
Abstract
Abstract
Background:
There has been tremendous growth in the amount of new surgical site infection (SSI) data generated. Key challenges exist in understanding the data for robust clinical decision-support. Limitations of traditional methodologies to handle these data led to the emergence of artificial intelligence (AI). This article emphasizes the capabilities of AI to identify patterns of SSI data.
Method:
Artificial intelligence comprises various subfields that present potential solutions to identify patterns of SSI data. Discussions on opportunities, challenges, and limitations of applying these methods to derive accurate SSI prediction are provided.
Results:
Four main challenges in dealing with SSI data were defined: (1) complexities in using SSI data, (2) disease knowledge, (3) decision support, and (4) heterogeneity. The implications of some of the recent advances in AI methods to optimize clinical effectiveness were discussed.
Conclusions:
Artificial intelligence has the potential to provide insight in detecting and decision-support of SSI. As we turn SSI data into intelligence about the disease, we increase the possibility of improving surgical practice with the promise of a future optimized for the highest quality patient care.
It is projected that the big data revolution will yield annual healthcare savings between $300 and $450 billion in the United States alone [1]. A part of these savings might come from reducing the occurrence of costs associated with surgical site infections (SSIs). Rapid advances in sensor and information technologies have resulted in a data-rich environment, including both subjective and objective observations pertaining to SSI. Current knowledge of SSI comes from clinical experience and laboratory experimentation, but there has been a lack of systematically collected observations from post-operative patients, and hence a limited understanding both of how SSI evolves in real clinical settings, and of the insights that big data analytic might provide. Healthcare system characteristics present challenges that call for specialized techniques capable of integrating data, extracting intelligent knowledge and monitoring data from multiple sensors. The challenges in using these methods to address data relevant to SSI lie in complex new types of data (e.g., text, image), in a lack of deep understanding of the disease that could contribute to a model (e.g., monotonic progression), and in the complexity in clinical decision-support (e.g., risk predictions). As pointed out in a recent review article [2], surgeons are uniquely positioned to help drive innovative uses of AI to address SSI, in order to realize economic incentives, and improve safety and efficiency.
The emergence of new types of SSI data such as spatial-temporal data, free-text narrative data, and surgical site images allows researchers to explore the underlying opportunities of them with the field of artificial intelligence (AI). Many AI tools, such as natural language processing (NLP) for text analysis, deep learning (DL) for unstructured data such as images, temporal data, etc., and machine learning (ML) algorithms for data pre-processing, computing, and modeling, help in identifying patterns of SSI data. However, key challenges exist in applying these methods in the use of SSI data, where we need a holistic approach to move our understanding from data to information to knowledge and wisdom for sustainable and real impact.
In this article we provide some specific examples from recent studies and identify emerging opportunities to improve the detection, monitoring, and decision-support of SSI given these challenges. We also examine the limitations of using AI, including integration and adoption in clinical settings, interpretability, and the requirement for high-quality data needed to train models. The overview of an AI pipeline to address SSI is shown in Figure 1. We present several challenges in detection, monitoring, and decision-support and we discuss examples of AI methods applied to SSI detection and monitoring decisions, respectively. Finally, we conclude with the current limitations of AI methods.
