
Abstract
Background:
Removal of hardware with irrigation and debridement in patients with surgical site infections (SSIs) is performed commonly. However, the removal of hardware from patients with SSIs after spinal procedures is controversial. Moreover, primary spinal infections such as spondylodiscitis may require instrumentation along with surgical debridement. The purpose of this article was to evaluate critically and summarize the available evidence related to retention of hardware in patients with deep SSIs, and the use of instrumentation in surgical treatment of primary spinal infections.
Methods:
A literature search utilizing PubMed database was performed. Studies reporting the management of deep SSIs after instrumented spinal procedures, and of primary spinal infections using instrumentation published in peer-reviewed journals were included. Identified publications were evaluated for relevance, and data were extracted from the studies deemed relevant.
Results:
Because SSIs occur typically during the early post-operative period before stable bony fusion has been achieved, the removal of instrumentation may be associated with instability of the spinal column, pseudarthrosis, progressive deformity, pain, loss of function, and deterioration in the activities of daily living (ADL). Hence, early SSIs after spinal instrumentation are usually treated without removal of hardware. Moreover, primary spinal infections such as spondylodiscitis may require surgical debridement and instrumentation in cases with associated instability.
Conclusions:
Retaining or using instrumentation in patients with SSIs after spinal procedures or in patients with primary spinal infections, respectively, are commonly practiced in the field of spine surgery. Further evidence is required for the development of definitive algorithms to guide spine surgeons in decision making regarding the fate of instrumentation in the treatment of spinal infections.
Surgical site infections (SSIs) are associated with substantial morbidity, mortality, and cost. Approximately 80 million surgeries take place in the United States each year and approximately 1.5 million of these will be complicated by an SSI, a number that is believed to be greatly underestimated because of challenges in post-discharge case reporting [1]. Surgical site infections after spinal procedures are also a relatively common complication and have a devastating impact on outcomes [2]. The incidence of SSI is less than 3% with simple spinal procedures such as decompressive laminectomy or discectomy but the incidence increases to as high as 9% with the addition of instrumentation [3,4]. Instrumented surgical procedures increase the risk of SSIs for several reasons including the extended duration of operations performed using hardware, transmission of infectious agents through potentially contaminated implants, and the ability of microorganisms to use instrumentation as a reservoir [5]. As a result of the ability of microorganisms to use instruments as a reservoir and cause recurrent infections, removal of hardware is performed commonly in the context of deep SSIs associated with various instrumented surgical procedures across surgical specialties. However, this practice has changed in the case of deep SSIs after instrumented spinal procedures. Furthermore, instrumented stabilization in primary spinal infections has become a routinely performed procedure when indicated.
The current review had two purposes: first, to analyze critically available evidence to document the reasons for retaining or using instrumentation in patients with SSIs after spinal procedures or in patients with primary spinal infections, respectively. Second, to provide recommendations for management of the patients with deep SSIs after instrumented spinal procedures and of those with primary spinal infections who require surgical stabilization.
Bacterial Colonization of Hardware
Although implantable medical devices have revolutionized modern healthcare, complications associated with the insertion of hardware into living tissues are encountered frequently. A major concern after implant surgery is colonization of the implant surface or adjacent tissue with microorganisms that can ultimately necessitate implant removal or replacement [6,7]. Whereas decades of scientific studies have provided us with the most advanced means of preventing and fighting infections, microorganisms have also evolved to resist biocides and survive under the most unfavorable conditions. One of the key mechanisms that allows microorganisms to survive and cause infections is the ability to attach and form aggregates on implant surfaces. These communities of microorganisms are attached to implant surfaces by excreting a sticky, sugary substance that encompasses them in a matrix called biofilm.
Biofilms are well known to be resistant to both host defense and antibiotics and have been proposed as a critical contributor to chronic infections [7]. Evidence suggests that biofilms with less than ∼105 bacteria are capable of sustaining a chronic bacterial infection, although these infections may initially be asymptomatic for an extended time period [7,8]. Interestingly, biofilms can include living microorganisms other than bacteria such as fungi, algae, yeasts, and protozoa, creating a mixture of different microbial species. The three-dimensional extracellular polymeric slime (EPS) matrix structure of the biofilm makes penetration by host defense and antibiotic agents more difficult (Fig. 1). Bacteria in biofilms also have a low metabolic rate that is thought to be a major contributor to their resistance to antibiotic treatment [9].

Representational drawing of methicillin-resistant Staphylococcus aureus (MRSA) biofilm. (Source: Kateryna Kon/shutterstock.com. Used by permission.)
