
Abstract
Objective:
To evaluate the efficacy and safety of topical negative pressure therapy/vacuum-associated closure (TPN/VAC) in the treatment of cephalic facial skin abscess with infection.
Methods:
Forty-seven patients with cephalic facial skin abscesses were divided into two groups. The observation group was treated with negative pressure sealing drainage technique and primary wound suture. The control group was treated with abscess incision and drainage first; the second stage was wound suture after three to five days. The time and times of wound dressing, the pain score during wound dressing, the time of antibiotic use, and the recurrence rate were observed.
Results:
The wound healing time of the observation group was seven days, which was better than that of the control group for 10–12 days. The time of dressing change in the observation group was 14.9 ± 2.0 minutes (11–19 minutes), and the time of dressing change in the control group was 14.6 ± 2.6 minutes (10–20 minutes). There was no difference between the two groups (p > 0.05). The total number of dressing changes per patient in the observation group was three to five times, and the total number of dressing changes per patient in the observation group was five to eight times. There was a statistically significant difference between the two groups (p < 0.05). The pain score of the observation group was 3.2 ± 0.6 points (2–4 points), and the pain score of the control group was 5.1 ± 0.8 points (4–7 points). The difference between the two groups was statistically significant (p < 0.05). There was no recurrence in the observation group and two cases in the control group.
Conclusion:
Local negative pressure closed drainage technology can shorten the patient's healing course and reduce the duration of treatment, reduce the pain of dressing changes, improve prognosis, and have satisfactory therapeutic effect. It is a simple, effective, and safe technology, which is worthy of clinical application.
Cephalic facial skin abscess is a common disease in outpatient clinics. Inflammatory reaction of abscess formation causes inconvenience and pain to patients because of redness, swelling, discomfort, and pain [1].The classic treatment was dressing change after incision and drainage and two-stage suture was performed after the pus cavity was cleaned. This method had a long course of treatment, and the daily dressing changes were painful and affected normal work and life [2].
In our study, topical negative pressure therapy/vacuum-associated closure (TPN/VAC) was used for outpatients who had cephalic facial skin abscesses. Secretion culture and drug sensitivity analysis were performed for pus and sensitive antibiotic agents were selected based on the results of the examination. This method can shorten the course of the disease, reduce the treatment duration, reduce the duration of antibiotic usages, and achieve satisfactory results.
Clinical Data
The study group comprised 47 patients with cephalic facial skin abscess. There were 31 males and 16 females, aged from 29.0 to 7.3 years (range, 16 to 48 years) with a disease course of three days to eight months, were collected from November 2017 to November 2018. In the observation group, 26 patients (17 males and 9 females with an average age of 28.4 ± 7.5 years) were treated with local negative pressure sealing drainage and primary wound suture. In the control group, 21 patients (14 males and 7 females, aged 29.9 ± 7.7 years) were treated with abscess incision, drainage, and secondary wound suture after three days. The choice of treatment methods was randomly determined by random data table. The age, gender, and course of disease were comparable between the two groups (p < 0.05).
Treatment
Topical negative pressure therapy/vacuum-associated closure in observation group
For the patients with cephalic facial skin abscesses, local infiltration anesthesia was performed 5 mm around the abscess to achieve the effect of nerve block. Approximately 0.8–1.0 cm long drainage orifice was incised at the most prominent part of the abscess. Secret culture and drug sensitivity tests were carried out in all patient's drainage pus. If there was a ruptured sebaceous cyst, its contents and capsule were removed. According to the results, sensitive antibiotic agents were selected for treatment. The pus cavity was washed repeatedly with hydrogen peroxide, iodophor, and saline until no obvious purulent secretion was found. A 1-mm long incision was made through the skin at the lowest end of the suppurative cavity standing position. The drainage tube with side wall opening was placed in the suppurative cavity along the prepared low drainage tunnel to the farthest end. The drainage tube was fixed on the skin with 5-0 nylon thread, and the wound was sutured intermittently along the whole skin layer with 6-0 nylon thread. Negative pressure suction was performed with a 20-mL syringe outside the drainage tube to ensure that the negative pressure was stable and that the drainage tube would not be dislodged.
