
Abstract
Background:
The aim of this study is the evaluation of clinical signs and outcomes of treatment in children under five years of age who underwent appendectomy because of acute appendicitis.
Patients and Methods:
From January 2009 until December 2018, 90 patients (54 boys and 36 girls) younger than five years of age, treated with appendectomy because of acute appendicitis, were included in this study. Patients were divided into two groups, depending on the intra-operative finding of non-perforated (Group I; n = 32) or perforated (Group II; n = 58) appendicitis. The groups were compared regarding demographic, clinical, and laboratory data and outcomes of treatment.
Results:
Of 1687 appendectomies in this period, 90 (5.3%) of them were performed in patients aged five years or younger. There were 58 (64.4%) patients with perforated appendix. Positive correlation between the rate of perforation and the age of patients was found. Perforation rates were significantly higher in younger patients (100%, <1 year; 100%, 1–2 y; 83.3%, 2–3 y; 71.4%, 3–4 y; 78.6%, 4–5 y, and 47.3%, 5 y) (p = 0.037). Vomiting and diarrhea were found more commonly in the group of perforated appendix (p < 0.002, p < 0.001), while constipation was found more often in the patients whose appendix was not perforated (p < 0.001). The median duration of symptoms (48 h vs. 16 h; p < 0.001) and median duration of hospitalization (7.5 d vs. 5 d; p < 0.001) were notably longer for the group of patients with perforated than the group of patients with non-perforated appendix. All complications occurred in the group of perforated appendix with total incidence of 4.4%.
Conclusion:
The clinical presentation of acute appendicitis for children aged five years or younger is often unusual, and establishing the proper diagnosis is often delayed. Patient age is tied closely to the stage of acute appendicitis, so the youngest patients present with more advanced stages of disease and are at greater risk of perforation. Acute appendicitis should be considered in all cases where a child is having abdominal pain, fever, and diarrhea, which has been shown to be present significantly more often in children with perforated appendix.
Acute appendicitis is the most common emergency in the department of pediatric surgery, and it is most frequent in the second decade of life. Classic clinical appearance is present only in one third of all patients. Clinical appearance in the patients younger than five years of age, however, is often atypical, and misdiagnosis in this age group is not rare, which can lead to an increased rate of perforation [1,2]. Perforation in this age group often leads to diffuse peritonitis, and the most important thing in the management is to establish the diagnosis and perform surgical treatment, assisted by broad-spectrum antimicrobial therapy [3]. In older children, clinical data, physical examination, and laboratory results are sufficient in most cases to establish diagnosis [4].
The differential diagnosis of acute appendicitis includes gastroenterocolitis, mesenteric lymphadenitis, Meckel diverticulitis, inflammatory bowel disease, right lower lobe pneumonia, urinary tract infections, and intussusception, particularly in young pre-verbal children [5]. Perforation rates in this age group are significantly higher than in older children. Depending on patient age, between 30% and 75% of patients could have perforated appendix at the time of diagnosis [1]. Laparoscopic appendectomy is the main method for managing acute appendicitis in children resulting in shorter hospitalization, faster recovery, less post-operative pain, and reduced rates of post-operative complications [6,7].
The aim of this study was to analyze clinical presentation and outcomes of treatment in patients aged five years or younger who were treated with appendectomy because of acute appendicitis within a 10-year period.
Methods
Patients
A total of 90 patients, under five years of age who were treated with appendectomy because of acute appendicitis between January 1, 2009 and December 31, 2018 in the Department of Pediatric Surgery, University Hospital of Split, Croatia, were included in this retrospective research. Patients of both genders, aged five years or younger whose diagnosis was confirmed by pathohistologic analysis were included in this study. Patients older than five years of age, patients who did not have complete medical documentation, and patients in whom another cause of abdominal pain was found during the surgical procedure were excluded from this study.
The medical records of all patients included in the study were reviewed retrospectively. Depending on the intra-operative finding, patients were sorted into two groups: the first one included cases of non-perforated appendicitis (n = 32), while the second one included cases of perforated appendicitis (n = 58). The following parameters were noted for all patients: demographic data (age, gender, body mass index [BMI]); pre-operative laboratory results (white blood cell [WBC] count, neutrophil count, C-reactive protein [CRP] concenration); clinical findings (duration of symptoms, body temperature, local findings, nausea and vomiting, constipation, diarrhea, pain, anorexia); and treatment outcomes (duration of hospitalization, rate of reoperations, and post-operative complications).
