
Abstract
Background:
While ubiquitously multi-resistant bacteria are on the rise, peri-operative antimicrobial prophylaxis in trauma and near-to-bone surgical procedures has only been changed slightly during the last 25 years. Recent clinical studies concerning the bacterial spectrum and efficacy of antimicrobial treatment in infected trauma surgical patients are rare. The aim of the study was analysis of the contemporary bacterial spectrum and its antimicrobial resistance including the assessment of the appropriateness of peri-operative antimicrobial prophylaxis with cefuroxime.
Methods:
Patients of a level-I academic trauma center who underwent open or arthroscopic surgery because of a recent trauma necessitating the use of bone-near metal implants were included in the study. All patients in whom a surgical site infection (SSI) had developed during six weeks post-operatively necessitating surgical debridement and had positive microbiologic culture results from an intra-operative surgical site swab were analyzed, retrospectively. In particular, age, gender, date and duration of surgical interventions, and patient's related risk factors were collected, and infecting agents and their minimum inhibitory concentration values for 34 selected antimicrobial agents were evaluated. An SSI occurring later than 6 weeks post-operatively and patients with chronic and septic wounds were excluded. Statistical analysis was performed with SPSS® (IBM, Armonk, NY).
Results:
There were 438 pathogens cultured in specimens from 303 enrolled patients (female = 140, male = 163). The most frequent pathogens were Staphylococcus aureus (27.1%), S. epidermidis (20.6%), Enterococcus faecalis (13.6%), Escherichia coli (5.1%), and Pseudomonas aeruginosa (3.7%) accounting for 303 isolates. Of those, 89 (29.4%) were multi-resistant. Of the S. epidermidis isolates, 79.8% (n = 71) were resistant against Oxacillin and thus against most beta-lactam antibiotic agents. Altogether, only 44.1% of the infecting organisms were susceptible to cefuroxime, the antimicrobial agent most often being used for prophylactic purposes.
Conclusion:
Standardized antimicrobial prophylaxis with cephalosporins has to be reconsidered critically. Multi-resistant species such as S. epidermidis are an increasing challenge in trauma operations.
Wound infections are one of the most serious complications in surgical treatment of patients down to the present day [1]. Because of multiple surgical procedures, long-term immobility, and increased length of hospital stay [2], patients with surgical site infections (SSI) are at high risk for thromboembolic events, nosocomial infections, and dependency on post-hospital care [3]. Occurring complications determine increased deaths [4].
Every SSI has both a burden to the patient and the physician as well as an economic charge for the treating hospital and health care system [5–8]. If causative pathogens possess augmented antimicrobial resistance, these effects are substantially intensified [9], not only affecting the therapeutic pathway [10].
After the introduction of antiseptic and later aseptic surgical techniques [11,12], the development of peri-operative antimicrobial prophylaxis schemes again were a major advancement. While the early use of penicillin in 1955 [13,14] soon became ineffective, later clinical studies laid the academic foundation of a standardized antimicrobial prophylaxis with cephalosporins [1,15–32].
Because of increasing use of antimicrobial agents, Guglielmo et al. [33] concluded that revision of the actual epidemiology and antimicrobial resistance of pathogens involved in SSI is needed periodically. Only a few studies, however, addressing the spectrum of bacterial species or antimicrobial resistance have been performed during the last 25 years [30–32]. More often, authors used data of previous research or paid more attention to the susceptibility rates for particular antimicrobial agents [1,34–36]. Others measured SSI rates while they paid no attention to the bacterial offenders [37,38].
While microbiologist research groups investigated the mechanisms of increased virulence, biofilm formation, and distribution of resistance mechanisms, clinical studies did not address bacterial species in detail, but mostly considered the amount of methicillin-resistant Staphylococcus aureus only [39–47]. Thus, a single shot peri-operative antimicrobial prophylaxis with cephalosporins is still the standard prophylaxis in many instances [48,49].
This study was performed to assess any change in spectrum of the offending infective agents and their antimicrobial resistance causing early SSI and to analyze whether or not peri-operative antimicrobial prophylaxis with cephalosporins meets the current challenges.
