
Abstract
Abstract
Background:
The implementation of health information technology interventions is at the forefront of most hospital institutional policy agendas. Despite the availability of numerous apps and mobile platforms focusing on specific areas in healthcare the widespread integration into clinical practice can be a complex process. Here we present guidelines and methodology that we have learned in the implementation process of new technology and an overview of some of the current barriers and enablers specific to implementation of post-surgical site surveillance technology.
Methods:
Analysis of the experience of successful information technology (IT) implementation in different healthcare systems reveals that, despite differences among patient groups, care providers, and hospitals, there are common barriers and enablers to implementation of health IT.
Results:
The process of implementation in organizations and among individuals can be most successful by identifying barriers and enablers within three key stakeholder groups: (1) patients; (2) care providers/clinicians; and (3) manager/administration within healthcare systems. This can be achieved by specific engagement and co-design processes establishing clear benefits, sufficient incentives, and adequate support for clinicians as well as payer–provider relationships, marketplace competition and privacy legislation.
Conclusions:
The successful implementation of such programs requires appropriate strategic planning to address the needs of three specific components: patients, care provider, and policymakers/healthcare management understanding and acceptance.
Innovative healthcare technology is a key factor in improving quality and reducing cost in healthcare, and yet, the successful adoption of new health information technology (IT) varies greatly among healthcare systems. Proven clinical effectiveness, cost savings, and patient satisfaction are insufficient to ensure adoption and implementation of new clinical technologies. Despite the availability of numerous apps and mobile platforms addressing specific gaps in healthcare the widespread integration into clinical practice can be a complex process.
Analysis of the experience of successful IT implementation in different healthcare systems, reveals that despite differences among patient groups, care providers and hospitals, there are common barriers and enablers to implementation of health IT [1]. Creating commitment to the process of implementation in organizations and among individuals can be enabled by establishing clear benefits, sufficient incentives, and adequate support for clinicians as well as payer–provider relationships, marketplace competition, and privacy legislation. Critical success factors are multiple and require innovative leadership, integrated management, and collaboration with the doctors based on concrete needs, benefits, incentives, and support [3,4]. Initial dilemmas for managers include proof of return on investment for health IT versus leadership and tough management decisions; the optimal balance in the tradeoff between market dynamics, competition, and choice, and the value of an integrated system that can generate substantial benefit to clinicians, patients, and payers [1,2]. The successful implementation of such programs requires appropriate strategic planning to address the needs of three specific components: patient engagement, care provider engagement, and policymakers/healthcare management understanding and acceptance.
Building on our experience of designing and evaluating mobile health (mHealth) information technology interventions in Canada, the United States, and the United Kingdom [5–7], we present here guidelines and methodology that we have learned in the implementation process of new technology and an overview of some of the current barriers and enablers specific to implementation of post-surgical site surveillance technology.
The Patient
Previously patients have been seen as passive recipients of healthcare, but increasingly it seems that patients are willing to be engaged in their own care. To promote adoption of technology by patients, the strategic use of focus groups and co-design are two high-yield methods of patient engagement [7–10]. It is a myth that smartphones and tablets will never be used by an aging population. Increasingly, it is a favorite way of staying connected with grandchildren, family, and friends. The penetration of mobile devices in the aging population is on the increase worldwide [11]. Recognizing the preferences of different age groups, such as the frail elderly and younger teenage patients, can dictate the design of user interface that will improve user ability. Fundamentally, compliance and engagement are totally dependent on co-design (Table 1).
Principles of Successful Implementation of New Technology for Patients
Effective design thinking on the appearance of the user interface must be intuitive. The size and color of touch screen buttons can make a difference in uptake by certain groups (Fig. 1). Appropriate questions specific to the recovery and surgical procedures are important. Having the survey text available in multiple languages is essential in providing comprehensive patient care to the entire community. Using incentives, such as deploying gamification or offering iTunes certificates as reward for completion of online surveys, have worked well in some projects. We have also found that patients want to know when the information that they have entered has been reviewed by a care provider [6]. With this in mind, thorough education and onboarding are imperative for smooth handoff in home monitoring programs. Providing direct communication links to care providers can be a deterrent to provider engagement, because this may represent potential runaway responsibilities that may be considered extra work and be rejected as beyond scope of practice. Patient-initiated texting back to the care provider and return email options within the technology can work under controlled scenarios but must be curated carefully. It must be clear to the patient that mHealth communications should not supplant normal emergency protocols, such as dialing 911. Patients must understand that this is a monitoring system and that the connectivity is between 9:00 and 5:00 not 24/7. There are expectation management issues on both sides of the system.
