs and characterize the needs and challenges of addressing this issue.
Results:
Surgical infections comprise a broad range of diseases including intra-abdominal, skin and soft tissue, and healthcare-associated infections and other infectious processes. Treatment of surgical infections requires a functional surgical ecosystem, microbiology services, and appropriate and effective antimicrobial therapy. Systems must be developed and maintained to evaluate screening, prevention, and treatment strategies. Solutions and interventions are proposed focusing on reducing the burden of disease, improving surveillance, strengthening antibiotic stewardship, and enhancing the management of surgical infections.
Conclusions:
Surgical infections constitute a large burden of disease globally. Challenges to management in LMICs include a shortage of trained personnel and material resources. The increasing rate of antimicrobial drug resistance, likely related to antibiotic misuse, adds to the challenges. Development of surveillance, infection prevention, and antimicrobial stewardship programs are initial steps forward. Education is critical and should begin early in training, be an active process, and be sustained through regular programs.
The burden of surgical infections in low- and middle-income countries (LMICs) remains poorly defined compared with high-income countries (HICs) [1]. Whereas there are common infections necessitating operations prevalent across the LMIC world such as appendicitis and peptic ulcer disease associated with Helicobacter pylori, other conditions such as leishmaniasis or filariasis are more localized geographically. Surgical infections require a combination of effective operative management as well as proper antimicrobial therapy. The purpose of this review is to summarize current understanding of global infectious diseases treated by operations, as well as the infectious sequelae of invasive procedures (Fig. 1).
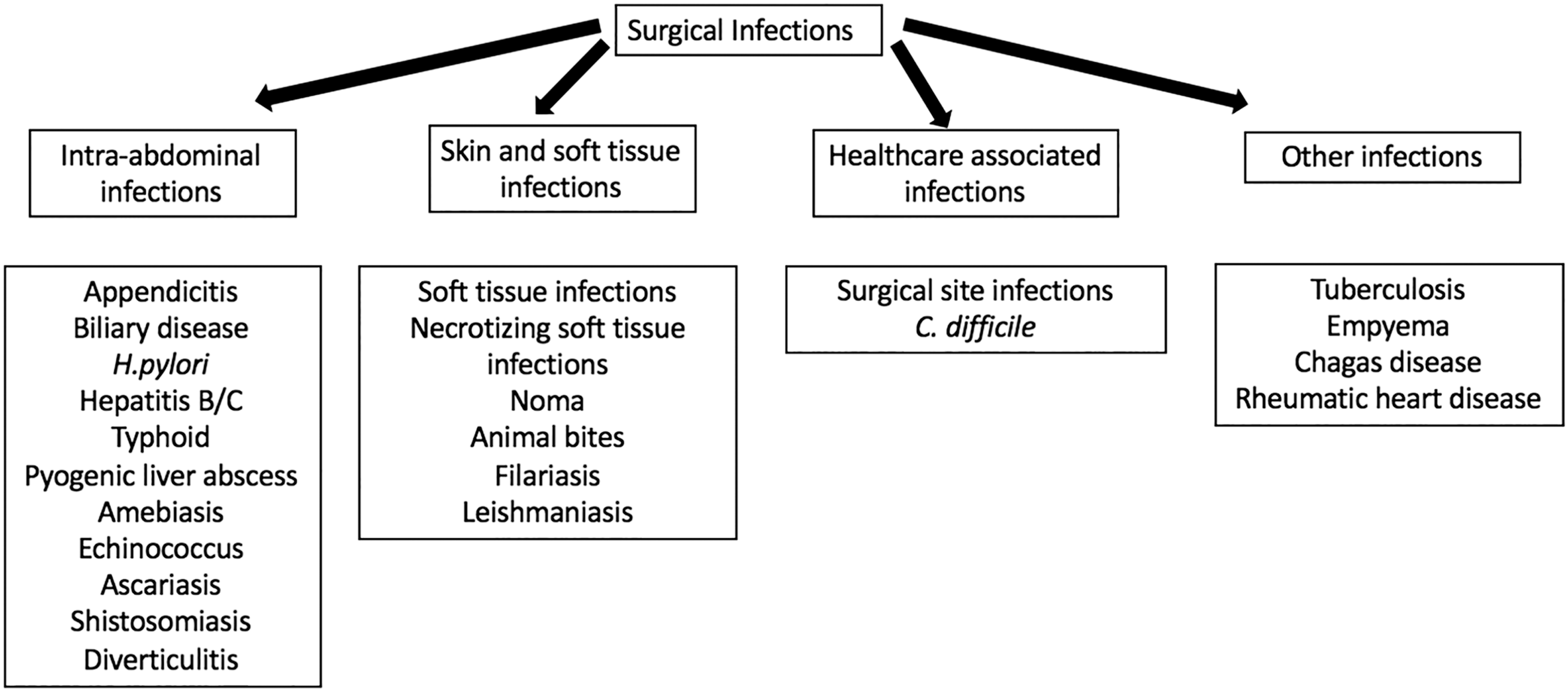
Surgical infections in low- and middle-income countries.
Burden of Surgical Infectious Disease in Low- and Middle-income Countries
To our knowledge, there has been no comprehensive assessment of the number of operatively treatable infections or sequelae of surgical infections in LMICs. Existing global estimates of surgical needs such as the World Health Organization (WHO) Global Burden of Disease Program (GBD) do not categorize many infectious pathologies necessitating operative intervention independently, despite infections clearly being “any pathology for which an invasive procedure may provide treatment, palliation, or cure” [2]. To the extent possible, we provide a summary of current estimates of surgical infectious disease in LMICs, defining surgical infections as any infectious process requiring operative intervention or any infection caused by an operative process (Table 1).
Surgical Infections and Operative Interventions
Intra-Abdominal Infections
Appendicitis
In 2017, the global incidence of appendicitis was 19 million [3]. In 2010, appendicitis resulted in an equivalent number of deaths in LMICs and HICs but was associated with considerably more years of life lost and disability-adjusted life-years [4–6]. Studies from LMICs have shown population frequencies of appendicitis that are lower than, or comparable to, that in HICs [7–10]. In LMICs, appendicitis tends to present later in the natural history of the disease, frequently with gross perforation [6,11–13] that may contribute to the elevated surgical site infection (SSI) rates (17.9%) seen with appendectomy in LMICs [13]. Although the utility of non-operative management of uncomplicated appendicitis has been documented, most cases of appendicitis, especially complicated disease, are managed with appendectomy [14].