Classification of SSIs after Instrumented Spinal Surgeries
Surgical site infections typically result from contamination of the surgical site during the interval between the skin incision and incision closure when the instruments are introduced into the body [2]. Occasionally, SSIs can be acquired hematogenously any time after an instrumented surgery as a result of other infectious processes within the body such as urosepsis, skin infections, etc. [10]. Arbitrarily, instrument-associated spinal SSIs can be divided into two categories: early and late onset [10,11].
Early-onset infections are defined as those occurring within the first 30 days after the surgery. The usual pathogens are highly virulent microbes such as Staphylococcusaureus, streptococci, and enterobacteria (Escherichia coli, Proteus mirabilis, Klebisella spp. etc.) [10,11]. The signs and symptoms of early-onset infections are usually more typical in acute infections including fever, pain, erythema, swelling, warmth, and surgical site drainage.
Late-onset infections occur after the first 30 days after surgery and are caused by less virulent microorganisms such as coagulase-negative staphylococci, Propionibacterium acnes, and diphtheroids. The signs and symptoms can be more insidious and chronic in nature. Constitutional symptoms with local pain and tenderness may be the only indication of infection. Because of chronicity of the infection, complications such as vertebral osteomyelitis are more likely to occur in patients with late-onset instrument-associated spinal infections.
Factors Affecting the Decision to Retain or Remove Instrumentation
In most specialties, management of patients with deep SSIs after instrumentation requires irrigation and debridement, hardware removal, and long-term antibiotic agents because the implants can harbor bacteria by means of biofilm formation [12]. In contrast, the management paradigm has evolved over the last two decades within spinal surgery. The present recommendation is to preserve rather than remove the spinal instrumentation in the majority of spine cases [11]. The most important guiding factors in deciding to retain or remove spinal instrumentation are the status of bony fusion and the stability of the spine. The majority of SSIs become evident during the early post-operative period during which bony fusion is unlikely to be achieved. Therefore, removal of spinal instrumentation in early-onset spinal SSIs can cause grave complications such as instability, pseudarthrosis, and progressive deformity [11–13]. Surgical management of patients with early-onset SSIs after spinal instrumentation should include irrigation with debridement, retention of hardware and bone graft, intra-wound antibiotic powder if appropriate, and primary closure using nylon sutures over a drain when feasible (Fig. 2).
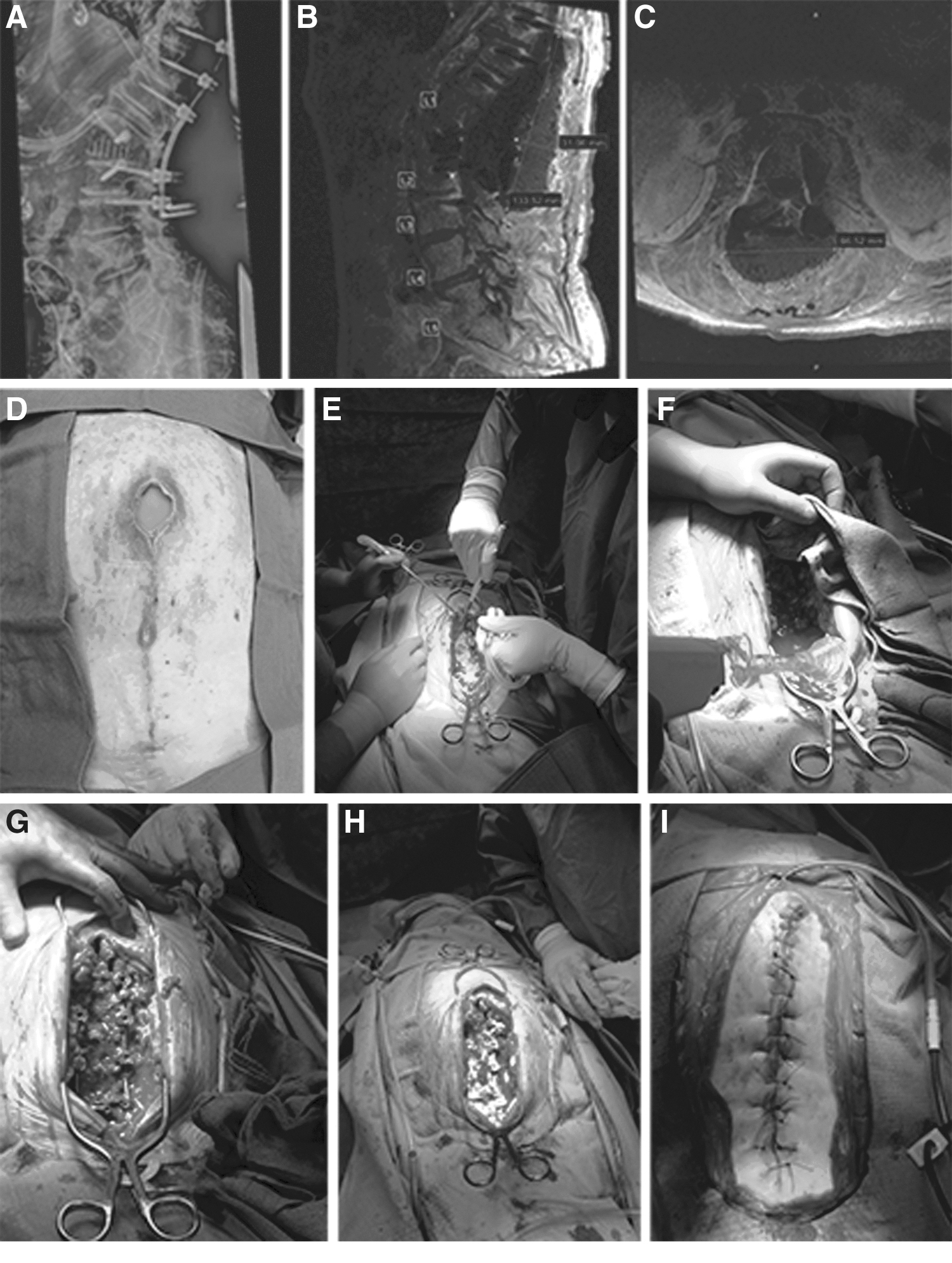
Images from a case of unstable L1–L2 fracture. Lateral radiograph demonstrates T10–L3 posterior spinal instrumentation and fusion (
In late-onset SSIs after spinal instrumentations, a bony fusion is often established, or there is at least a stiff fibrous union [11]. Hence, the risk of instability caused by removal of hardware is less than that of early-onset SSIs. Surgical treatment of patients with late-onset SSIs after spinal instrumentation can be performed with irrigation and debridement, removal or replacement of hardware, intra-wound antibiotic powder if appropriate, and primary closure using nylon sutures over a drain. It should be kept in mind that even when there appears to be radiographic evidence of bony fusion, removal of instrumentation can be associated loss of correction, and/or progressive deformity of the spine in the setting of an undetected pseudarthrosis [11,12].