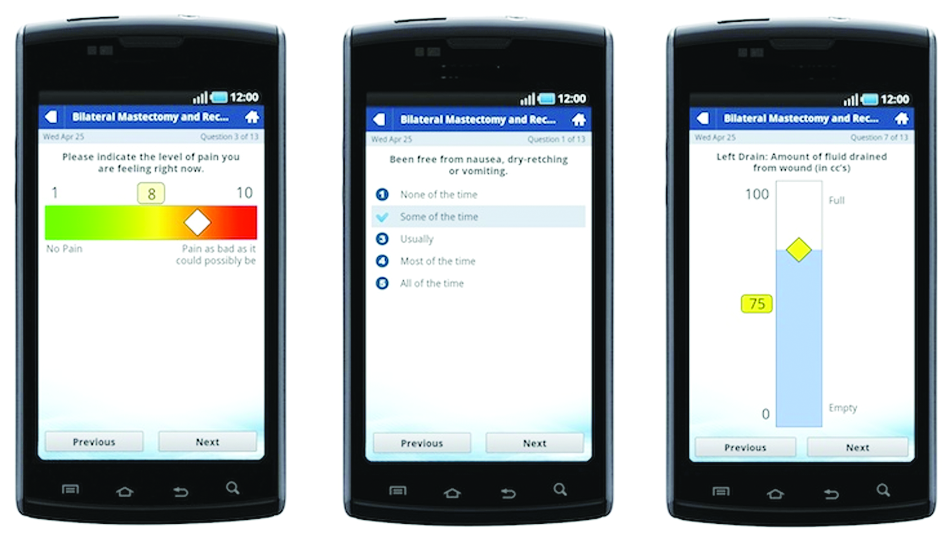
Examples of the touchscreen interface of the patient portal, including the visual analogue pain scale, an example of the questions on post-operative nausea, and the visual analogue scale for fluid in the post-operative surgical drains. Color image is available online.
Digital photographs of surgical sites and surgical site infections are another important aspect of mobile monitoring and remote surveillance programs. This year more than a trillion digital pictures will be taken globally on smartphones. The ability of any population to take discriminating high-quality photographs with their cell phone is now considered an innate curatorial ability. Sequential pictures of a surgical site can provide a unique window on normal healing processes and potentially reveal early development of surgical site infections (Fig. 2) [7]. Indeed, there is much focus on developing predictive analytics using digital photographs to elicit clues regarding early warning signs that could trigger preventive interventions before the onset of a fulminating post-operative infection.