Biliary disease
In 2017, the global prevalence of nononcologic biliary disease was 30.6 million [3]. Each year, 3%–4% of U.S. patients with gallstones undergo operation, making it the most common elective abdominal procedure [15]. Reported morbidity and mortality rates associated with biliary disease are considerably lower in LMIC settings. As the Western diet and lifestyle become more common in LMICs, however, it is possible this trend will reverse; and cholesterol gallstone disease resulting in cholecystitis will become more common [16,17].
Helicobacter pylori and peptic ulcer disease
In 2017, the prevalence of peptic ulcer disease (PUD) was 17.2 million [3]. In 2015, 60% of the world's population (an estimated 4.4 billion individuals) were infected with H. pylori [18]. Considerable regional variation has been noted, with a greater prevalence of disease in Africa, South America and the Caribbean, and Asia [18,19]. Untreated, long-term infection with H. pylori may lead to PUD in 10% of patients with 1%–3% developing gastric adenocarcinoma [20,21]. Indications for operative intervention in PUD include bleeding, perforation, obstruction, and intractable disease. Peptic ulcer disease is the leading cause of disability and death among all indications for emergency general surgery in LMICs, with 85% of PUD-related deaths occurring in such countries [4,5,22].
Hepatitis B and C and hepatocellular carcinoma
Hepatitis B virus (HBV) has been estimated to infect between 240 million and 350 million persons worldwide, with much of the burden of disease falling on LMICs, the Asia Pacific and sub-Saharan Africa regions in particular [23–27]. Of the 786,000 HBV-associated deaths in 2010, 341,000 (43%) were attributed to hepatocellular carcinoma (HCC). Similarly, hepatitis C virus (HCV) was estimated to infect 185 million persons worldwide in 2005, with the highest prevalence (>3.5% infected) in Central and East Asia and North Africa and the Middle East [28]. Infection with HCV increases the risk of HCC 15–20-fold by inducing fibrosis and cirrhosis [29]. Two thirds to 80% of HCC occurred in the Western Pacific or sub-Saharan Africa, where liver carcinoma is the fourth most common type of cancer [4,25,30]. It is not known how many of these patients with HCC underwent, or could have undergone, operation [31–33]. In Africa, the incidence of HCC correlates closely with the fatality rate, suggesting late diagnosis, few available therapeutic options, or both [30,33].
Typhoid intestinal perforation
In 2000, an estimated 21 million cases of typhoid fever and 216,000 deaths occurred worldwide [34]; this increased to 26.9 million cases annually as of 2010 [35]. More than half of the cases of typhoid fever are estimated to occur in LMICs, although the figure may underestimate grossly the number of infections in endemic settings [36]. Salmonella typhii, the causative agent of typhoid fever, can be found in the Peyer's patches in the small bowel and can sequester in the gallbladder. Among seven national-level studies reporting secondary outcomes of typhoid fever, intestinal perforation rates ranged from 0–4% [36]. Management of typhoid intestinal perforation is operation for bowel repair and source control. The overall case fatality rate is 15% [37].
Pyogenic liver abscess
The frequency of pyogenic liver abscess differs considerably by region [38]. Historically, the most common cause of a pyogenic liver abscess has been appendicitis, although this has changed over time to cholecystitis [39,40]. There are no recent national- or regional-level epidemiologic studies of pyogenic liver abscess in developing countries. In the U.S., it is responsible for 2.3 hospital admissions per 100,000, increasing to 275 per 100,000 admissions per 100,000 in Taiwan [38].
Management of pyogenic liver abscess centers on treating the underlying cause, drainage of abscesses, and systemic antibiotic therapy. Drainage can be accomplished through percutaneous, interventional, laparoscopic, or open means [41]. Small abscesses (<3–5 cm) usually resolve with appropriate antibiotics without operative intervention; larger abscesses (>5 cm) may be served best by operative drainage.
Amebiasis
In 1986, an estimated 10% of the world's population was estimated to be infected by Entamoeba histolytica, with only 1% of infected individuals experiencing invasive disease [42]. These values now are believed to be overestimates as a consequence of separation of the pathogenic species E. histolytica from the non-pathogenic Entamoeba dispar [43]. Operation may be required for complications of primary infection such as perforation, stricture, or bleeding of the intestine. Between 3%–6% of patients progress to fulminant amebic colitis necessitating operative intervention with a mortality rate ranging from 57%–100% [44–46]. Amebic liver abscess, occurring in ∼1% of infections, also may require operative intervention [47,48].
Echinococcus
In 2007, 4 million persons worldwide were estimated to be infected with Echinococcus granulosus or Echinococcus multilocularis, the causative organisms of cystic echinococcosis and alveolar echinococcosis, respectively [49]. In 2010, 1,200 deaths were attributed to echinococcosis [4,5,49]. Operative resection of cysts and cystic lesions is a mainstay of treatment. Although anti-helminthic chemotherapeutic regimens may result in cure rates of 30% or more, nearly 70% of infected patients will benefit from operative intervention [49].
Ascariasis
Ascariasis is a common helminthic infection worldwide, with nearly 25% of the world's population infected [50]. No existing population-based studies examine the frequency of operative disease among infected persons. However, operative pathology attributable to ascariasis is well-described and includes appendicitis, Meckel's diverticulitis, volvulus, intestinal obstruction, intussusception, perforation, and biliary and pancreatic obstruction [7,51–54].
Schistosomiasis
More than 200 million people worldwide are infected with Schistosoma [55]. Acute operative conditions such as appendicitis, Meckel's diverticulitis, and cholecystitis in endemic regions are rarely described [7,56–59]. More common chronic conditions amenable to operation are bladder cancer [60] and portal hypertension [61–63].
Liver flukes
Infection with Clonorchis sinensis results after ingestion of raw fish contaminated with infective cysts. An estimated 15–20 million people globally are infected [64]. Rarely, infection can necessitate operative intervention for acute processes such as obstructive jaundice, cholangitis, or cholecystitis [65–71]. Other indications for operative intervention are sequelae of chronic infection such as mucinous cystadenoma [72] or cholangiocarcinoma [64]. Similarly, Fasciola spp. liver flukes are estimated to infect 2 million individuals worldwide and cause biliary ductal dilation and other biliary pathology [73–78].
Oesophagostomiasis
Oesohagostomiasis is caused by worms of the family Strongylidae (Oesophagostomum bifurcum, O. apiostomum, and O. stephanostomum among others), which is characterized by acute abdominal pain mimicking appendicitis, intestinal obstruction, painless cutaneous masses in the lower abdomen, and, rarely, bowel perforation [79]. These worms are endemic or potentially endemic in 36 countries predominately in Africa, South America, and southeast Asia and infest approximately 250,000 persons whereas more than 1,000,000 persons are at risk of infestation [80–83]. The anti-helminthic drug albendazole is the mainstay of treatment [84]. Surgeons may be involved in cases of misdiagnosis or if there are complications of nodular disease such as bowel obstruction, peritonitis, or intestinal volvulus.