Methods
A retrospective analysis of all patients who underwent open or arthroscopic surgical procedures because of a recent trauma necessitating the implantation of a metal medical device was analyzed. The patients were treated in a level-I academic trauma center during the period January 2007 until December 2012 (n = 13,800). Standardized antibiotic prophylaxis was performed with cefuroxime 3 g intravenously. All patients in whom an SSI developed during the six weeks after the primary intervention and had positive microbiologic culture results were included in the study. Patients with isolated soft tissue trauma, chronic and septic wounds present at the first operation, or clinical infection necessitating treatment before operation were excluded.
Diagnosis of SSI was made by trauma surgery consultants and residents in trauma surgery under supervision of an infectious disease consultant, respectively. Because of a lack of minimum inhibitory concentration (MIC) data from November 2009 until September 2010, patients who underwent surgical procedures in this period had to be excluded as well.
Patients' related data were included into a Microsoft Access 2010 (Microsoft Corporation, Redmond, WA) database as follows: Date of birth, gender, risk factors (diabetes mellitus, current smoking, hazardous alcohol consumption [>30 g/d in males and >20 g/d in females, respectively], obesity [body mass index >30 kg/m2], immunosuppression), date of admission and discharge, date and duration of trauma surgical intervention, death within hospital stay, International Statistical Classification of Diseases and Related Health Problems (ICD-)10 (ICD-10-2018-GM) and AO-classification of the trauma, associated soft tissue trauma, code of surgical procedure, dates of operations after clinical diagnosis of SSI, specimen sent to microbiologic laboratory.
Microbiologic analysis was performed by plating on appropriate solid media and broth enrichment. Grown strains were identified by commercially available biochemical test kits (API 20E, API 20NE, API Staph, API 20 Strep, API Coryne, API 20A, BioMerieux, Lyon). The MICs of 34 selected antimicrobial agents were established employing broth micro-dilution procedures according to ISO 20776-1. Case-related qualitative and quantitative results for species identification and respective MICs were included into the database. Age at operation, length of stay, pre-operative and post-operative days were calculated by Microsoft Access.
Statistical analysis was performed with SPSS (IBM Corporation, Armonk NY) by unexceptional exact testing. All dichotomous values were tested by chi-square test or Fisher exact test. Quantitative values were checked for normal distribution (Kolmogorov-Smirnov test) and association. If a normal distribution was found, the Student t test was used for statistical evaluation. Values without normal distribution were statistically examined with the Mann-Whitney U test.
Statistical analysis of quantitative values with normal distribution toward nominal items was performed with a one-way analysis of variance. Levels of significance were adjusted according to Bonferroni if necessary. Antimicrobial resistance was defined by MIC values using European Committee on Antimicrobial Susceptibility Testing 5.0 guidelines [50] and graphically expressed using Microsoft Excel 2010 (Microsoft Corporation, Redmond, WA).
Results
Overall, 303 patients (w = 140, m = 163) were enrolled. Because of a trauma at two independent times and an early infection in different anatomic sites, two patients (w = 1, m = 1) were included twice (Table 1). The 303 patients had 384 fracture diagnoses. Mean age at the time of surgical procedure was 62.9 years (range 16–97 y, standard deviation [SD] 20.04 y). Women were significantly older (mean 72.0 y, SD 17.7 y, range 16–97 y, p < 0.001) than men (55.1 y, SD 18.7 y, range 19– 96 y). Fourteen patients (w = 7, m = 7) died during in-hospital treatment. Mean length of stay was 29.21 days (range 1–173 d, SD 24.29 d). Infection rate of early SSI was 2.2%.
Patient Characteristics
BMI = body mass index.
Mann-Whitney U test.
t test.
Fisher exact test.
Significant (adjusted according to Bonferroni).
Significantly more smokers (p < 0.001) and hazardous alcohol consumers (p < 0.001) were found in men than in women. Further, men more often were affected by AO type C fractures than women (p < 0.001) while women more often had type A fractures (p < 0.001). There was no gender difference in type B fractures (p = 0.722). Open fractures (p = 0.002) and foot fractures (p = 0.009) were more frequent in men. Fractures of the femur were seen significantly more often in women (p < 0.001, Table 2). Open fractures were more frequent in patients younger than 60 years (p < 0.001).
Involved Anatomic Regions
Fisher exact test.
Significant (adjusted according to Bonferroni).
Mean duration of the operative procedure was 108.5 minutes. Differences between the surgical treatment duration of different body parts was statistically significant (p = 0.03). There was no significant correlation of operative time and infecting bacterial species (Table 3).