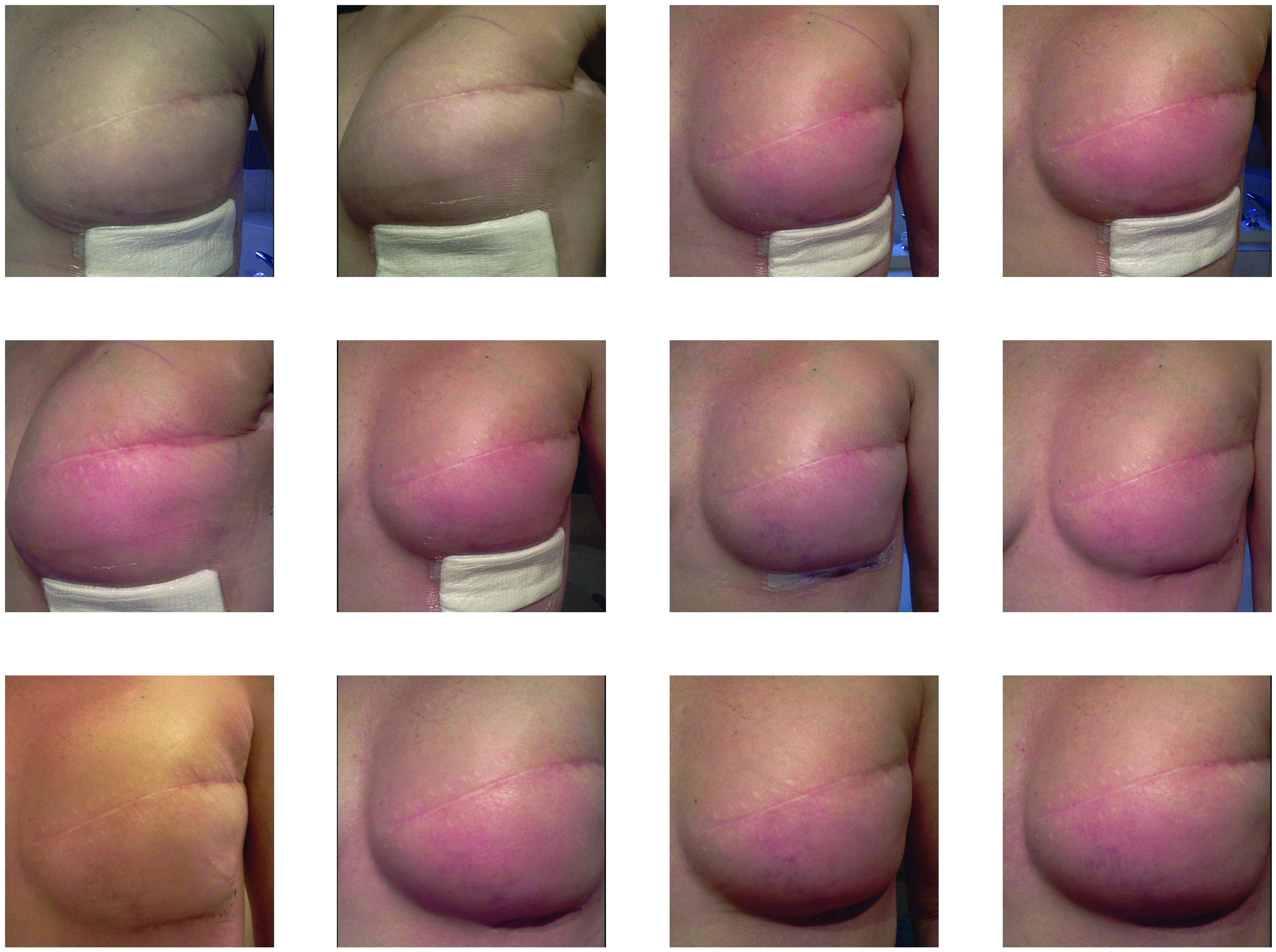
Shows a selected series of patient-entered digital photographs from a mobile phone. The sequential photographs show the left breast of a patient after insertion of a tissue expander, where the surgeon identified an increasing erythema at 10 days post-operation. Although there are lighting irregularities the pictures are of reasonable quality. The camera quality on most mobile phones is capable of detecting subtle changes in skin tone. Color image is available online.
Care Providers
Just as co-design methods such as focus group engagement are critical for the successful uptake of technology with patients, the same holds true for providers, because this presents a forum to address motivations and uncover tensions regarding care coordination. One of the main components of successful implementation of new technology for care providers is to identify real opportunities to improve workflow patterns that make sense within care pathways while improving standard of care for patients. In trying to anticipate what flow adjustments would be important to specific surgical care pathways, eliciting consensus among the medical staff is key to successful adoption. Table 2 presents principles of successful implementations related to care providers.
Principles of Successful Implementation of New Technology for Care Providers
EHR = electronic healthcare record.
The sudden availability of a large volume of new patient data on a daily basis initially may seem to be an improvement but can cause concern among care providers because this may represent additional workload and increased responsibilities on top of current job descriptions. The design of provider-facing platforms for remote monitoring of patients should incorporate strategies to address these concerns (Fig. 3). Unionized allied professionals may feel that using patient monitoring technology is outside their scope of practice as described in existing institutional contracts. It is important to identify clearly what characteristics are being measured, what data types are collected, and the potential impact of these data on patient care.