Cytomegalovirus perforation
Cytomegalovirus (CMV), a member of the Herpesviridae family, usually is acquired in childhood [85]. The estimated global seroprevalence is 83%, although this may be even higher in lower-resource settings such as Africa and Southeast Asia [86,87]. Infants, recipients of solid organ transplants, and other immunosuppressed patients, particularly those with human immunodeficiency virus (HIV) who have a CD4 count <50 per mm3 are at greatest risk of clinical sequelae of infection [85,88]. Gastrointestinal manifestations have been found to affect <1%–14% of HIV-infected patients in Africa, although rigorous epidemiologic studies of CMV infection among persons living in LMICs are limited [87–89]. Complications likely to be encountered by surgeons are colitis, gastritis, esophagitis, duodenitis, pancreatitis, peritonitis, intestinal perforation, and splenomegaly. Epidemiologic assessments of the surgical burden of CMV infection in LMIC settings are lacking.
Diverticulitis
Historical accounts from surgeons in LMICs rarely identify diverticulitis as an indication for operation [90]. Few population-based estimates of diverticular disease exist for diverticulitis in LMICs, and those that do are single country or single institution [22,91–93]. As diets and lifestyle patterns change, an increase in diverticulitis in LMICs may be anticipated [91–93].
Skin, Soft Tissue, and Bone Infections
Extremity soft tissue wounds may be attributable to a wide range of etiologies, including vascular disease, diabetes, and trauma. Any trauma or wound, particularly those poorly managed, may progress to skin and soft tissue infection. There are no estimates of the number of skin and soft tissue infections in LMICs. Soft tissue infections are associated with 1.5 times the number of deaths in LMICs as in HICs, with concomitantly greater years of life lost and disability-adjusted life-years [22].
Trauma
The burden of infection after traumatic injury is considerable in LMIC settings. There are more than 4 million fatalities annually from traumatic injury, with 88% of injury-related deaths occurring in LMICs [4,94,95]. The true incidence of skin or soft tissue infection after traumatic injury in LMIC countries has not been defined. However, evaluation of infection after orthopedic fixation of traumatic fractures is not particularly encouraging. Skin and soft tissue infections after operative fixation of open fractures is common in LMIC settings, with rates up to three times those found in HIC settings [96].
Osteomyelitis
Although osteomyelitis may occur after injuries or other soft tissue infections and represents a large healthcare burden in LMICs, to our knowledge, there are no population-level data. In Ugandan hospitals, osteomyelitis accounted for 10% of all operative procedures [97]; little data exist beyond individual facility reports, and GBD does not provide any assessment of this condition. A review of infections after open reduction and internal fixation of long bones for trauma in LMICs identified an infection rate of 6.4 per 100 procedures; open fractures had an infection rate of 18 (95% confidence interval [CI] 13.9–23.0) infections per 100 procedures [96]. A high incidence of road traffic collisions coupled with personnel, facility, and other resource challenges limit the ability to render timely and definitive fracture management, contributing to this burden. In fracture management, early washout of open fractures and internal or external fixation allows earlier return to ambulation, function, work, and independence. If antibiotic administration, washout, and fixation of open fractures are not performed in a timely fashion, the risk of non-union and acute and chronic osteomyelitis is significant.
Diabetes mellitus and peripheral vascular disease
There are 496 million people globally with diabetes mellitus and 118 million people globally with peripheral arterial disease (PAD) [3]. The prevalence of PAD in sub-Saharan Africa may be equal to or higher than that in HICs, exceeding 50% in some high-risk populations [98]. The prevalence of PAD ranges from 3%–24% in adults age older than 50 years. The prevalence is even higher (39%–52%) in persons with known risk factors such as diabetes mellitus [98]. The number of persons affected worldwide is expected to double by 2030, with an anticipated 485 million people affected. This increase will affect LMICs disproportionately, with nearly two thirds of all new cases originating in these countries [99]. Common complications of diabetes mellitus are peripheral neuropathy and peripheral vascular disease, which can lead to diabetic foot infections. These infections require operative debridement and potentially amputation. The number of associated skin and soft tissue infections anticipated with a global increase in chronic diseases including peripheral vascular disease and diabetes has not been quantified but likely will be substantial.
Necrotizing soft tissue infections
Necrotizing soft tissue infections, including necrotizing fasciitis and Fournier's gangrene, may occur as a result of untreated soft tissue infections or de novo. There are few existing country- or regional-level studies assessing the burden of necrotizing soft tissue infections in LMICs, with most studies retrospective, descriptive, hospital-level assessments or compilations of case reports [100,101].
Bites/Stings/Venom
Animal bites are a common problem in LMICs and may require operative management or surgical consultation. There is no global estimate of the total annual number of animal–human bite injuries, although the burden may be considerable in rural and agricultural settings [102]. Globally, 44 million people are injured or diseased as a result of contact with animals [3] Dog bites are estimated to account for 76%–94% of bite wounds in LMICs [103]. High-risk bite features for which antibiotics should be administered include bites to areas with compromised venous or lymphatic drainage, bites to the hand or a prosthetic joint, bites of patients with diabetes mellitus or who are immunosuppressed, crush injuries, or delayed presentation [104].
Cat bites are the second most common animal bite worldwide, accounting for 2%-50% of bite injuries [103]. Because cat bites tend to be at high risk of secondary infection, antibiotic prophylaxis is recommended, in addition to consideration of the rabies post-exposure prophylaxis, tetanus toxoid, and local wound care necessary for all animal bites [102, 104].
In some settings, monkeys may be responsible for 2%–20% of bites [103]. For certain species of macaque monkeys, the risk of herpes B infection should be considered; this rare virus is nearly uniformly fatal for humans if not treated early [105].
Approximately 5 million snake bites are estimated to occur annually, the majority occurring in Africa and southeast Asia [103]. Infections after a snakebite have been reported to affect 9%–35% of victims [106, 107].
Lymphatic filariasis
Lymphatic filariasis, caused by Wuchereria bancrofti, Brugia malayi, and Brugia timori, affects between 67 to 120 million people worldwide [108,109]. Most of the burden falls on LMICs in Asia, Latin America and the Caribbean, and sub-Saharan Africa [110]. Although acute infection is treated with anti-filarial drugs, chronic stigmata of infection such as hydrocele, lymphedema, and elephantiasis may require operative intervention [109,111,112]. Approximately 37% of infected personsin historical analyses experienced hydrocele, although this frequency is likely lower today given improved surveillance and treatment [110].