The external negative pressure syringe was replaced for two consecutive days after operation. The wound was disinfected and dressed with iodophor routinely, and the drainage tube was kept in a negative pressure state. The drainage tube was removed 48 hours after the operation. After the drainage tube was removed, the residual pus was discharged by pressing the abscess. The drainage site, usually the size of a pinhole, can close naturally. Suture removal was performed seven days after drainage.
The abscess was incised and drained, secretions were taken for bacterial culture, and a drug sensitivity test was carried out. Sensitive antibiotic agents were selected for treatment according to experience. The cavity was repeatedly rinsed with hydrogen peroxide, iodophor, and saline and packed with sterile gauze containing compound polymyxin B ointment (Zhejiang Rishengchang Pharmaceutical Co., Ltd., Chinese medicine quasi-word H20061269). After daily dressing change to achieve fresh wound tissue and no secretion, local debridement and suture were performed. After operation, the residual secretion was drained with a drainage rubber sheet made of sterile gloves, and the drainage rubber was removed one to two days after operation. Sutures were removed seven days after debridement and suture.
Statistical Methods
Data were processed by SPSS 21.0 statistical software (IBM Corp, Armonk, NY). The measurement data were expressed as
Results
The results of pus culture of patients are shown in Table 1. The results of comparisons of therapeutic effects between groups are shown in Table 2. The posterior earlobe abscess and the scar are shown in Fig. 1 and Fig. 2.
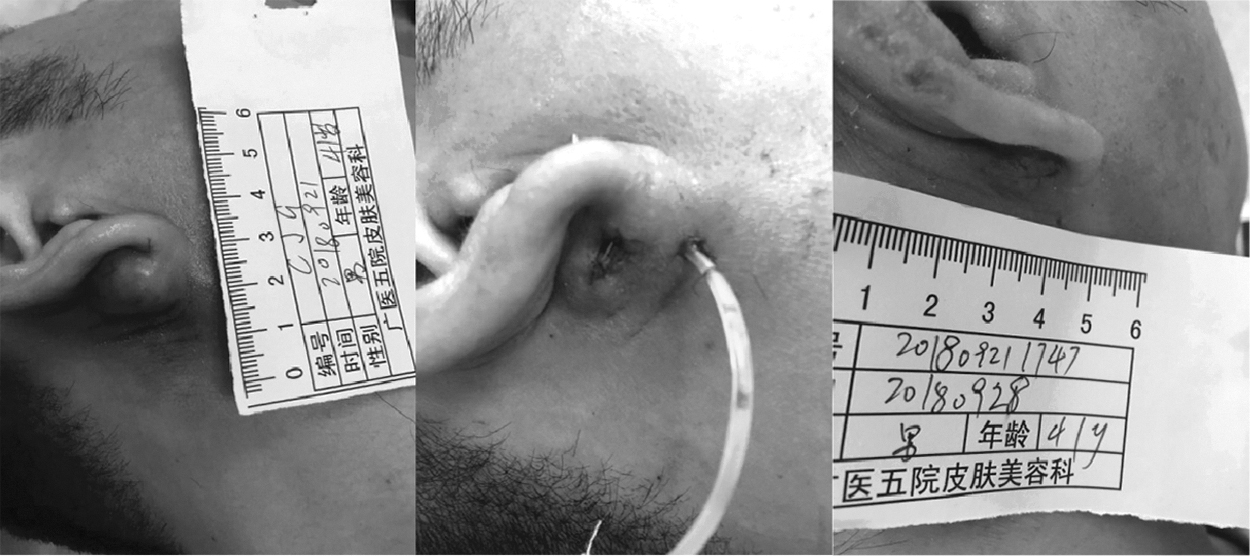
Posterior earlobe abscess. The patient had an abscess approximately 2.5 × 2.5 cm behind the earlobe before treatment. The swelling and fever were obvious. After topical negative pressure therapy/vacuum-associated closure (TPN/VAC) treatment, inflammation such as redness and swelling were completely eliminated within seven days and the scar was not obvious after recovery.