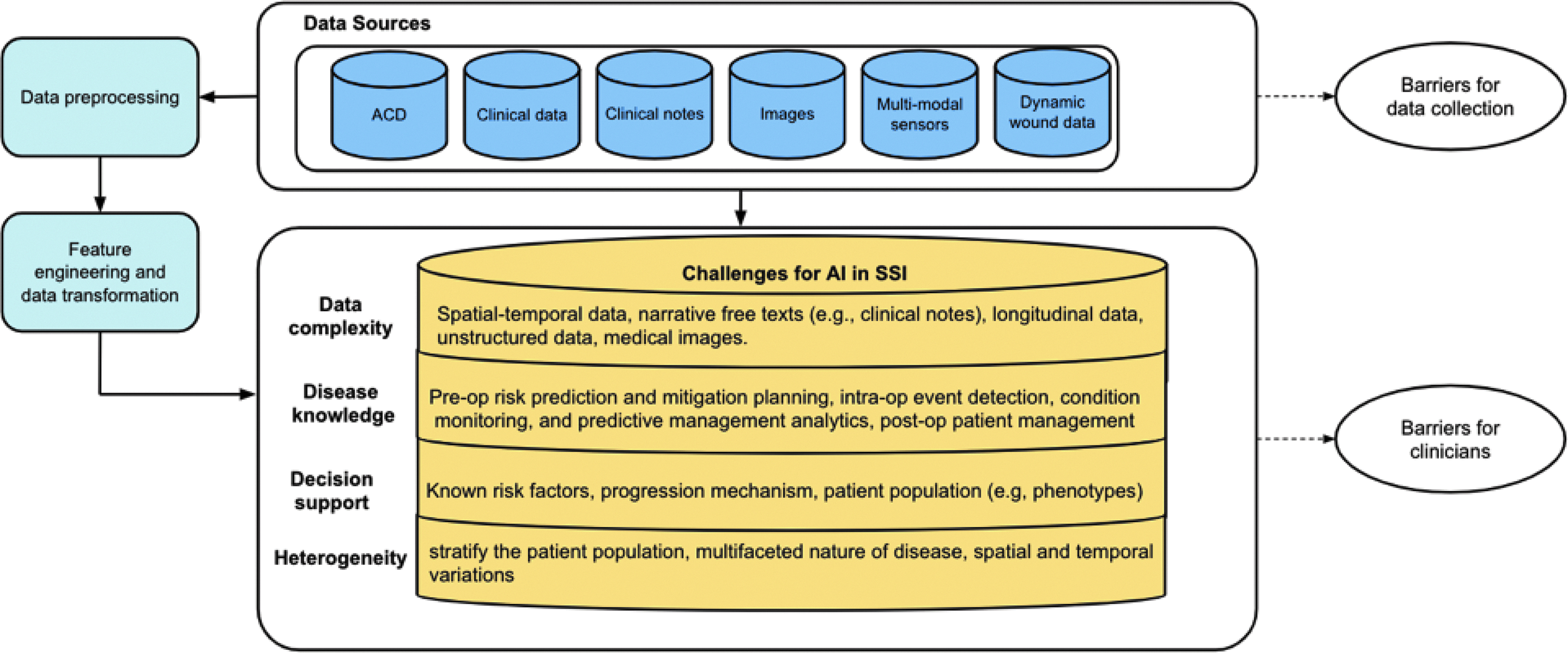
Overview of the artificial intelligence (AI) pipeline. Color image is available online.
Detection, Monitoring, and Clinical Decision-Support Challenges
Complexities in using SSI data
Available data related to SSI have been largely limited to administrative coding data (ACD; e.g., diagnosis or procedure codes) and clinical data (e.g., vital signs, symptoms, laboratory, and radiology results).
Administrative coding data lack clinical content
Several traditional surveillance methods rely on ACD data. Some of these works focused mainly on using antibiotic choice and timing [2,3], using traditional statistical methods such as statistical process control charts (SPC) [4,5] or developing standardized infection ratio (SIR) [6,7]. However, several challenges are apparent in using such traditional methods. For example, Baker et al. [4] applied conventional Shewhart and the exponentially weighted moving average (EWMA) SPC charts to 10 previously investigated SSI outbreaks that occurred from 2003 to 2013. Their studies were limited to an evaluation of the specificity of out-of-control signals at study hospitals, hence, there were chances that false alarms may have coincidentally preceded an actual outbreak in their study. Another traditional method is SIR. It has been considered as a statistic available for most risk-adjustment analysis by infection control practitioners. However, Delgado-Rodriguez and Llorca il [8] discussed how SIR could be a misleading procedure for controlling differences in patients' intrinsic risk of infection by illustrating multiple cases.