Leishmaniasis
Infection with Leishmania spp. can cause several clinical syndromes. Cutaneous leishmaniasis, caused by Leishmania tropica, is estimated to affect 0.7 million–1.2 million persons per year and is an endemic disease in many LMICs [113]. Operative excision of lesions has been used as an adjunct to anti-protozoal treatment [114–116]. Visceral leishmaniasis, also known as kala-azar, is caused by Leishmania donovoni and Leishmania infantum and affects approximately 200,000–400,000 persons per year [113]. Although operative intervention rarely is needed, it has been utilized in cases resistant to, or relapsing from, treatment with anti-protozoal drugs, particularly in immunosuppressed individuals with HIV [117–123].
Noma (gangrenous stomatitis, cancrum oris)
Noma is rapidly progressive, severe gangrene of the face and mouth commonly caused by a polymicrobial infection including with Fusobacterium necrophorum and Prevotella melaniogenica [124]. This infection typically affects children age three to 10 years living in poverty in sub-Saharan Africa [124]. In 1998, the WHO estimated that 140,000 children contract noma each year, predominately in a geographic region represented by a belt across western and central Africa [125]. This is likely an underestimation of the true incidence, as fewer than 10% of affected children seek care during an active infection [126,127]. Most cases (70%–90%) are fatal [128]. Operative management consists of wound care in the acute phase. In patients who survive the infection, reconstructive surgery may be required.
Healthcare-Associated Infections
Surgical site infections
Worldwide, SSIs occur in 2%–20% of patients after operation, and the rate differs according to the environment in which operations are performed, local resources, and a number of patient- and surgery-related factors. Rates are likely higher in LMICs, and one study has shown as much as a 20% SSI rate in women in Africa who have cesarean sections [129].
Surgical site infections are the most common infectious complications among hospitalized patients in developing countries, with a pooled cumulative incidence of 5.6 infections per 100 surgical procedures [130]. The incidence differs depending on the degree of incision contamination. The largest prospective evaluation of SSI after gastrointestinal resection identified 12,539 patients from 343 hospital in 66 countries [131]. The incidence after gastrointestinal resection was lowest among high HICs (9.4%) and higher among middle-income countries (MICs)(14%) and low-income countries (LICs) (23%) [131]. Patients from LICs had the greatest risk of SSI, irrespective of the degree of intra-operative contamination (adjusted odds ratio [AOR] 1.60 [95% CI 1.05–2.37; p = 0.030]). Furthermore, the African Surgical Outcomes Study noted that infection was the most common post-operative complication, with an overall rate of 10.2% (1,156 of 10,970 patients), and the rate of death linked to infection was 9.7% (n = 112) [132].
Cesarean section is the most common major surgical operation in many countries, with an estimated 29.7 million performed in 2015 [133,134]. Higher cesarean delivery rates may lead to increases in maternal morbidity and death, as cesarean sections are associated with a five-fold to 20-fold increase in the risk of infection compared with vaginal delivery [135]. A recent meta-analysis noted that 23.8% of women dying after childbirth in these settings had had a cesarean section [136]. The rate of SSI after cesarean section differs globally, ranging from 3%–11% in HICs to 3%–24% in LMICs [137–139]. Surgical site infections result in prolonged hospitalization and a greater burden on resource-limited facilities and environments [133,140]. However, a recent study of post-cesarean SSI rates in four sub-Saharan African countries show results comparable to those in HIC, indicating standardized protocols, peri-operative antibiotics, instrument sterilization, and incision care can be achieved in a low-resource setting [140]. In LMICs, where quality measures are not available or are difficult to assess, post-cesarean SSI could be a proxy for the quality of surgical care.
Variability among the rates of SSI after different surgical procedures and between techniques for the same procedure may not be captured or assessed in these larger cross-sectional studies. For example, the weighted, pooled infection rate after appendectomy was 17.9% in LMIC settings. However, in that review, 90% of appendectomies were performed in an open fashion [13]. Among 6,224 intra-medullary nails implanted, infection rates of 3.5% (CI 3.0–4.1) and 7.3% (CI 6.2–8.4) were observed for femoral or tibial fractures, respectively [141]. Pooled analysis of 31 studies from LMICs where mesh was used for inguinal hernia repair identified an infection rate of 4.1% (CI 2.9–5.4) [142]. The weighted, pooled infection rate after sternotomies in LMICs was 4.3%, which is within the range reported in HIC ecosystems [143]. This similar infection rate after sternotomy may reflect the infrastructure and process management necessary to perform complex cardiac procedures safely, irrespective of the human development index status of a country.
Clostridioides difficile colitis
Clostridioides difficile is a common cause of gastroenteritis among hospitalized patients and one of the most common causes of health-care–associated infections in the U.S. [144]. Operative intervention is a cornerstone of therapy for severe, fulminant C. difficile infection [145]. The burden of these infections in LMICs remains poorly understood, with few national-level estimates [146,147].
Other Infections
Tuberculosis
Nearly one quarter of the world's population is infected with, or has been exposed to, Mycobacterium tuberculosis, the causative agent of tuberculosis (TB) [148], with the greatest burden in LMICs [149,150]. In 2016, more than 1.7 million deaths were attributable to this infection [148]. Operations may be required for both pulmonary and extra-pulmonary TB [151–153]. Operative interventions for pulmonary TB may involve chest tube placement, thoracotomy and decortication, lung resection, or Eloesser flap construction. Operative intervention for multi-drug–resistant pulmonary TB may be cost-effective in LMICs as long as there is adequate surgical expertise, facilities, and diagnostic capacity [154,155]. Operative management of extra-pulmonary TB may include biopsy for diagnosis, laparotomy for obstruction or perforation, or spine surgery for Pott's disease.
Empyema
Empyema may develop as a result of a bacterial or viral pneumonia, TB, retained hemothorax after trauma, or iatrogenic injury. There is no global estimate of the incidence of empyema, although the burden likely is considerable, as lower respiratory tract infections are the leading infectious cause of death worldwide [156]. Pneumococcal and Haemophilus influenzae pneumonia are responsible for more than 99% of all pneumonia deaths in LMICs [5,156,157]. Approximately 20%–57% of patients with bacterial pneumonia will develop a parapneumonic effusion, and of these, 5%–10% will progress to frank empyema [158]. Operative interventions may include chest tube placement, thoracotomy and decortication, or Eloesser flap.
Chagas disease
Chagas disease is caused by the parasite Trypanosoma cruzi, transmitted principally to human beings through bites of the Reduviid bug or through transfusion. An estimated 8 million people are infected with T. cruzi worldwide, with most infections occurring in South and Central America [159]. Operation may be indicated in the chronic phase, which can affect the gastrointestinal tract causing mega-colon and mega-esophagus (10% of infected patients) or the heart, resulting in dilated cardiomyopathy (30%) [160–162].