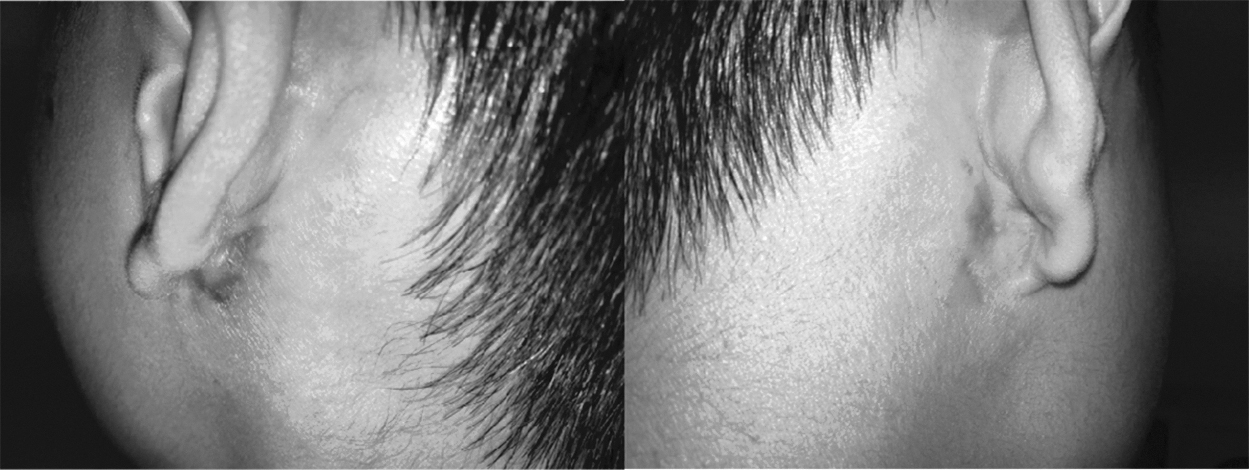
Healing scar of the observation group (left) and the control group (right).
Microbial Culture Results
Comparisons of Therapeutic Effects between Groups
Surgical site healing and recurrence
Both the observation group and the control group achieved primary healing. After one month of follow-up, there was no recurrence in the observation group and two recurrences in the control group. There was no significant difference between the two groups (p > 0.05).
The observation group achieved healing and suture removal seven to nine days after operation, and the scar was not obvious (3–8 mm). In the control group, three to five days after the first stage of abscess drainage, the second stage of wound suture was performed. The total healing time was 10–12 days, and the suture was removed; the scar was more obvious (15–25 mm). There was significant difference between the two groups (p < 0.05).
Dressing change
Both methods require daily dressing changes. The time of dressing change in the observation group was 14.9 ± 2.0 minutes (11–19 minutes) and that in the control group was 14.6 ± 2.6 minutes (10–20 minutes). There was no significant difference between the two groups (p > 0.05). The total number of dressing change was three to five times for each patient in the observation group and five to eight times for each patient in the observation group. There was statistical significance between the two groups (p < 0.05). The pain score of patients in observation group was 3.2 ± 0.6 (2–4 points) whereas that of patients in the control group was 5.1 ± 0.8 (4–7 points). There was significant difference between the two groups (p < 0.05). For the control group, the operation requires two times, the first-stage operation requires daily dressing change and drainage skin replacement after incision and drainage. The second-stage operation requires three steps: continuous dressing change after suture, suture removal once, duration of seven to 10 days, and may even require hospitalization, increasing the burden of medical staff and patients. The process of removing and inserting drainage strips after the first-stage operation is painful and irritating to the wound. The patient had pain and poor tolerance. The observation group only needed to report on the day of operation, the first day after operation, the second/third day after operation, and the seventh day after operation for a total of four to five days. In addition to the operation time, dressing change and suture removal only need 10–20 minutes per visit, which does not interfere much with work/life; the dressing change process minimally irritates the wound, has a low degree of pain, and patients tolerate it well.