In a retrospective case series including 737 patients who underwent posterior spinal instrumentation of the thoracolumbar spine, Sierra-Hoffman et al. [13] identified 26 cases of post-operative infections. Of those 26 patients, 19 had early-onset, and seven had late-onset infections. Seventeen (90%) of the patients with early-onset infections were cured with irrigation and debridement, and intravenous (IV) antibiotic agents without removing the hardware. One patient had to receive extended antibiotic therapy and replacement of instrumentation because of hardware failure. The other patient had to undergo removal of instrumentation after fusion was attained and received another course of antibiotic therapy. Six of seven patients with late-onset infection required removal of instrumentation. Five patients had stable fused spines and had their instrumentation removed without new hardware. One patient had exchange of instrumentation because of spinal instability and eventually was cured. The authors concluded that early-onset infections associated with spinal instrumentation can be treated successfully without instrumentation removal.
Abbey et al. [14] investigated 1,059 patients after lumbar fusion and instrumentation and identified 34 patients with SSIs post-operatively. Instrumentation removal was required in 12 (35.3%) patients. Early removal (<1 month) was performed in only one patient, who was left with a non-fused back. The authors suggested not to remove instrumentation before fusion has been achieved and to consider long-term suppressive oral antibiotic agents until bony fusion is attained (up to 9 months) after short-term IV antibiotic treatment.
In a systematic review, Lall et al. [12] reported that “no level I or II evidence was identified in the literature regarding surgical or medical management of post-operative deep infection after spinal instrumentation.” However, the authors could identify level III evidence supporting instrumentation retention in the setting of early-onset infections and removal of instrumentation for late-onset infections. They noted that “for deformity patients, even if solid fusion is observed, removal of instrumentation may be associated with significant loss of correction.” Therefore, surgeons should consider implant replacement in late onset SSIs after correction of spinal deformity.
Potaczek et al. [15] evaluated the impact of instrumentation removal on curve progression in patients with adolescent idiopathic scoliosis. The most frequent reason for implant removal was fistula formation (38.9%) with a mean of 2.7 years between the index procedure and removal of instrumentation. In this study, the patients with infections had the greatest loss of correction despite the removal of implants at a minimum of 11 months after the index procedure. Overall, loss of correction was lower in patients who had their hardware removed over two years after the index procedure compared with the patients who underwent removal of instrumentation less than two years after the index procedure.