Clinical data lack structure
Despite evidence supporting traditional measures, they have not been widely adopted in clinical practice, and they do not incorporate some of the clinical elements of interest (e.g., clinical signs, symptoms, patient demographics, medical history, and surgical information). An approach to overcome these problems is the use of clinical datasets gathered from various sources (e.g., pharmacy, laboratory, and electronic health records (EHRs) [9–12]). However, often these data are unstructured, requiring additional data preprocessing, cleaning, and advanced data-driven approaches to integrate multiple sources and draw meaningful conclusions that support decision-making and SSI prediction. Conventional methodologies have limited ability to analyze large amounts of complex, unstructured data [13]. Recent applications of AI methods in SSI detection and surveillance have been largely motivated by the emerging new types of data, such as longitudinal structured observations, automated processing of free-text narrative data, provider-acquired wound images, and patient-generated health data (PGHD), including patient-acquired images. Next, we discuss challenges that exist in the use of new types of SSI data, and provide examples of how AI-driven opportunities can tackle these challenges.
Dynamic wound data lack all available sources required in utilizing continuous measurements
Capturing temporal patterns is essential to develop robust algorithms for prediction of SSIs. Clinical registries record temporal data, and the patterns in those data have been explored to predict the risk of complications and re-admissions after surgery [14–16], and to guide quality improvement in surgery [17,18]. Existing prediction models of SSI have incorporated static parameters, e.g., demographics, pre-operative laboratory results, etc. [9], and they are limited on specific time windows of the SSI progression process [19]. Unlike existing prediction models that have limited capacity to utilize temporal clinical data, Ke et al. [20] developed a decision-support system that is capable of SSI predictions with the help of several ML models. Ke et al. [20] developed an efficient optimization algorithm via a bilinear formulation to predict time to SSI onset with spatial-temporal data. Utilizing continuous measurements of surgical site-related parameters generated by mobile health (mHealth) tools, their proposed framework outperformed some of traditional AI methodologies such as linear regression. This is because with real-world applications, one common data challenge is that many patients do not develop SSI during the observation period. Thus, an advanced learning formulation that can use continuous measurements is needed. However, many of these advanced learning formulations rely solely on limited dynamic measures such as pre-operative patient descriptors while excluding post-operative parameters and image-based incision parameters [21,22].
It has been found that many post-operative and image parameters are important in predicting the SSI risk and may help guide physicians with decision supports [22,23]. Thus, investigating how surgical site image data and static risk factors combined with the dynamic surgical site data may increase the capability to predict SSI risks are some of the future research direction in utilizing evolving clinical data.
Free-text narrative lack data structure
With the increased availability of free-text narrative data, text mining has become increasingly important. Text mining is the process of structuring the input text and turning the text into data for analysis via the application of NLP, ML, and DL. The following is a list of some of the advances in extracting information from the text to improve SSI detection. Natural language processing refers to automated methods for converting narrative free text into computer-understandable format [24]. Advances in NLP have been used to identify SSIs [25,26]. For example, Bouzbid et al. [27] evaluated seven different strategies for the automated detection of nosocomial infections (NIs) in an intensive care unit (ICU) by using interconnected hospital information systems. This work showed that the automated detection of SSI represents an alternative to traditional monitoring methods.
Shen et al. [28] developed a lexicon of keyword features from clinical narratives using sublanguage analysis with heuristics to detect SSI and evaluated these keywords with medical experts with a precision of 90%. Their approach was able to identify SSI keywords from clinical narratives and could be used as a foundation to develop an information extraction system by augmenting search queries. An NLP-based approach offers several potential advantages over administrative-code based strategies to identify healthcare quality concerns. As opposed to administrative codes, search strategies using daily progress notes, laboratory reports, or imaging reports could be monitored on a prospective basis. Thus, this approach potentially identifies SSI while a patient is still in the hospital, which could greatly facilitate real-time quality assurance processes.
On the other hand, NLP-based algorithms are limited by lack of data sharing between healthcare organizations, and limited documentation of information and available data sources. Machine learning methods instead can be used for note classification that may require less expertise in the linguistic analysis [26,29]. For example, Sohn et al. [26] used an automated detection system via the Bayesian network to detect clinically important colorectal SSIs using risk factors from American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) data. Another example from Ehrentraut et al. [29] used support vector machine (SVM), a discriminative classifier defined by a separating hyperplane, and gradient tree boosting, a decision-support tool that uses a tree-like model for the application of text classification to detect hospital-acquired infections from patient records from a large Swedish hospital. They built an automatic surveillance system to reduce the burden of manual expertise for SSI detection.