Rheumatic heart disease
Group A streptococcal infection can lead to rheumatic fever, which can in turn cause rheumatic heart disease. The disease is characterized by autoimmune-mediated, progressive heart valve damage, which can lead to cardiac failure [163]. The mitral valve is most commonly affected [164]. Rheumatic heart disease is estimated to affect 15.6–33.4 million people worldwide, with most of these infections occurring in LMIC [165]. Operative therapeutic options are mitral commissurotomy, valve repair, or valve replacement [164].
The Surgical Ecosystem
Not only are comprehensive surgical infection data lacking, existing data on available surgical workforce and capacity are limited and fragmented, particularly in LMICs. According to the best estimates, 5 billion persons lack access to timely and safe surgical care [166]. This crisis is magnified in LMICs, where two thirds of the poorest countries are the site of only 6.5% of all operations performed [167]. The global number and distribution of surgical providers remain poorly assessed [168]. Efforts to build a WHO surgical workforce database to quantify surgical providers by country is in progress [169]. Worldwide, there are an estimated 1.1 million specialist surgeons, approximately 550,000 anesthesiologists, and 480,000 obstetricians, with only 20% of this workforce (19% surgeons, 15% anesthesiologists, 29% of obstetricians) working in LMICs [169]. Providers included in this database exclude trained non-physician personnel, which can underestimate the available surgical workforce, as task shifting is more common in LMICs. However, there is no standardized training of non-physician providers and limited data to show safety and effectiveness. Continuous data collection over the time of the surgical specialist workforce will assist in strengthening surgical systems on a local, national, and international scale.
To manage surgical infections adequately, one needs to consider the full spectrum of the healthcare workforce. Multidisciplinary support from physicians in infectious disease and other specialties, if available, can enhance patient care greatly. There needs to be adequate nursing staff, as good nursing care is essential for the care of operative sites. Ancillary support, such as physical therapists, nutritionists, and social workers, also plays invaluable roles in post-operative recovery. Ideally, there should be a laboratory with staff capable of culturing bacterial pathogens and testing them for sensitivity. This allows creation of an evidence-based antibiogram and an understanding of local microbiology susceptibility patterns. The previously cited prospective gastrointestinal surgery study noted that when such services were available to test incision flora, 36% of cultures identified microbes that were resistant to the antibiotic used for pre-operative prophylaxis at that location7 [131].
A growing surgical workforce and appropriate distribution of that workforce are components of increasing surgical capacity. Devries and Rosenberg conceptualize surgery as an ecosystem that involves a network of persons, processes, and materials necessary for rendering surgical services in a local environment (Fig. 2) [170]. Thus, a functional effective surgical ecosystem not only includes the availability of healthcare providers, but integration of related subsystems such as building infrastructure (electricity, waste management), biomedical engineering, supply chains, and pharmacy [170]. The ecosystem model and investment in surgical systems can improve care across all surgical domains and specialties, including surveillance and management of surgical infections globally. This requires continuing surveillance of infections, antibiotic use, laboratory capabilities, and site care materials plus local and national champions to institute educational training modules to improve stewardship.
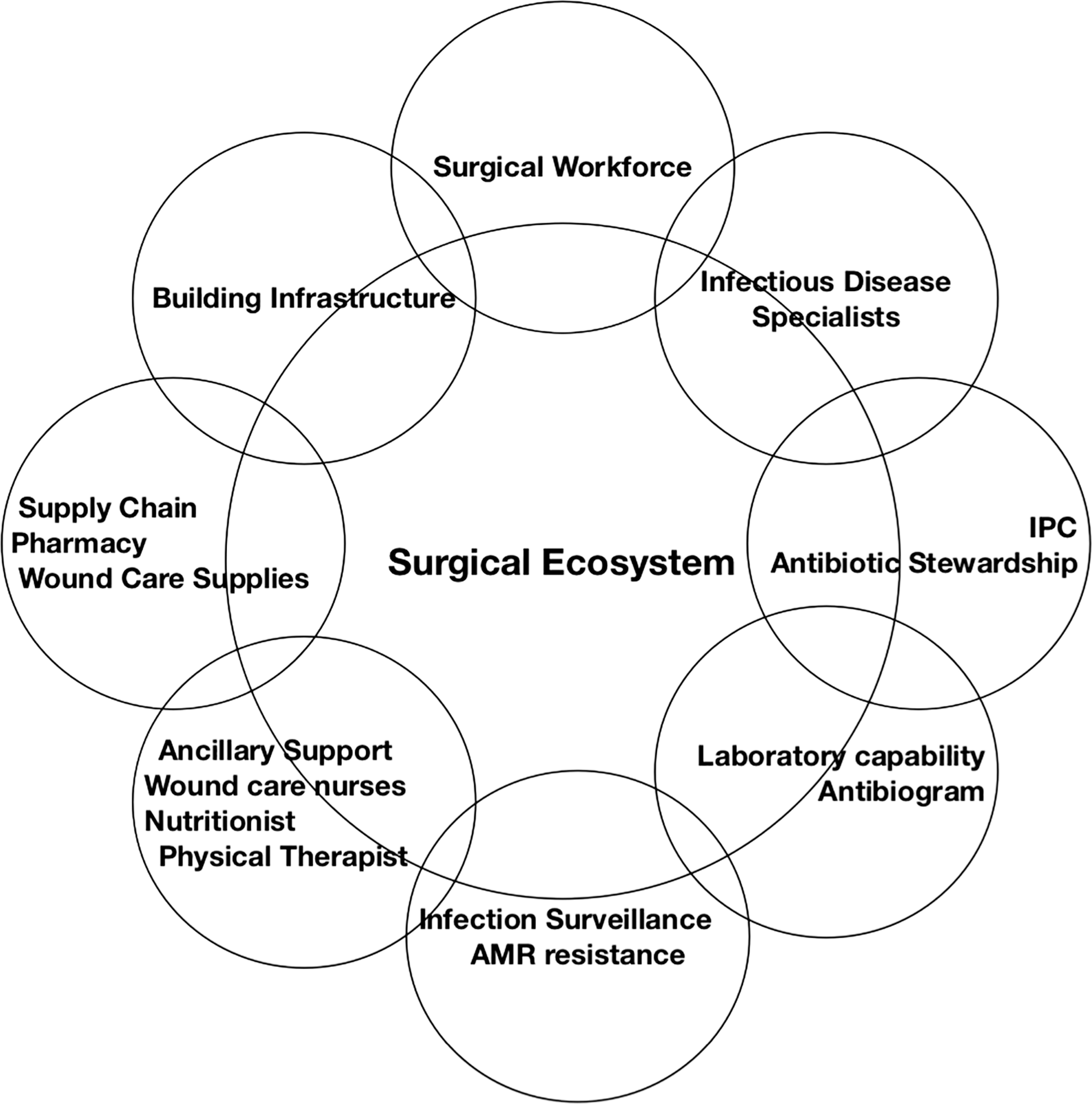
Surgical ecosystem.