Microbial culture results
All patients underwent microbial culture and drug sensitivity tests. The results are shown in Table 1. Staphylococcus aureus was cultured in 12 patients, Staphylococcus epidermidis in three patients, Staphylococcus dunnii in two patients, Proteus mirabilis in one patient, Enterobacter aerogenes in one patient, Candida growth in one patient's secretion, gram-positive anaerobic bacteria in one patient, gram-positive anaerobic bacteria in one patient, and gram-positive anaerobic bacteria in one patient. Gram-negative anaerobic cocci were cultured from the patients, including Acinetobacter baumannii in one case and methicillin-resistant Staphylococcus aureus (MRSA) in two cases. Drug sensitivity results were sensitive to a variety of antibiotic agents. The remaining culture results were negative.
Antibiotic use
The observation group was treated with antibiotic agents orally for three to five days (3.73 ± 0.87), whereas the control group was treated with unconstrained antibiotic agents intravenously for three days (generation 1 cephalosporin) and then orally for five to seven days (7.86 ± 1.15) according to the results of drug sensitivity. There was significant difference between the two groups in the number of days (p < 0.05).
Effects on the surrounding environment
In the observation group, the negative pressure suction device was replaced by dressing change, and the pus was confined to the vacuum suction device, which had less environmental pollution and reduced the risk of hospital infection and community infection. The control group changed dressing mainly by washing or scrubbing wounds. Flushing or scrubbing fluids may contain pathogenic bacteria, increase environmental pollution, and increase the risk of nosocomial and community infections.
Discussion
Sebaceous gland cysts are common, especially those with strong facial oil secretion. If an abscess is formed behind the earlobe, because the lesion is close to the mastoid process, the abscess will spread to the mastoid process and further lead to the accumulation of abscess in the brain tissue complicated by suppurative mastoiditis, which may be life threatening [3]. For the abscess in the head and face triangle area, it is easy to cause cavernous sinus thrombophlebitis caused by dissemination, and further develop meningitis or brain abscess, thus endangering life [4]. Therefore, in clinical practice, for such patients, active treatment is needed to avoid the formation of brain abscess caused by the spread of infection. The traditional treatment of an abscess is plastic skin graft drainage after incision and drainage or passive drainage. The drainage of an abscess is not thorough enough, and needs to replace the drainage skin every day [5]. It causes pain and fear to patients, and the tolerance and compliance are not high. Moreover, the medical staff change the dressings every day, which has a large workload and the risk of nosocomial infection. And after passive drainage is completed, second-stage surgery is needed to re-suture, and re-operation also causes more burden to patients and medical staff.
At present, the application of negative pressure suction in many kinds of refractory wounds has achieved satisfactory results [6,7]. The TPN/VAC method uses active suction to absorb the pus and necrotic tissue under negative pressure, avoid the spread of infection focus, and complete abscess incision, drainage, and debridement and suture in one operation, which greatly reduces the burden for both doctors and patients [8]. During the first two to three days of dressing changes, because the drainage fluid is located in the negative pressure vacuum syringe, less pollution to the environment and personnel results, reducing the possibility of nosocomial infection. Moreover, because local negative pressure can continuously attract and remove necrotic tissues, it can reduce the destruction of surrounding tissues during the operation. Only clear necrotic tissues can be removed, whereas other mild inflammatory infiltration tissues can be properly retained and TPN/VAC can continuously absorb and clean the necrotic tissues resulting in less damage to tissues and less formation of natural scars.
The use of antibiotic agents is under strict control in the current worldwide increasing bacterial resistance [9]. Although abscess belongs to the use of antibiotic agents, it will still increase the proportion of antibiotic agents used by physicians. It is necessary to minimize the use of antibiotic agents and achieve good therapeutic effect. Under TPN/VAC therapy, the dosage and level of antibiotic agents can be reduced, which has a positive effect on physicians, patients, and society at large. The incubation and drug sensitivity waiting period of common pathogenic bacteria causing abscess, such as Staphylococcus aureus and Staphylococcus epidermidis, is approximately 48 hours. During the incubation period, the infection focus in TPN/VAC will not aggravate or spread. After removing the negative pressure tube, sensitive antibiotic agents can be used to treat the abscess.
Footnotes
Funding Information
This study was supported by research funds from Guangzhou Health Science and Technology Project (20191A011093).
Author Disclosure Statement
No competing financial interests exist.