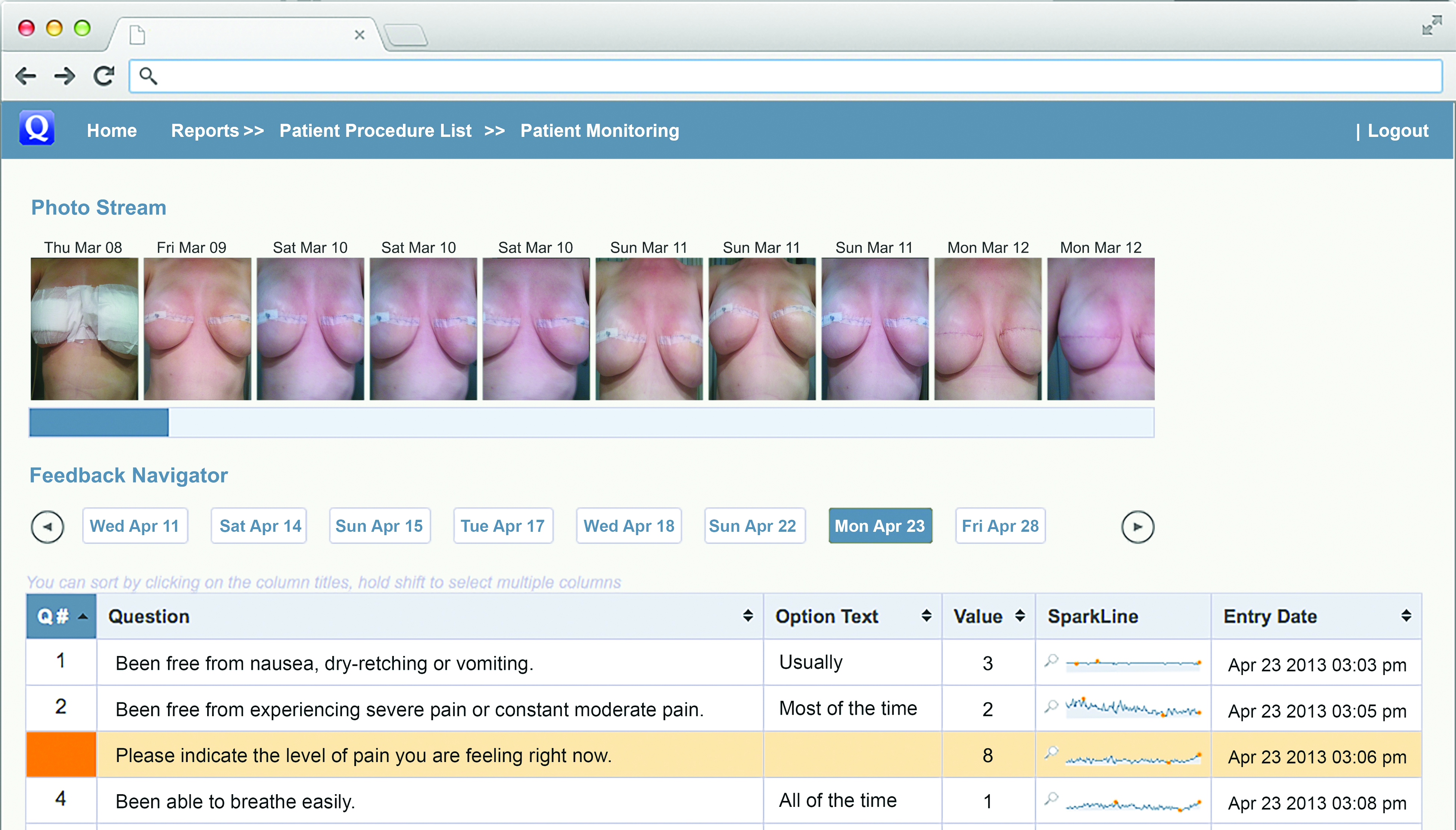
Image of the surgeon's dashboard. The surgeon or care provider can view the patient's quality of recovery on one screen. The photographs show the patient's own pictures of the surgical site with the date. The Quality of Recovery questions are listed with the patient's responses. Question #3 is highlighted because of the abnormally high pain score entered by the patient. The spark-line represents every score as a point of data on that particular indicator since the start of the monitoring. The pictures can be enlarged by tapping on them. (Used with permission from ©John L. Semple, Sarah Sharpe, M. Lucas Murnaghan, John Theodoropoulos, Kelly A. Metcalfe. Originally published in JMIR mHealth and uHealth [http://mhealth.jmir.org]). Color image is available online.