All children with perforated appendicitis received antibiotic therapy. Children with uncomplicated appendicitis received post-operative antibiotic agents only if they were febrile with highly elevated inflammatory markers. In some cases, when a large amount of infected fluid was found in the abdomen during exploration, antibiotic agents were prescribed.
Operative technique
The method of operation was a free choice of the surgeon. All surgical procedures were conducted under general anesthesia in emergency settings. Open appendectomy was performed through a modified Lanz incision [6], while laparoscopic appendectomy was performed using a three-trocar technique [7,8].
Outcome measurements
The primary outcome measures were incidence and clinical appearance of acute appendicitis in patients aged five years or younger. The secondary outcome measures were rate of post-operative complications and reoperations and length of hospitalization. Potential post-operative complications involved secondary surgical site infections, intra-abdominal abscess, internal bleeding, bowel obstruction, and post-operative ileus.
Statistical analysis
The data were analyzed using SPSS 24.0 (IBM Corp, Armonk, NY) software program. Medians and inter-quartile ranges (IQRs) were used to present distribution of quantitative parameters, and the Mann–Whitney U test was used to test differences in median values between the groups of patients. Categoric data were presented with absolute rates and percentages, and the chi-square and Fisher exact test were used for the statistical analysis. All values of p < 0.05 were deemed statistically significant.
Results
The entire number of patients treated with appendectomy because of suspected acute appendicitis during the time frame of the study was 96. Six patients were excluded from the study because they met at least one exclusion criterion. Ultimately, 90 patients with median age of 4 years (IQR 3, 5) and median BMI of 14.4 kg/m2 (IQR 12.8, 16.2) were included in the study. There were 54 (60%) boys and 36 (40%) girls. At operation, uncomplicated appendicitis was present in 35.6% (Group I; n = 32) patients and perforated appendicitis in 64.4% (Group II; n = 5 8) of patients. No significant differences were found between patients from the two observed groups regarding gender and BMI (Table 1).
Demographic, Laboratory and Clinical Data of the Patients Who Underwent Appendectomy
IQR, interquartile range; BMI, body mass index; CRP, C-reactive protein.
Mann-Whitney test; bchi-square test; cFisher exact test.
Median age was significantly lower in the patients whose appendix was perforated (4 y; IQR (3, 5) vs. 5 y (IQR; 4, 5); p = 0.005). Younger patients had a greater chance of appendiceal perforation (100%, <1 y; 100%, 1–2 y; 83.3%, 2–3 y; 71.4%, 3–4 y; 78.6%, 4–5 y, and 47.3%, 5 y) (p = 0.037) (Table 2).
Influence of Age on Rate of Appendiceal Perforation
Chi-square test.
Abdominal pain (n = 90, 100%), anorexia (n = 72, 80%), vomiting and diarrhea (n = 61, 67.8%) were the most frequent symptoms in our study. Frequencies of other symptoms are shown in Table 1. No significant difference was noted between the two groups regarding frequency of pain (p > 0.999), nausea (p = 0.084), and anorexia (p = 0.103) at the time of the initial examination.
Diarrhea manifested more often in the patients with appendiceal perforation than in the patients whose appendix did not perforate (50% vs. 3.1%, p < 0.001) as well as vomiting (79.3% vs. 46.9%, p < 0.002). Constipation was observed more often in the patients with non-perforated appendicitis (p < 0.001). Symptoms lasted longer in the patients with perforated appendix compared with those whose appendix did not perforate (48 h vs. 16 h, p < 0.001) (Table 1, Fig. 1).