Natural language processing has a strong linguistics component that requires an understanding of how we use a language (e.g., the subconscious bias in the text, etc.) to encode it into a ML algorithm to discover similar patterns automatically. To tackle this challenge, the class of DL algorithms can be used to extract high-quality information from unstructured and structured text. With the help of DL, the information in a text could be patterned without considering the semantics in the text. Deep learning has shown widespread advances in capturing the latent predictive features from clinical notes [30,31]. For example, Miotto et al. [31] developed the DeepPatient model that presents a novel DL method to derive a general-purpose patient representation from EHR data to facilitate clinical predictive modeling. Their findings indicate that DL applied to EHRs can derive patient representations that offer improved clinical predictions and could provide a ML framework for augmenting clinical decision-support systems by assessing the probability of patients to develop SSI. Overall, the performance of DL measures is direct and relatively simple; it has measurable mathematical concepts that can also be automated.
Wound images are challenging in processing techniques
Among novel data sources for SSI detection, incision images have garnered interest [32,33]. Sanger et al. [32] assessed how adding incision photographs to existing data sources modifies provider decision-support. They presented a Web-based simulation survey to a convenience sample of providers with expertise in surgical infections and demonstrated that adding incision photographs improved overall diagnostic accuracy from 67% to 76% (p < 0.001).
Broman et al. [34] examined how patient-generated incision photography affects SSI diagnosis in a realistic setting. In their study, they compared the surgeon's assessment of post-operative wounds with and without photography for detection of SSI. They found that photography increased specificity (from 56% to 63%) and improved surgeon confidence in making a diagnosis, but worsened sensitivity (from 58% to 50%) for the detection of SSI. As these two examples suggest, additional development of tools may be required to support improvements in prediction. Incision images are a challenging type of data because of the variability of subject and quality, particularly when generated by mobile devices in varying lighting conditions, and by non-professionals under uncontrolled conditions. These factors challenge computer vision and medical image processing methods, demanding novel ML efforts to make the most of processed image data.
Disease knowledge