Time of Operational Procedure (min)
SD = standard deviation.
Significant one-way analysis of variance, p = 0.003.
Pathogen spectrum
Microbiologic cultures yielded 438 pathogens (435 bacterial strains and 3 Candida species). The most frequent bacterial pathogens were S. aureus (27.1%), followed by S. epidermidis (20.6%), Enterococcus faecalis (13.6%), Escherichia coli (5.1%), and Pseudomonas aeruginosa (3.7%), which comprised altogether 70.1% of total isolates (Table 4; Fig. 1). In comparison with amalgamated previous studies [1,15–20,22,23,25–28,30–32], the species prevalence described here was statistically different except for E. faecalis (p = 0.993). Finally, there was no age-related difference in the bacterial spectrum (Table 5).
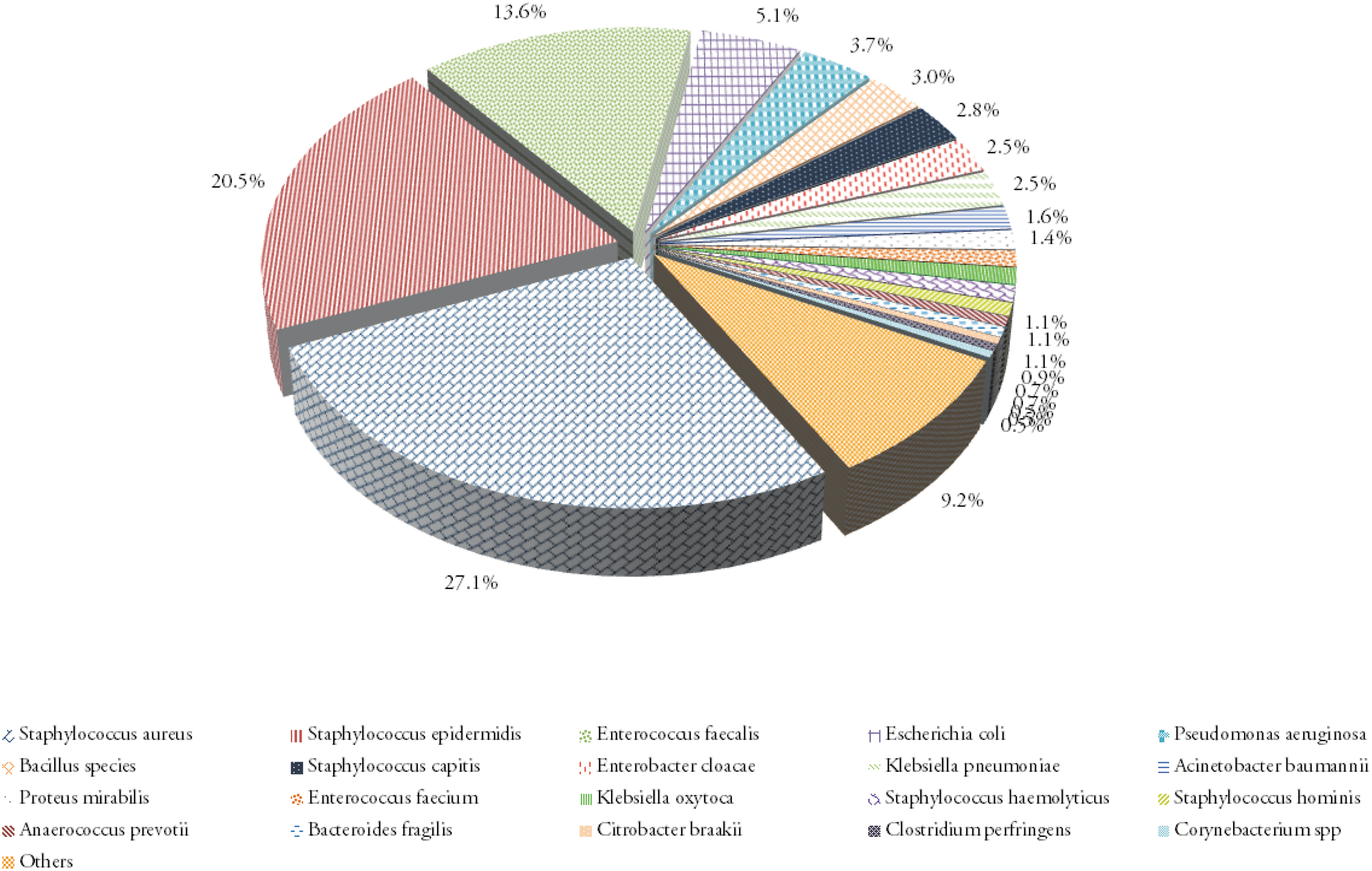
Simplified bacterial spectrum. Color image is available online.