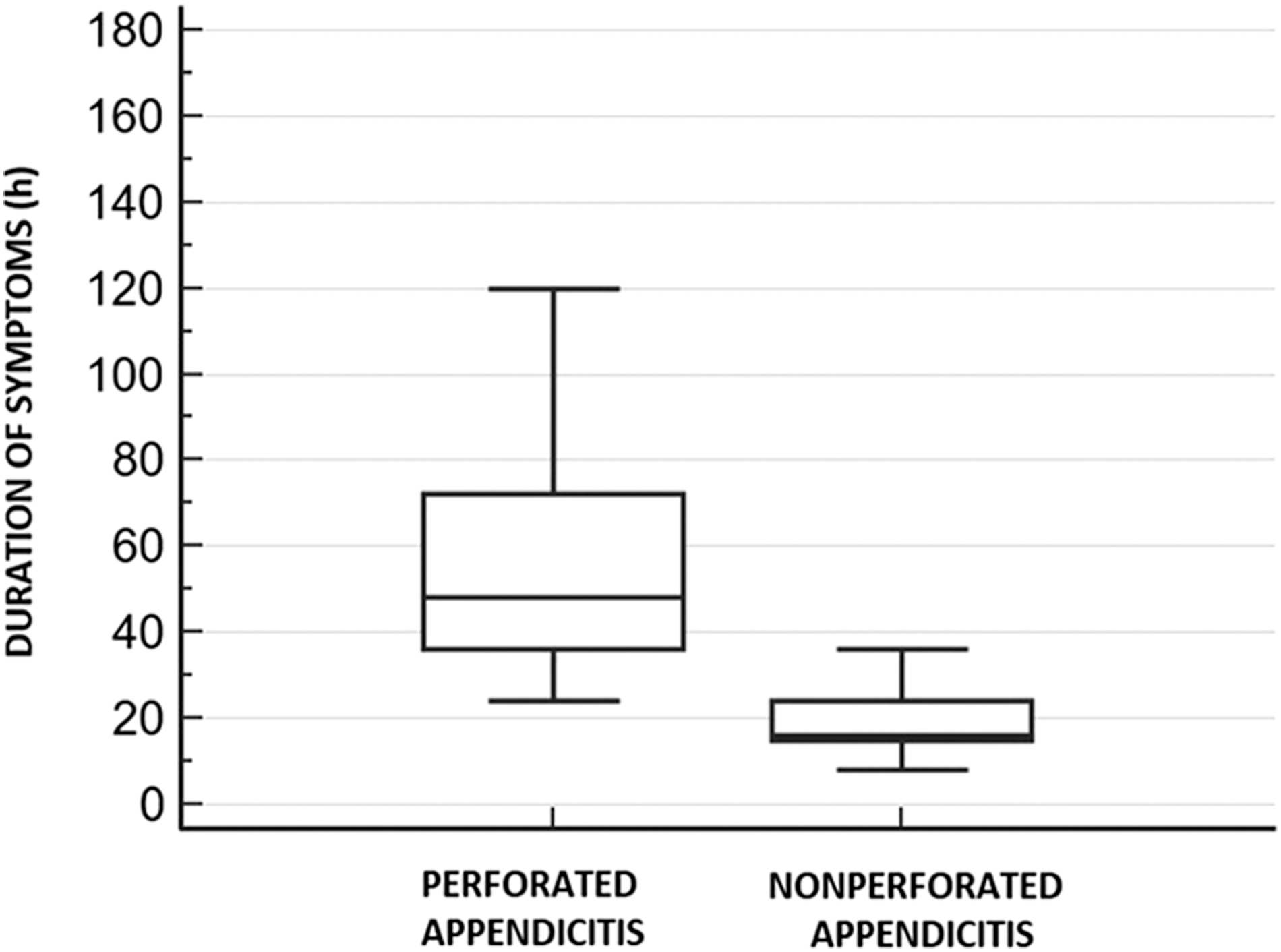
Box plot of duration of symptoms (h) in tested groups (p < 0.001).
Pre-operative laboratory values are shown in Table 1. Concentration of CRP (Fig. 2a), WBC count (Fig. 2b), and neutrophil count (Fig. 2c) were significantly higher in the patients with appendiceal perforation (p < 0.001).