One under-recognized aspect of surgical infection management is the availability of materials and local protocols for incision management. Supply chain and resource challenges for gauze, tape, saline, and other dressing supplies can impact incision management. The recent WHO Guidelines on SSI prevention make conditional recommendations on the use of negative- pressure wound therapy (NPWT) and other advanced dressings [171]. Use of NPWT has the potential to improve management of incisions through its wicking of excess fluid, barrier effect on wards with high cross-over infectious risk, and ease of management.
Antibiotic Use, Availability, and Resistance
Surgical infections are treated by a combination of operative intervention and antibiotics, depending on the underlying pathology. The scientific community has fought for focused and logical use of antibiotics for many years [172]. Some 20%–50% of antibiotic usage in acute care models is either unnecessary or inadvertent, which risks longer hospital stays and drug resistance [173]. In the U.S., overuse of antibiotics results in 23,000 deaths and costs $20 billion per year. Increased costs can be secondary to a requirement for more expensive treatment options, delayed hospital discharge, or delayed administration of appropriate antibiotics [174].
Antimicrobial resistance (AMR) in bacteria is driven largely by antibiotic overuse in institutional environments. Antibiotic misuse is rampant throughout the world. This problem is especially problematic in LMICs, as these areas are particularly vulnerable to the economic implications of adverse events related to antibiotics and large-scale AMR and where stewardship might be particularly challenging [175]. In LMICs, only 70% of patients with pneumonia receive appropriate antibiotics, and half of those with viral upper respiratory tract infections receive antibiotics inappropriately [176]. In addition to over-prescribing by healthcare workers, antibiotics may be available over the counter, allowing more prolific community access. There also may be variability in access to antibiotics, forcing providers to change antibiotics continually before treatment is completed, which can lead to resistance. The issue of overuse of antibiotics also has plagued the livestock industry [177]. Animal waste as well as unregulated pharmaceutical waste contribute to resistance; humans are exposed to these antibiotic-resistant bacteria through poor hygiene and contract with contaminated water.
Resistant organisms are classified as multi-drug resistant (MDR), resistant to three or more categories of agents; extensively drug-resistant (XDR), susceptible to only one or two categories of antimicrobial agents; and pan-drug resistant (PDR), susceptible to no category of antimicrobial agents. Patients receiving antibiotics are at a higher risk of becoming colonized with MDR bacteria. Carbapenems and polymyxins are antibiotics of choice for the treatment of MDR gram-negative bacteria [178]. The latest literature shows greater usage of these last-line agents, suggesting a higher incidence of extended spectrum beta-lactamase–producing organisms, XDR, and PDR organisms around the globe [179,180]. Carbapenem- and third-generation cephalosporin-resistant Enterobacteriaceae are an area of critical priority [180].
The growing crisis of AMR is widespread, with much of the data coming from HICs [181]. Drug-resistant infections account for 50,000 deaths yearly in Europe and the United States with an estimated 10 million deaths forecast to occur worldwide by the year 2050, with the majority of deaths predicted to be in LMICs [182]. Despite the dearth of data from LMICs, the existing data demonstrate high rates of AMR. Nosocomial and hospital-associated infections (HAIs) are reported increasingly in LMICs, with studies finding twice the average prevalence compared with Europe and three times the rate in intensive care units compared with the rates in the United States [130]. Emergence of common drug-resistant infections such as methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterobacteriaceae (VRE), and multi-drug–resistant gram-negative bacteria are increasing in LMICs and are most pronounced within LMIC intensive care units [183]. In addition, there is increasing nosocomial transmission of community-acquired multi–drug-resistant organisms such as Streptococcus pneumoniae, M. tuberculosis, Salmonella spp., Shigella spp,, and Vibrio cholerae [184]. The WHO has identified critical resistant bacteria that warrant priority research and new antibiotic development: carbapenem-resistant Acinetobacter baumannii and Pseudomonas aeruginosa, carbapenem-resistant and third-generation cephalosporin-resistant Enterobacteriaceae, vancomycin-resistant Enterococcus faecium, MRSA, clarithromycin-resistant H. pylori, and fluoroquinolone-resistant Campylobacter, Salmonella spp., Neisseria gonorrhoeae, S. pneumoniae, Haemophilus influenzae, and Shigella spp. [185]. The burden of these pathogens in LMICs is particularly worrisome because of the lack of alternative treatment options, limited ability to identify these organisms without adequate laboratory support, and inability to perform antimicrobial susceptibility testing [186]. Surveillance is largely lacking in LMICs, although active measures have been taken to track drug-resistant tuberculosis, malaria, and HIV [187]. Rising AMR transmission in LMICs is compounded by increasing population density, lack of access to clean water, poor sanitation practices, inadequate healthcare infection control, and increased susceptibility to infection because of malnutrition or HIV infection [186]. Despite the bulk of communicable diseases being present in LMICs, those countries typically have the least resources to tackle the problem, with weaker surveillance systems. Therefore, the largest number of lives lost and the enormous economic burden from drug-resistant infections are predicted to be in LMICs [183,188].
The establishment of antimicrobial stewardship programs—coordinated efforts to improve appropriate antimicrobial usage, including prescription of the optimal agent, dose, and duration of therapy—is an important global strategy to decrease antimicrobial use and resistance. In high-income areas, these programs have shown success in reducing resistance, lowering costs, and improving overall care [189]. Individual instances of stewardship in LMICs have been successful. For example, one Doctors Without Borders surgical program for victims of war in Amman, Jordan, Iraq, Yemen, and Syria demonstrated that implementation of a stewardship program in areas with a significant lack of resources resulted in a cost reduction of $160,000 and overall decreased broad-spectrum antibiotic use [190]. The intervention included a team that reviewed hospital prescriptions and made recommendations to optimize the choice of treatment, duration, and route [190].
Challenges to establishment of antimicrobial stewardship programs include variable access to antibiotics, limited data on local resistance patterns, cultural and organizational differences, and cost loaded on top of loco-regional variation in organism representation and resistance patterns. In addition, a majority of antibiotics in LMICs are prescribed in the community [191]. Strategies that need to be employed in the this setting include improving knowledge of the medical staff, pharmacy workers, and public regarding treatment guidelines and appropriate antibiotics and adjusting the inventory of antibiotics. This teaching should start at the medical student or undergraduate level [191].