Bacterial Spectrum
CI = confidence interval.
Fisher exact test.
Significant (adjusted according to Bonferroni).
Bacterial Spectrum in Comparison of Age and Gender
Fisher exact test.
Significant (adjusted according to Bonferroni).
Of the 435 bacterial pathogens, 235 strains were single isolates and 200 were found in mixed cultures (Table 6). There were 132 bacterial strains found in sites harboring two bacterial pathogens while 68 strains were detected in sites with more than two pathogens. In mixed cultures, E. faecalis was more prevalent than other species (19.7% vs. 8.9%, p = 0.005) while S. aureus was found less frequently in mixed than in single cultures (13.6% vs. 37.0%, p < 0.001). There was no statistical difference in the prevalence of bacterial species when sites yielding only one pathogen were compared with those infected with two or more species (Table 7).
Bacterial Spectrum in Multiply Colonized Surgical Sites
Fisher exact test.
Significant (adjusted according to Bonferroni).
Comparison of Surgical Sites with Two or More Cultured Species versus Monoculture
Fisher exact test.
Significant (adjusted according to Bonferroni).
Antimicrobial resistance
The current state of antimicrobial resistance of the five most frequent bacterial species in the observed population is depicted in Supplementary Figures S1, S2, S3, S4, S5. Low up to moderate levels of resistance were found in E. coli and E. faecalis with preserved susceptibility against established broad-spectrum antimicrobial agents. The E. faecalis strains, however, displayed high-level resistance against gentamicin in 69.5%. Of P. aeruginosa strains, 44.4% were resistant to ciprofloxacin, 33.3% had resistance to ceftazidime. Figure 2 shows resistance levels for cefuroxime and reference antimicrobial agents for selected bacterial strains.
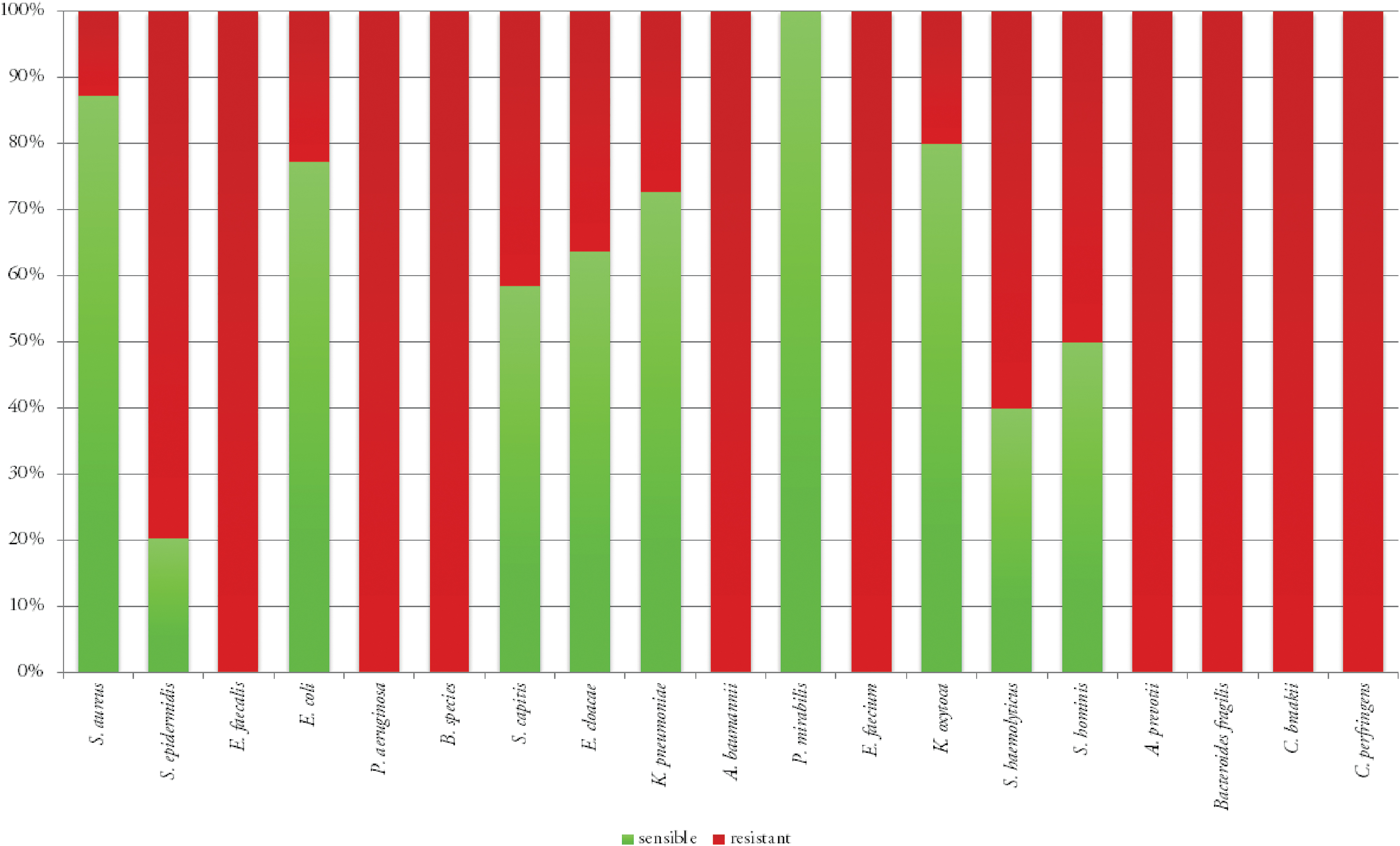
Resistance levels for cefuroxime and reference antimicrobial agents for selected bacterial strains. Color image is available online.
Not surprisingly, S. epidermidis strains showed a higher frequency of resistance against antimicrobial agents than of S. aureus isolates (Table 8).
Antimicrobial Resistance of Staphylococci against Selected Antimicrobial Agents
Fisher exact test.
Significant (adjusted according to Bonferroni).
Susceptibility against peri-operative prophylaxis with cefuroxime