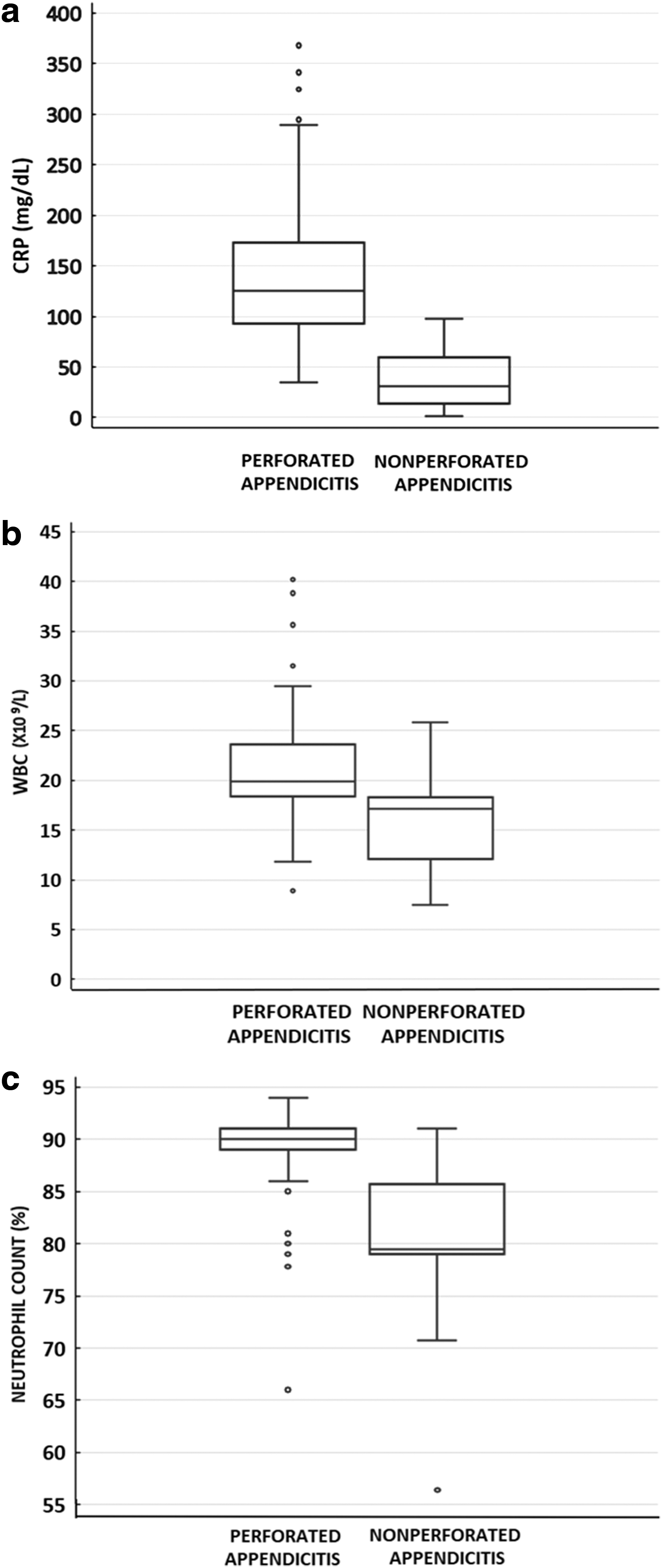
Box plots of pre-operative laboratory values (
The median hospitalization was 2.5 days longer in patients with appendiceal perforation (7.5 d vs. 5 d; p < 0.001) (Table 3, Fig. 3). Overall, the incidence of post-operative complications was 4.4%. Post-operative complications were recorded only in patients with perforated appendicitis (abscess rate was 2.2% and secondary surgical site infection rate was 2.2%). There were no statistically significant differences between compared groups regarding the approach for appendectomy. Rate of reoperation was 1.1%, and the only reoperation was performed on a patient with perforated appendix (p > 0.999) (Table 3).