The increased availability of various types of SSI data has also resulted in the growth of disease knowledge, deepening our understanding of SSI in terms of disease progression and key measures of risk factors. Many data collection methods have been developed to monitor patients who are subject to develop SSI. For example, to assess the condition of incisions, daily incision measurements such as temperature, granularity, a distance of the wound, etc. along with clinical signals such as body temperature and heart rate could be used. Figure 2 shows real-world longitudinal data of a incision-related parameter (type of exudate present) that indicates the monotonic degradation process of the SSI group. Combining these SSI data to capture the underlying SSI process to predict a patient's risk predictors may facilitate effective preventive care in SSI, however, conventional methodologies usually yield low accuracy [14,35].
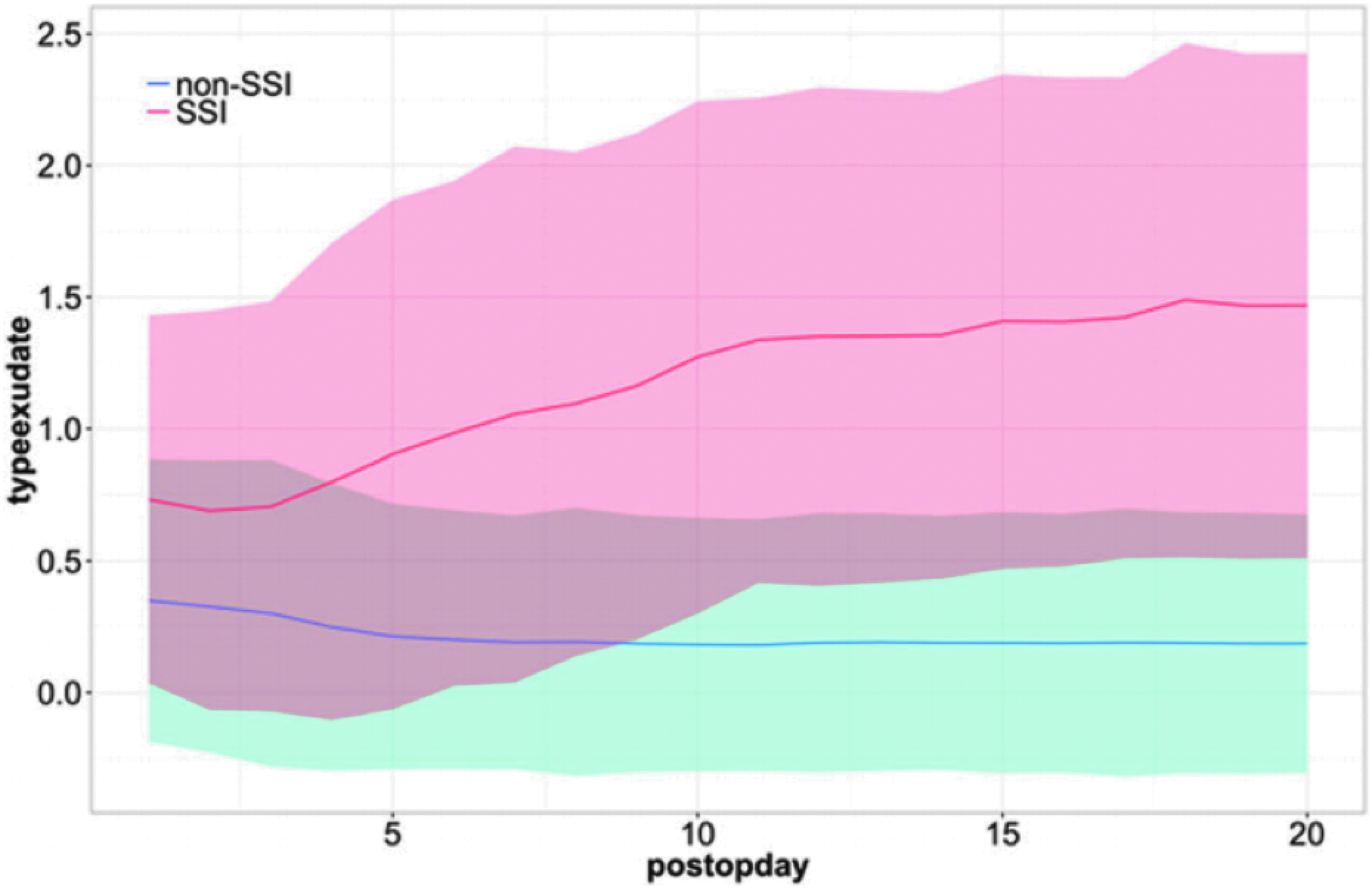
Example of the longitudinal data of incision assessment that could gradually separate the surgical site infection (SSI) group from the non-SSI group as the condition progresses over time [39]. Color image is available online.
An AI-driven approach for patient risk predictors can equip surgeons with automated assessment and feedback by bringing efficient tools to maximize the quality of care [36]. For example, to assess analytics, complex data should be transformed and modeled using appropriate AI techniques to derive objective measures that can inform various aspects of care, including prevention, diagnosis, or intervention [13]. In SSI analytics, these complexities can arise when we deal with irregular time series data, collected from different individuals at different time points within a different time duration. This characteristic violates the underlying assumptions of many statistical models for time series data analysis. Also, many clinical parameters can be measured longitudinally, and there might be many parameters that are not useful or redundant with others. That said, for robust clinical decision-support systems, AI methods aspire to solve these problems. For example, Lawson et al. [37] identified risk factors that were uniquely predictive of superficial versus deep organ/space SSIs through hierarchical multivariable logistic regression models. Their approach accounted for clustering of patients within hospitals by allowing each hospital to have a different random intercept and incorporates the empirical Bayes method.
Another example is the study conducted by Gervaz et al. [38], in which they used a multivariable logistic regression model for prediction of SSI after colorectal resection. They showed that a simple clinical score based on four pre-operative parameters was clinically useful in predicting the risk of SSI. Although these advanced techniques can be used to represent the progression of SSI, they usually ignore the multifactorial aspects of the disease. For example, building trajectory models solely based on measures from clinical data can only capture one part of SSI progression, whereas there are many other measures (text, images, etc.) that can be used. Therefore, future studies must accommodate the need for multi-modality prediction models to combine different sources of data using domain knowledge of the disease.