Consider that 90.1% (n = 392) of all patient isolates, 55.9% (n = 219) of the strains were resistant to cefuroxime (Supplementary Fig. S5). In particular, 12.8% of S. aureus (n = 15), 79.8% of S. epidermidis (n = 71), and 22.7% of E. coli (n = 5) were resistant to cefuroxime. Eight species with intrinsic resistance against cephalosporins (24.8%, n = 108) were found within the 20 most frequent species.
Discussion
Common gender-related differences of AO type A and C fractures were found in this study [51–53]. Duration of trauma surgical procedures was an independent risk factor for SSIs [54–56]. Bacterial species causing the SSI were not statistically correlated with the duration of the operation. The origin of the bacterial offenders, the way of transmission, and the extent of exogenous and endogenous infection must remain speculative.
Because of people's high mobility and worldwide prevalence of multi-resistant pathogens [57–65], periodic revision of the epidemiology of pathogens causing SSIs and their antimicrobial resistance is needed [33,66–68]. Continuous surveillance and permanently high hygiene standards [69,58] may reduce the use of broad-spectrum antimicrobial agents and prevent outbreaks of highly resistant strains [35,43,47,70].
Principally, the pathogens found in SSI did not differ from previous publications [1,15–20,22,23,25–28,30–32], but the prevalence of individual species was significantly altered. Today, S. epidermidis can be found in SSIs more frequently, while strains of S. aureus and E. coli were found less often than 20 years ago. Statistical analysis was performed in comparison with the greatest coherent study population [1]. These differences, however, in part may be because the appraisal of the pathogenic potential of [71]. coagulase-negative staphylococci has changed over time, especially for S. epidermidis [71].
Mainly, S. aureus occurred in single cultures (15.5% vs. 37.0%, p < 0.001), which is indicative of its unique virulence. Malic at al. [72] found growth inhibition of other species in biofilms by S. aureus and P. aeruginosa. Formation of biofilm by S. aureus has been known for years. Many biofilm producing species demonstrate a wider spectrum of antimicrobial resistances [44]. Moreover, small colony variants of S. aureus appear to possess proteins related to Streptococcus suis that facilitate temporary intracellular persistence [41]. Thus, S. aureus can persist in sites for a longer time if antimicrobial agents that are just distributed in the extracellular compartment are used for treatment.