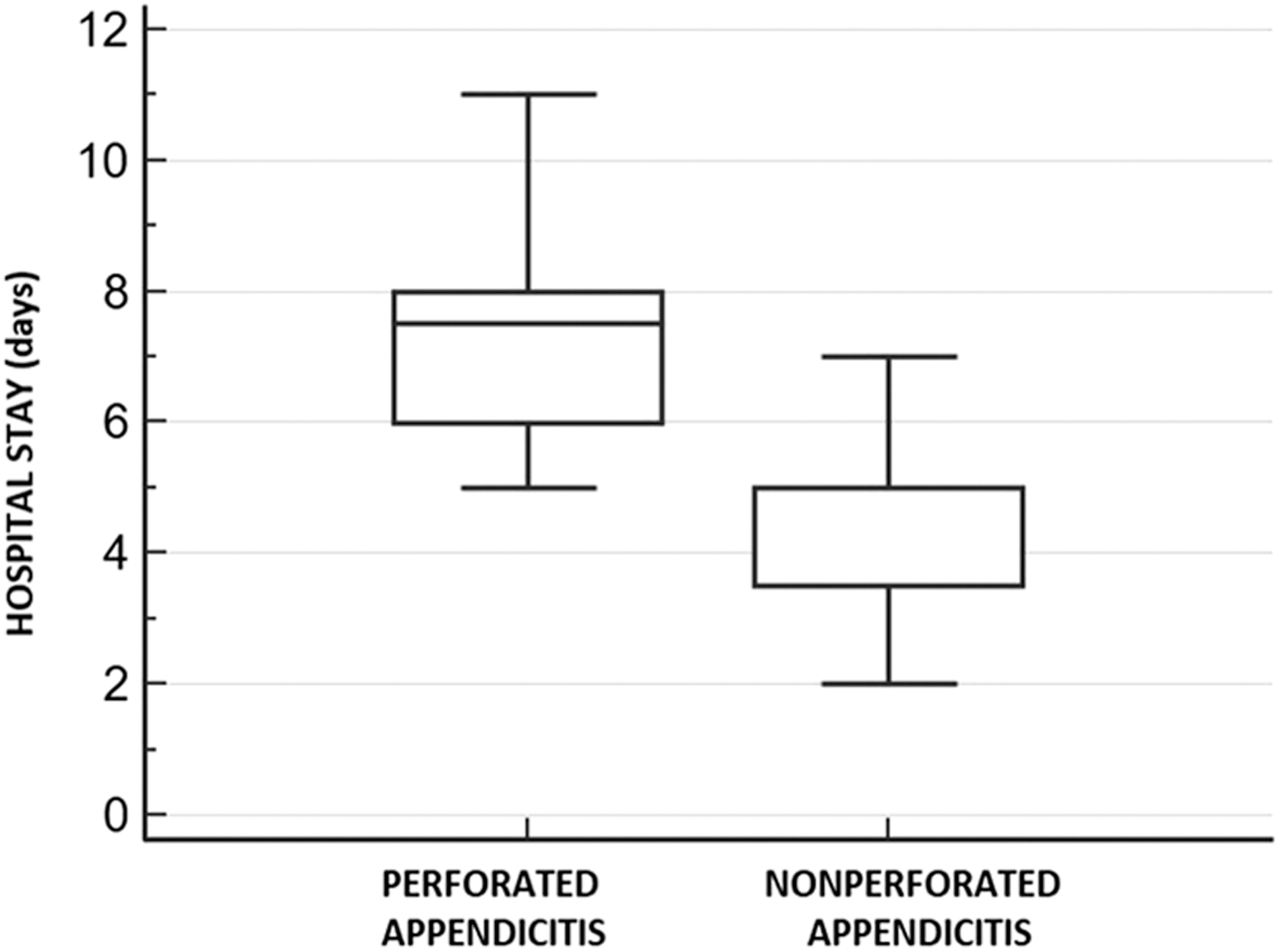
Box plot of hospital stay (d) in tested groups (p < 0.001).
Treatment Outcomes of Patients Who Underwent Appendectomy
IQR, interquartile range.
Mann-Whitney test, bchi-square test, cFisher exact test.
Surgical site infections were managed conservatively (surgical site drainage and dressing changes). One child with abscess was treated conservatively with intravenous antibiotic agents, and another was reoperated because of diffuse peritonitis. A total of 1687 patients under the age of 18 were treated with appendectomy because of acute appendicitis during the 10-year time frame of the study, and 90 (5.3%) of the operations were performed on patients aged 5 years or younger (Table 4).
Rate of Appendectomies in Children Aged 5 Y or Less In Total Number of Appendectomies
Discussion
This study has shown that acute appendicitis in children aged 5 years or younger is an uncommon condition with a rate of 5.3% compared with the entire pediatric population. Also, clinical presentation is often unusual, and initial misdiagnosis is frequent, which can lead to delayed diagnosis and increased risk of complicated appendicitis. Complicated appendicitis includes cases of peri-appendicular abscess and localized or generalized peritonitis and leads to significantly longer hospital stay. Our study has shown that in this age group, there is a higher incidence of appendiceal perforation, and the rate of perforation is inversely proportional to the age of children. Other authors published similar results [1,9–11].