Future interventions also may display unpredictable geographic variations, such as efforts targeting at restoring a healthy microbiome and host immune defense modulation. Finally, with the increasing frequency of global travel and medical tourism, increasingly robust methods to track the spread of resistant organisms will become ever more necessary.
Measurements and Indicators
Measurement is the cornerstone of improvement; without a contemporaneous understanding of outcomes, improvement becomes impossible. The classic strategy for measurement is described in the Donabedian framework of structure, process, and outcome, where structure relates to the resources available within the system of care, process refers to the practices that contribute to the delivery of care, and outcomes are the results of care [192]. A number of indicators can improve a facility's understanding of its results and direct improvement opportunities (Table 2). These indicators are ideally suited for facility-level collection; however, they also can be used in aggregate nationally to aid with policies that could improve surgical capacity, delivery, and outcomes.
Measurement and Surveillance Recommendations
IPC = Infection Prevention and Control.
Although outcomes are clearly of tremendous value, understanding the system and the processes of care also are useful, particularly when attempting to value and incentivize improvements at the facility level. Some structural measures can be achieved quickly, whereas others will be a greater challenge. One important structural characteristic of a facility is the presence of an Infection Prevention and Control (IPC) committee that takes responsibly and maintains oversight of infections and quality control mechanisms within a hospital, clinic, or health system [193]. Such a committee can audit processes of care, particularly as they pertain to peri-operative antibiotic use and infection control practices (such as sterilization of instruments and surgical equipment, pre-operative bathing, and skin and hand preparation). They also can impact practice, especially when leading surgeons participate in such a group, as the misuse of antibiotics in the peri-operative and post-operative period is a major source of potential harm; these practices, often are engrained during training, founded on misconceptions of how antimicrobial drugs work, and require continuing education and oversight to bring practices into line with accepted standards. The presence of a microbiology unit or a laboratory that can perform cultures and sensitivity testing is an important aspect of IPC. Knowing what organisms are responsible for infection and the local AMR patterns is critical for selection of appropriate antibiotics. By the same token, knowing what antibiotics are available to the surgeons for both prophylaxis and treatment—coupled with an understanding of community and hospital resistance patterns—allows a facility and its IPC team to use antimicrobial resources effectively and efficiently. This usually cam be understood through pharmacy inventories, purchasing history, and supply logs.
The early use of broad-spectrum antibiotics in patients presenting with sepsis is well established [194]. Administering empiric, broad-spectrum antimicrobial therapy within one hour of presentation when there are signs of sepsis or septic shock, coupled with the narrowing of therapy once a pathogen is identified, is best practice. For patients presenting with an intra-abdominal infection, once source control has been established definitively, antibiotics can be discontinued safely after four days [195].
The timing, selection, and duration of antibiotics present a tremendous opportunity for improvement. According to the WHO Guidelines on SSI Prevention, surgical antibiotic prophylaxis should be administered within 120 minutes of skin incision [196]; in fact, many authorities have recommended that antibiotics be delivered within 60 minutes to take advantage of peak tissue concentrations after intravenous administration [197]. For practical purposes, this frequently means antibiotic delivered either in the immediate pre-operative period or once the patient arrives in the operating room. Antibiotic selection should be guided by the type of operation, the likely contaminant (skin, gut flora, etc), and resistance patterns in both the community and the hospital [198,199].
Infection prevention and control efforts frequently are disconnected from the circumstances of surgical care and occur without the input of surgeons. As surgical providers contribute to these committees, understanding whether and how they participate, and promoting their training in surgical infection control principles, can help strengthen local priorities to reduce peri-operative infections and advance surgical outcome surveillance systems. Surgical involvement in IPC activities must be encouraged and IPC expertise leveraged on behalf of surgeons working to improve the quality and safety of surgical care.
There is a wide range of outcomes to monitor at both the patient and the facility level. The peri-operative mortality rate (POMR) has been suggested as a global surgical indicator. Other potential measures are length of hospital stay, SSI rate, and AMR.
The current definition of SSI comes from the Centers for Disease Control (CDC), which defines superficial, deep, and organ space infections [200]. These definitions can be cumbersome, as diagnosis by a physician frequently is the default in the absence of other clinical signs. More objective criteria have been applied in large studies, particularly when trying to compare different settings, such as the GlobalSurg II study assessing SSI rates for gastrointestinal surgery across 343 hospitals in 66 countries [131]. Such criteria include: (1) Purulent drainage from the superficial or deep incision; (2) pain/tenderness, localized swelling, redness, heat, or fever and that the incision is opened deliberately or dehisces spontaneously; or (3) abscess within the incision [201]. This is a practical and practicable definition that relies on purely objective criteria. Such practical definitions capture clinically meaningful morbidity, as drainage, purulent effluent, incisions that have opened, and abscesses all require additional care and add to the length of stay and cost. Organ-space infections, the most challenging to diagnose and treat, still defy easy assessment without the use of imaging, something that can be prohibitively expensive in many settings. Even in HICs, such infections usually require the maturation of an abscess rind in order to distinguish free edematous fluid or old blood from actual infection or clinical deterioration that drives surgical or other invasive intervention regardless of imaging findings.
Solutions and Interventions
Reduce the burden of surgical infections
There many preventive and treatment options to reduce the burden of the wide global range of surgical infections. Clean water and sanitation can prevent typhoid fever transmission, and its early recognition and treatment may prevent intestinal perforation. Vaccination can stop the spread of hepatitis B and C and progression to HCC. Helicobacter pylori and peptic ulcer disease can be treated with triple therapy and managed long term with proton pump inhibitors and histamine blockers. Preventive maintenance of patients with diabetes can prevent or delay the onset of peripheral neuropathy and diabetic foot infections. Early fracture immobilization, fracture reduction, and wound irrigation can reduce disability and infections such as osteomyelitis that can be associated with open fractures [202].
Much literature has been dedicated to the prevention and management of SSIs. Environmental and resource factors include availability of surgical site preparation, hand washing techniques, pre-operative antibiotics, infection surveillance, incision management systems, and peri-operative serum glucose control. Patient and surgical factors include body mass index (BMI), diabetes, cardiopulmonary disease, length of operation, blood loss, degree of contamination, and location of the operation. Reducing the incidence of SSIs leads to significant clinical improvements for patients, cost savings, and reduced hospital lengths of stay. In recent WHO guidelines for SSIs, 29 recommendations are made based on the most recent evidence [196]. Although some of these guidelines are not readily deliverable in LMICs, many others are achievable.