Measuring “success metrics” within the technology to audit whether the technology is actually doing what is intended should be collected at different milestones [6,8,9]. This type of feedback loop for care providers confirms the original concept as worthy, establishes a platform for modification of the program, and supports efforts and funding for sustainability of the program. New concepts such as virtual clinics, how virtual scheduling is created, and how virtual visit data are documented and tracked in different electronic medical record systems must be established and resolved with new technology. Additional limitations include concerns about physician compensation for care delivered by new technologies, such as mobile applications, and the possibility that access to these technologies may be limited to patients who can afford it or are able to understand how to use it.
Implementation Challenges in Administration and Institutions
Institutions and hospitals are interested in adopting innovation but are risk-averse for valid reasons. Cloud servers and other IT concepts are often presented as confusing and current U.S. Food and Drug Adminstration standards and regulations are still somewhat vague [9]. Many institutions have some form of digital technology established that may not integrate with new vendor specifications. Electronic healthcare record (EHR) vendors are reluctant to integrate other types of software and can be obstacles to data integration. Electronic healthcare record firewalls and legacy software components may preclude upgrades or introduction of new technology outside their stable of products. New technology with proven privacy and security standards with Health Insurance Portability and Accountability Act (HIPAA) and Personal Health Information Protection Act (PHIPA) compliance are important. This is a key element for smooth implementation that covers the concerns of all areas discussed here: the patient, the care provider, and the institution/healthcare system (Table 3). Best practice for privacy is essential, which includes multiple levels of encryption (both in-transit and at rest) anonymized data and being aware of cloud regional jurisdiction regulations [10,12]. Clinical photographs must be in a secure folder both within EHR storage and on mobile devices [7,12].
Principles of Successful Implementation of New Technology for Institutions and Hospitals
EHR = electronic healthcare record.
Discussion
The successful implementation of mHealth and mobile technology concepts are often viewed as a prime example of complex health interventions, given the interaction of individual, contextual, and technological variables. However, mobile applications and telemedicine in general have been shown to improve the care transition of postoperative patients from institution to home [7–9,12,13]. The overall benefits of post-operative monitoring using mobile applications have seemingly addressed all the triple aim objectives including the simultaneous pursuit of the three aims: improving the experience of care, improving the health of populations, and reducing per capita costs of healthcare [14]. Despite the evidence-based and innovative programs available to institutions and hospitals there is little understanding of how healthcare facilities purchase, implement, and adopt technology.
Theories and models currently used when investigating technology, technology adoption, and implementation mainly focus on how the end users (patients) adopt technology, and describe methods, interventions, and variables that promote the use of evidence-based practice [15]. This approach does not entirely address the complexity of the implementation framework within the context of the patient, the care provider, and institutional characteristics as variables [15,16]. To be successful, an all-encompassing approach is needed to investigate and understand the key stakeholders and their different needs and requirements [16,17]. Here we present guidelines on several of the variables in the implementation of new healthcare technology. Each has unique and overlapping requirements that if addressed and respected can lead to a more successful adoption and implementation.
Footnotes
Acknowledgments
This work was supported by U.S. Centers for Disease Control and Prevention (CDC) award #200-2016-91803 through the Safety and Healthcare Epidemiology Prevention Research Development (SHEPheRD) Program, which is managed by the Division of Healthcare Quality Promotion. The content is solely the responsibility of the authors and does not represent the official views of the CDC.
Author Disclosure Statement
J.L.S. holds shares in QoC Health Inc. which is a mHealth technology company from which the graphics interface in the figures are sourced. H.E. is an advisor for Tetraphase. None of the other authors have any disclosures.