Main limiting factors of this study are retrospective data collection and non-randomized comparison between the groups. A relatively small sample of patients included in the research may be one of the limiting factors, and others may or may not confirm these results.
In our study, main symptoms were pain, anorexia, nausea and vomiting, and diarrhea. Other authors published similar frequency of symptoms [1,5,9–13]. Diarrhea was more often present significantly in the patients with appendiceal perforation (50%) than in those with no perforation (3.1%), which can be attributed to the stimulus of the rectum by the adjacent peritonitis. Gougoudi et al. [14] concluded that this increased incidence of diarrhea in young children with appendiceal perforation should heighten awareness for the diagnosis.
The presence of diarrhea with elevated body temperature and abdominal pain is one of the reasons why children are often released home with the diagnosis of acute gastroenterocolitis, which is one of the most common conditions in the differential diagnosis [15,16]. Horwitz et al. [16] noted that history of diarrhea accompanied by abdominal pain and fever in the youngest patients should not be diagnosed as gastroenteritis; rather, these patients should be examined thoroughly with a high degree of suspicion for appendicitis. Therefore, diarrhea is a late symptom of acute appendicitis, and it would be optimal to establish the diagnosis before rupture.
Bickell et al. [17] reported the link between the duration of the symptoms and the probability of appendiceal perforation. They concluded that the chance of perforation is low in the first 36 hours of the disease and increases by 5% every 12 hours thereafter. We found a notable difference in the duration of symptoms between the observed groups, which is why concluded that one of the reasons for high rates of complicated appendicitis in this age group could be a delayed visit to the doctor. Similar to our results, Bansal et al. [1] revealed notable differences in the duration of symptoms between the groups of perforated and non-perforated appendicitis.
Younger children are at greater risk of appendiceal perforation with a rate of 100% in patients younger than one year, while the rate of perforated appendicitis in children aged five years was 47.3%. The results of a retrospective study published by Bansal et al. [1] have shown similar rates of perforation, while Nance et al. [9] have reported a slightly higher perforation rate (74%). Graham et al. [10] noted a 63% rate of perforation in patients aged younger than six years with acute appendicitis, including 100% in children aged two years or younger and 52% in children aged five years. This review was published in 1980 by Graham et al. [10], and, despite the advances in medicine in all fields, the results published almost four decades later showed about the same perforation rates for young children.
One of the most important parameters in establishing diagnosis is the laboratory data. Numerous scientists have tried to find a laboratory parameter that could provide a correct diagnosis in 100% of cases [18–20]. Not a single laboratory parameter has shown adequate sensitivity and specificity, however. The gold standard of laboratory parameters is still CRP and leukocytes with neutrophil count. In this study, children with appendiceal perforation had notably higher values of the acute phase reactants than the group of children with non-perforated appendicitis.
Contrary, Bansal et al. [1] published that leukocyte count has little significance in differentiation between perforated and non-perforated appendicitis. Nance et al. [9] have concluded that the total number of leukocytes is not predictable for perforation, but that neutrophil shift to the left is a significant parameter for establishing the diagnosis of acute appendicitis. Gougoudi et al. [14] concluded that despite a high incidence of leukocytosis in their patients, leukocyte count does not correlate with the histologic findings [14]. According to some authors, CRP has higher sensitivity than leukocyte count in assisting to make the diagnosis of perforated appendicitis [13].
In our study, duration of hospitalization was notably longer in patients with appendiceal perforation than in those without. The median difference between the two groups was 2.5 d, which means that children with perforated appendicitis stay longer in hospital and need more recovery time. Bansal et al. reported similar results [1].
Patients with perforated appendicitis had a slightly higher rate of post-operative complications, which could be one of the reasons for longer hospital stays. In our study, post-operative complications were rare (4.4%), and they only occurred in the patients with appendiceal perforation. Also, more frequent use of antibiotic agents in patients with perforated appendicitis is one of the reasons for a longer hospital stay. Bansal et al. [1] in their research reported a similar rate of post-operative abscesses of 3.2%. Sakellaris et al. [11] reported a somewhat higher rate of complications, but they also all developed in the patients with perforated appendicitis. The rate of secondary surgical site infection was 5%, and the rate of intra-abdominal abscess was 4%.