Decision-support
Artificial intelligence methods could be useful in addressing clinical decision-support systems, from pre-operative risk prediction and mitigation planning to intra-operative event detection and condition monitoring/predictive management analytics, to post-operative patient monitoring. This can be achieved by making sense out of data and understanding how to make the best use of SSI data to obtain valuable information for decision-support. For example, pre-operative baseline data for a patient undergoing bariatric surgery may include glucose levels, meal calories, and fitness tracker actigraphy. Data-driven methodologies for pre-operative baseline data can yield valuable predictors for post-operative care [40]. Mujagic et al. [41] examined the association between commonly obtained pre-operative biochemical markers and the risk of SSI via a multiple logistic regression model. Their approach potentially could be used for modifying pre-operative and intra-operative strategies when the consequences of developing SSI would be dire.
Another possibility to support decision making is by utilizing continuous data streams throughout the surgical care pathway. This requires continuous intra-operative monitoring, which integrates EHRs and clinical parameters to optimize care, and provides intelligent assistance to decision makers [42,43]. In this context, computer vision can utilize mathematical techniques to analyze images and video streams, and transform them as quantifiable features such as color, text, and position, which can further be used to identify bleeding or other significant intraoperative events. For example, the successful utilization of DL could be beneficial in creating such computer vision algorithms for classifying SSI tissue types with high accuracy [44]. Nejati et al. [44] suggested an automatic long-termc SSI tissue classification system that correlates to actual clinical assessment and supports clinical decision-making. They proposed the use of layers of a pre-trained neural network as high-level image representations, subjecting them to dimensionality reduction. The smaller set of features was then used to train a discriminative classifier using the SVM algorithm to label the incision image into seven tissue types.
Extensive literature exists in predicting SSI in post-operative patients. For example, Shapiro et al. [45] undertook one of the earliest studies to determine risk factors for SSI. Using logistic regression, they found seven significant predictors of post-operative SSI including duration of surgery, antibiotic prophylaxis, age, surgical procedure, obesity, blood loss, and surgeon [45]. Another example is a recent user-friendly post-operative mortality risk calculator called emergency surgery score (ESS) developed by Han et al. [46]. This algorithm used multiple univariable and multivariable models to predict the risk of SSI by measuring the correlation between ESS and the probability of occurrence of 30-day post-operative complications via calculating the c-statistic. The ESS predicts accurately the occurrence of post-operative infections and could be used for pre-operative clinical decision-support, as well as quality benchmarking of infection rates.
Heterogeneity
It is known that the heterogeneity of the patient population (even of the same diagnostic group) plays a substantial role in the clinical outcomes [13], for reasons such as severity of disease, responsiveness to the care, or the presence of multiple comorbid conditions. The existence of patient heterogeneity multiplies the complexity of developing AI models. For one thing, clinical data management systems usually are derived from large collections of data, but there is still a relatively small amount of data for each patient. One way to personalize predictions for each patient is to build a patient-specific predictive model to identify more relevant and informative patient-specific risk factors for each patient. Because of the costly computations of building individual models, most existing statistical models are designed for an average user and ignore patient heterogeneity, therefore limiting their applicability in real-world settings.
From the perspective of personalized medicine, a “one size fits all” predictive model may not be the best approach for individual patients. Such a static global model captures information that is important for the entire training patient population but may miss less information that is important for each patient. For these reasons, personalized models in the context of healthcare have been investigated. Recent work in the area of personalized medicine in SSI show that each patient has unique characteristics and that the patient population is heterogeneous [47,48]. For example, early use of ML models in analyzing the SSI re-admission data has revealed interesting patient subgroups, in which a subset is defined by a distinct clinical characteristic that leads to statistically different risk levels for re-admission. For example, Hartney et al. [47] studied the link between SSI complications and re-admission using a conditional inference tree (also referred to as recursive partitioning) that uses statistical theory to select parameters for estimating interpretable personalized re-admission rules. Given the re-admission rules created by their model, they could identify subgroups of patients having different risks such as those who have an organ/space infection or who are likely to return to the operating room or are candidates for early discharge.