The ever-increasing use of medical implants allows biofilm producing bacteria such as S. epidermidis to evade more often non-specific immune mechanisms as well as to escape antimicrobial agent effects [42,73,74]. Kocianova et al. [40] found secretion of poly-γ-DL-glutamic acid (PGA) by S. epidermidis previously found in Bacillus anthracis. Hence, these characteristics cause the rise of virulence even in immunocompetent patients despite earlier reports to the contrary [41]. Therefore, current research activities aim at preventing biofilm formation on implant surfaces [42,75].
Staphylococcus epidermidis occurred in single and mixed infections. Improved mechanisms of cross-communication of antimicrobial resistance genes [41] and high genetic flexibility [42,45,73,76] may contribute to the increased antimicrobial resistances against several agents in S. epidermidis strains compared with strains of S. aureus [46].
In this study, the prevalence of E. faecalis was similar to that in earlier reports [1,15–20,22,23,25–28,30–32]. This might in part be because of continuous selective pressure of cephalosporin prophylaxis. All strains found in the study population were susceptible to imipenem, linezolid, vancomycin, and teicoplanin. Cross-communication of resistance genes by E. faecalis, however, is known [77], allowing acquisition and transfer of antimicrobial resistance in mixed cultures. The high resistance levels to gentamicin by E. faecalis strains should be considered in local treatment with strings and sponges containing antimicrobial agents [78,79]. Altogether, the still limited resistance seen for E. faecalis is suggestive of endogen sources of these micro-organisms [80].
With a prevalence of 3.0% (n = 13), Bacillus species were the sixth most frequent isolates. A statistical correlation with open fractures was not found. Sporulation allowing ineffectiveness of alcohol-based skin disinfection [81] and high resistance against cefuroxime (84.6%) might result in a selection advantage for bacilli. A contamination of patient's skin at hospital admission cannot be verified because of the ubiquitous prevalence of these organisms.
Levels of antimicrobial resistance of P. aeruginosa isolates match earlier reports [82]. Interaction and joint production of virulence factors by P. aeruginosa and S. aureus were found by Pastar et al. [83]. Interaction is performed by quorum sensing [84]. Mixed isolates of S. aureus and P. aeruginosa were found in four cases in this study.
More than a half of all infecting strains were not captured by the peri-operative antimicrobial prophylaxsis with cefuroxime. Whether this percentage is driven by the use of this agent for prophylaxis cannot be determined because data for patients operated on without peri-operative antibiotic agents are not available. Mono-center studies as reported here involve the danger of a locality bias. On the other hand, meta-analyses suggesting a peri-operative prophylaxis with cephalosporins rely on research data of 1970 until 1999. [34]
Thus, the questions arise as to whether the current standardized antimicrobial prophylaxis is still appropriate in view of the data reported here. This might argue for new studies on peri-operative antimicrobial prophylaxis in a multi-center double blind randomized clinical trial with high numbers of cases fulfilling strictest medical and ethical criteria.
Because this was a single center study with a limited sample size, our findings cannot be generalized worldwide. Nonetheless, the spectrum of bacterial species found here was comparable to that in previous reports. This study, however, showed a change in the prevalence and resistance of the species causing SSI. Thus, it seems necessary to monitor the epidemiology of SSI continuously.
Conclusion
In this study, standardized peri-operative antimicrobial prophylaxis with cefuroxime captured only 44.1% of the later found organisms causing early SSIs. Thus, it might be time to reconsider the current approach. Bacterial species prevalences have changed significantly during the last 25 years. Infections caused by multi-resistant and biofilm producing species like S. aureus, S. epidermidis, and E. faecalis are on the rise. Local knowledge of bacterial strains causing infections and antimicrobial resistance is the pre-condition for a sufficient antimicrobial prophylaxis.
For current patients at risk or with multi-resistant strains, a single shot prophylaxis with vancomycin or linezolid may be an option. Further individual regimes should be assessed in a common decision by the local Antibiotic Stewardship Team. Nevertheless, further clinical and experimental research is needed to comprehend the development of virulence in certain species as well as to design colonization-inhibiting medical implants to make a targeted antimicrobial prophylaxis possible.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.