Conclusion
Acute appendicitis in patients aged 5 years or younger is not common and is often clinically atypical, which is one of the main reasons of late diagnosis that contributes to the high rate of complicated appendicitis. Our recommended algorithm of treatment for patients younger than five years presenting with acute appendicitis is shown in Figure 4.
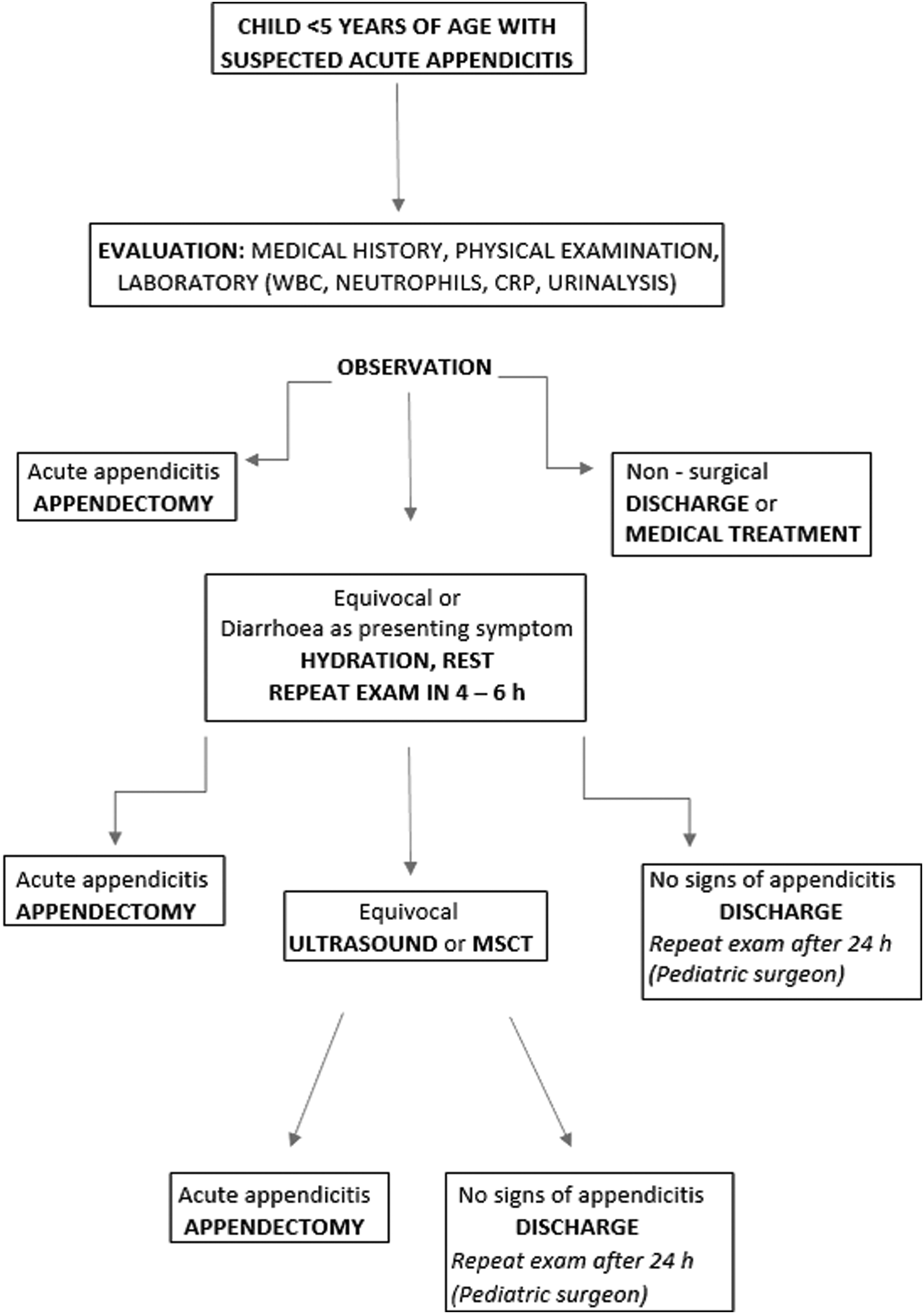
Algorithm of treatment of patients younger than 5 years with suspected acute appendicitis. White blood cell (WBC) count; C-reactive protein (CRP); MSCT, multi-slice computed tomography.
Footnotes
Author Disclosure Statement
No competing financial interests exist.