Patient education and participation have been promoted in medication management in recent years. In 2017, a group of infection prevention and infectious disease experts convened to review how current evidence could be conveyed to patients to increase their participation and in turn reduce SSI rates [203]. The experts produced nine recommendations ranging from S. aureus decolonization, to personal hygiene measures pre-operatively and post-operatively, to management of diabetes mellitus. Patient participation can be an especially high-yield concept in LMICs, where patients often live remote from hospitals and health centers. Engaging key stakeholders, such as Ministries of Health, is critical to ensuring program sustainability.
Improve surveillance of surgical infections
Lack of personnel and money is one of the major obstacles to compiling reliable surveillance data when paper forms are used and hospitals do not have electronic health records. Automated data capture and central deposition may be particularly advantageous for review and analysis. Research Electronic Data Capture (REDCap) is one useful application for wide-scale projects [204]. “Store and forward” data collection is especially important when collecting data in areas where internet access is limited [204].
Establishing national databases with hospitals and health centers enrolling in the programs voluntarily may improve surveillance. One such effective and thoughtful approach emerged in Thailand in 2009 where 10 hospitals enrolled [205]. A central headquarters for recording data on one computer was established at each study site, and a form, manual, and website were created to guide each of the sites. Key aspects that led Thai investigators to enroll almost 18,000 patients was their commitment to follow-up and access given to individual hospitals. Quarterly centralized meetings were provided for discussion and instruction, to review definitions, and to analyze data. Researchers visited each site every two to three months and were available continuously via telephone or e-mail throughout the study period. Furthermore, researchers allowed hospitals to compare their SSI data with the pooled dataset from the other nine hospitals. Surveillance tends to improve care and outcomes, so it is not surprising that all hospitals had a decrease in SSI rates during the period.
Further opportunities for improving surveillance will involve education of healthcare providers, patients, and families. Many SSIs appearing after discharge may be missed in existing surveillance programs. Novel studies are examining the role of smartphones and mHealth technology to identify and track outcomes including surgical infections [206].
Improve antibiotic use and stewardship
The first goal to improve use of antibiotics should be to track how often they are used. Antibiotic surveillance should occur in parallel with surveillance of surgical infections, and information should be recorded through establishment of a centralized registry or use of advanced database tools. The following information should be recorded: Antimicrobial agents used, dose, route of administration, duration of use, and organisms treated (whether cultured or presumptively diagnosed). When it is available in LMIC locations, thoroughly recording microbiologic culture data is important to assess the appropriateness of antibiotic use. A team should be created to evaluate antibiotic use. In conjunction with available data on bacteriology and AMR patterns, the team should help develop a tool to optimize antibiotic selection.
The next goal should be to establish country or regionally based antibiotic stewardship programs (ASPs). Such programs are still fairly new even to HICs, with most started in the last decade. Much of the early progress in establishing ASPs will be recording data on antibiotic use and duration as it relates to the microbiology or diagnosed SSIs (Table 3). The concepts of a dedicated team to start an ASP, record data, and manage improvement projects have been described in the literature for environments with better resources [207].
Key Questions for Establishing Antibiotic Stewardship Programs
Although an ASP program may not be feasible in all settings, concepts of antibiotic stewardship should be stressed in LMICs. Education should be the cornerstone to improving antibiotic stewardship and to achieving optimal effects, should not be purely passive; e.g., using just written materials and lectures [208]. The highest yield in making gains in antibiotic stewardship may necessitate earlier education programs, starting in medical, pharmacy, and nursing schools. Little curriculum has been devoted to antibiotic stewardship in more resourced areas of the world yet 90% of medical students suggest a need for more education on the topic [209]. Recruiting well-regarded surgeons to lead this work helps reassure other clinicians that best practices involve more judicious and selective use of antibiotics.
Improve management of surgical infections
Improvements in the management of surgical infection can be achieved through early recognition. Once infections are recognized, management often requires simple straightforward surgical principles including source control, dressing care, thoughtful antibiotic courses, and diligent followup. Improving early recognition involves concepts similar to those described above regarding surveillance. Surgeons in LMICs often have significantly greater workloads because of shortages of trained colleagues and provide care for a larger number of patients over wider geographic regions. An outreach program allows specialists, such as orthopedists, who often are more centrally located in the major cities, to come to the primary-level hospitals on a weekly or monthly basis to perform cases while educating general practitioners on open fracture management. Increasing the training of surgeons is a valuable step to increase the number of specialists within a country, although this is costly and takes time. An alternative is to train general practitioners, nurses, and health center workers on the signs and symptoms of surgical infections. Technology to improve communication between outpatient providers and surgeons also may help improve early recognition of surgical infections.
Increasing health center workers' capacity in LMICs through education programs establishing them as a local experts improves management of a number of disease processes including HIV, hypertension, adolescent care, and chronic kidney disease [210–212]. By engaging in serial, frequent training sessions of health center workers, marked improvements can be made in earlier recognition and treatment of surgical infections [206]. The goals for health center workers are to establish skill sets to recognize superficial SSIs and appropriate site care. Additionally, health center workers should be trained to recognize signs and symptoms of common surgical conditions including peritonitis, obstruction, and soft tissue infections. Education on common post-operative complications requiring operation, such as deep incisional and organ space infections, will identify patients needing prompt referral to a facility with surgical capabilities. Lastly, training should include appropriate indications for and usage of antibiotics. Training and education principles can be applied to general practitioners, healthcare workers, nurses, and pharmacists in both inpatient and outpatient settings so that surgical infections are embraced as a multidisciplinary problem that all providers are stakeholders in. Ideally, training will be conducted in local environments, ensuring that providers are able to apply the principles using local resources. Training and education programs also should include methods to monitor retention of knowledge and skills.
Large gains can be achieved by mobilization and education of personnel, including surgeons, nurses, operating room technicians, hospital staff, and patients. Regardless of which guidelines are chosen on the basis of available local resources, we suggest a bi-annual educational program of institutional guidelines, with the program materials delivered to all providers involved in the care of surgical patients. A bi-annual schedule would allow updates in evidence to be discussed. Adherence to institutional guidelines should be monitored over intervals and compared with surveillance data on the rates of surgical infections during the same intervals. Future directions can involve technology to allow collaborative education programs between institutions in LMICs. This could improve efficiency of content delivery, as programs could be conducted in regions that have similar resources and surgical diseases. There also is an opportunity for HICs to engage with LMICs in this fashion.
Conclusion
Surgical infections constitute a large burden of disease globally, with a significant burden carried by LMICs. Challenges to management in LMICs include a shortage of trained personnel and material resources. The increasing rate of AMR, likely related to antibiotic misuse, adds additional challenges. Development of surveillance, infection prevention, and antimicrobial stewardship programs are initial steps forward. Education is critical and should begin early in training, be an active process, and be sustained through bi-annual educational programs.
Footnotes
Author Disclosure Statement
The authors have no disclosures or conflicts of interest to report.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.