Whereas addressing the heterogeneity of patients may call for personalized models or uncertainty quantification to augment AI techniques, this may also motivate clinicians to develop new approaches to subgroup detection and analysis. This may be an effective strategy to personalize treatment by using techniques such as using clustering or deep learning. For example, in the research by Nezhad et al. [48], a bi-clustering algorithm using convex optimization was developed to detect patient subgroups and prioritize risk factors for hypertension (HTN). Unlike traditional integrative clustering methods, DL can better exploit the deep intrinsic statistical properties of each input modality and complex cross-modality correlations among multi-platform input data [49].
Relevant AI Methods for Detecting SSI
The range of new types of SSI data make almost every branch of AI and ML potentially useful [2,16,50–55]. Given this promising prospect, however, we realize that it is also a possibility that the true promise of AI could be lost in its hype similar to many other emerging technologies if AI could not be fully integrated into clinical practices or well understood by both surgeons and data scientists [2,56]. Thus, we recognize that the data to information to knowledge to encoded wisdom (DIKW) pyramid (Fig. 3), holds great relevance in the era of big data. In this section, we apply our recently developed contemporaneous health index (CHI) framework to illustrate how this paradigm could be useful to guide AI development tailored for the application context and data characteristics specific to SSI.

The artificial intelligence AI data to information to knowledge to encoded wisdom (DIKW) pyramid for surgical site infection (SSI). Color image is available online.
Contemporaneous health index
The CHI aims to fuse irregular multivariable longitudinal time series data to quantify the severity of degenerative disease conditions over time [39]. It was motivated by the observation, as shown in Figure 2, that incision assessment data would gradually separate the SSI group with the non-SSI group as the condition progresses over time. This gradual separation could be observed when longitudinal data from a group of patients is aggregated, exhibiting a systematic trend that we may term a monotonic degradation process. The CHI method sets a prior modeling form to make sense of the data, in other words, this patient condition progression model is a monotonic model disrupted by random noise. This monotonicity, as revealed in methodological studies of the CHI model in the study by Huang et al. [39], could help build an accurate patient condition monitoring model with substantially shorter observational duration from fewer patients. They demonstrated that in simulation studies and the application on a real-world dataset of SSI, even without training data labeled by infection preventionists, the CHI could be trained using irregular time series data that showed comparable performances with methods that use the label information. Manually labelled training data is a costly barrier to many clinical applications of ML models.
Deep learning-CHI: a dictionary learning-based CHI model to address heterogeneity
Although it is natural to think that we could build a personalized model for each patient using their own data, such models require a substantial amount of labeled training samples, which is generally not feasible in clinical settings. Additionally, this separate learning is not efficient in exploiting the similarity of the patients because we could not share training data. Toward this goal, the DL-CHI framework was built on the strength of dictionary learning. The basic idea of dictionary learning is that data generated in nature (text, images, etc.) have common statistical structures and can therefore be represented as a combination of a set of simpler structures (dictionary elements). Numerous experiments in both simulated and real-world data have shown the effectiveness of DL-CHI in creating personalized CHI models [57].
Uncertainty quantification-based model of CHI to quantify imperfect and continuous delivery of knowledge
A degree of uncertainty is always involved in decision-support systems. This uncertainty can be traced back to sample errors, system noise, or insufficient sample size when the model parameters would be determined unambiguously for complex mathematical models. In clinical predictions, it is necessary to deal with such uncertainty in an effective manner. If the model parameters are not well constrained, the resulting predictions may represent an unacceptable degree of uncertainty that would lead healthcare professionals and caregivers to make uninformed decisions potentially leading to medical errors. Toward this goal, Samareh et al. [58], described the development of uncertainty quantification-based (UQ)-CHI, by combining Bayesian learning and convex optimization using the maximum entropy learning (MEL) framework. Using numerical studies, they demonstrated the effectiveness of the proposed UQ-CHI method in prediction accuracy and monitoring efficacy.
It is worth mentioning that the CHI framework together with its various methods is just one representative AI method among several alternatives. Compared with alternative methods, a unique principle of the CHI method is its level of integration of data and disease knowledge, tailoring its method development for the specific disease context. The monotonic degradation process of the disease condition has been encoded fully into the mathematical formulation of CHI to fuse the multivariable longitudinal data.
Discussion
Application of AI to surgical data
Data-driven methods require transparent, trustable, and systematic cross-validation. Although research on advanced AI methods to detect SSI is at a relatively early stage, often the translation of these methods to practice is through the development of a software-based decision-support system to aid patients or physicians in making decisions. For example, Shenoy et al. [59], proposed a convolutional neural networks (CNNs) ensemble (a subgroup of artificial neural networks that have shown great promise in analyzing visual imagery) called Deepwound to categorize surgical incision images. Further, they developed a mobile application, Theia, that enables patients to generate incision analysis reports and sends them to the surgeon regularly from a remote location, such as their home. With permission from the patient, this app can also be used to collect incision images to add to their dataset. The enlarged dataset can be used to improve their proposed DL algorithms further.
Emerging mHealth tools enable continuous measurements of many incision-related parameters and other evolving clinical symptoms. Using the patient's mobile device provides access to post-operative evaluation and care in an efficient and patient-centered manner. However, most recent research endeavors in the patient's mobile devices in SSI have not yet been used in practice. Mobile apps such as Theia are proof-of-concept of how algorithms developed in research settings can assist physicians and patients in postoperative wound surveillance but have not been commercially used.
Limitations
Barriers for clinicians
An AI-driven method consists of complex algorithms that try to learn latent patterns and relations from data, therefore, explaining how the model works is a challenge. For example, many of these complex algorithms such as ensembles and neural networks typically give more accurate performance compared with traditional ML models such as linear regression. However, clinicians without data science training may have difficulty interpreting the model [60], especially for techniques that are based on black box designs such as neural networks [61]. The benefits of AI models may not be realized if physicians are not comfortable relying on AI-derived results. Therefore, the outcomes of such tools should be built with interpretation by clinical users in mind. Another limitation that has impacted the utility of AI-driven methodologies in medicine is the verifiability and safety of automated analysis. These limitations have pushed the data science community to improve the interpretability of AI analyses [62,63]. Irrespective of the advances in developing the verification of such algorithms, it is critical to address the accountability of these methodologies through collaboration with the clinicians who deliver care, and potentially even the patients to whom the algorithms are intended to benefit.
Barriers for data collection
Greater varieties of data are enabling capabilities in AI and ML in SSI, but information is not always completely available. Earlier, we discussed missing data but other biases in clinical data can affect the prediction capabilities of AI [64]. Within the field of ML, there are two main types of tasks: supervised and unsupervised. The main difference is that in supervised learning we have prior knowledge of what the output values for our samples should be. For instance, input would include a training set of surgical cases would be manually classified as either “SSI” or “not SSI.” Unsupervised learning, on the other hand, does not have labeled outputs, so its goal is to infer the natural structure present within a set of data points. For example, in the context of supervised learning, identification of manually classified training data should be provided. However, the full knowledge of the labels might be not possible because of unavoidable costs associated with data collection.
For example, Karl et al. [65], proposed a framework for SSI identification based only on blood tests. Their objective was to alleviate the problem of getting access to manually classified training data for patients undergoing colorectal cancer surgery. Their framework was based on powerful kernels for multivariable time series that accounted for missing data when computing similarities based on post-operative data. Although the results obtained in their work were promising in the context of unsupervised learning, previous studies [66] show that the combination of heterogeneous data sources such as drugs, texts, or vital signs from EHR might provide better performance. Including more data into the modeling, however, comes at the cost of an increase in the computation cost and a demand for a more complex algorithm.
Conclusion
Artificial intelligence is bringing a paradigm shift to clinical systems, powered by increasing rapid progress of analytics techniques and availability of healthcare data. Surgeons are well-positioned to help drive innovative uses of AI to address SSI to generate real-time clinical decision-support, optimize patient care, and improve safety and efficiency. As the potential to provide decision-support to providers is realized, it may eventually be possible to extend this decision-support directly to patients, although the same limitations, particularly around trust and interpretability, will become even more important.
Footnotes
Acknowledgments
This work was supported by U.S. Centers for Disease Control and Prevention (CDC) award #200-2016-91803 through the Safety and Healthcare Epidemiology Prevention Research Development (SHEPheRD) Program, which is managed by the Division of Healthcare Quality Promotion. The content is solely the responsibility of the authors and does not represent the official views of the CDC.
Author Disclosure Statement
All authors report no competing financial interests exist.