In support of findings from the study by Potaczek et al. [15], Alpert et al. [16] reported on 75 patients who underwent removal of instrumentation after posterior spinal fusion (PSF). The mean age at the time of hardware removal was 15.9 years and the mean time from the index PSF to removal was 2.8 years. The patients who underwent removal of spinal instrumentation because of infection (28%) had more curve progression than those without infection (with a mean of 33.8 degrees vs. 18.8 degrees, respectively). Interestingly, curve progression was greater in patients who had all of the instrumentation removed than in those who had partial removal (average 23.1 degrees vs. 3.2 degrees). On the basis of these studies (Table 1) and authors' experience, it is highly advisable not to remove hardware before fusion has been achieved in patients with SSIs after instrumented spinal procedures.
Studies Supporting Retention of Hardware in Patients with Early-Onset SSIs after Instrumented Spinal Procedures
It must be noted that removal of hardware because of infections even at very late stages may cause worsening of scoliosis.
PSIF = posterior spinal instrumentation with fusion; SSIs = surgical site infections; AIS = adolescent idiopathic scoliosis; I&D = irrigation and debridement; IV = intravenous.
Instrumentation for Surgical Treatment of Primary Spinal Infections
Analysis of the epidemiologic data regarding primary spinal infections reveals a rapidly growing incidence over the last two decades paralleling the increase in the prevalence of intravenous drug abuse, and the increasing availability of novel immunosuppressive therapies [17,18].
Surgical treatment with instrumentation in patients with primary spinal infections such as vertebral osteomyelitis or osteodiscitis with abscess formation and deformity has been a controversial area because of the dogma that insertion of implants into an infected patient will make the eradication of infection more difficult once the implant has been seeded [19]. However, there is general consensus among spine surgeons as to when surgical treatment is indicated. The indications for escalating to irrigation and debridement with instrumentation can be summarized as spinal cord compression, neurologic compromise, gross bone loss with progressive deformity and spinal instability, and failure of medical management [20–24].
In a retrospective study with 118 patients who underwent surgical management for primary spinal infections, Bydon et al. [25] compared the outcomes of decompression only (36 patients) versus decompression with instrumented fusion (82 patients). There were seven re-operations (19.44%) in the decompression-only group and 14 re-operations (17.07%) in the decompression with instrumented fusion group (p = 0.756). Although the number of patients presented with osteomyelitis/discitis pre-operatively was greater in the instrumented group compared with the decompression-only group (79.27% vs. 36.11% respectively; p = 0.001), there was no difference between the two groups in terms of post-operative continued osteomyelitis/discitis (9.76% vs. 8.33% respectively; p = 0.807). These findings suggest that the addition of instrumentation in patients with primary spinal infections does not increase the incidence of recurrent infection while allowing for stabilization when spinal integrity is compromised.
In another retrospective cohort study, Dennis Hey et al. [26] compared the mortality, re-operation, and re-infection rates in patients with deep spine infection treated with antibiotic agents alone (n = 24), antibiotic agents with debridement (n = 33), and antibiotic agents with debridement and instrumentation (n = 27). There was no difference between the groups in terms of re-operation or relapse. However, the authors could demonstrate a reduction in crude hospital mortality for patients who underwent instrumentation compared with those who received antibiotics alone (odds ratio [OR] 0.82; p = 0.01).
In a population of immunocompromised patients with pyogenic vertebral osteomyelitis (PVO), Carragee and Iezza [27] demonstrated resolution of infection after debridement with instrumentation in 31 of 32 (96.9%) patients. The only case of recurrent infection occurred in a patient with an infected indwelling vascular catheter. At 10-year follow-up, all available patients had achieved resolution of their infection. The authors suggested that “the use of spinal instrumentation in immune-compromised patients with PVO is associated with a low risk of long-term recurrent infection.”
Finally, in a systematic review of 26 publications representing 931 patients with spondylodiscitis who underwent decompression, debridement, and instrumented fusion, de la Garza-Ramos et al. [28] found that the addition of instrumentation in primary spinal infection has a low local recurrent infection rate (1.6%). Their results revealed 6.3% overall post-operative infection rate (recurrent plus SSI), and 4.5% re-operation rate because of complications such as pseudarthrosis and instrumentation failure. Although overall post-operative infection and re-operation rates appear to be much higher compared with the rates seen after instrumentation procedures for non-infected degenerative spinal pathologies, it can be speculated that instrumentation in primary spinal infections help achieve spinal stability in more than 95% of the patients who might otherwise develop progressive spinal instability.
Although available evidence does not include any level 1 or 2 studies (Table 2), in primary spinal infections with severe spinal bone loss, deformity, instability, cord compression, and neurologic deficits, surgical treatment with irrigation and debridement, and instrumentation to stabilize the spinal column is justified.
Some of the Studies Reporting of Instrumentation in Patients with Primary Spinal Infections
I&D = irrigation and debridement.
Summary
The goal of instrumented fusion in spinal procedures is to achieve spinal stability, to mitigate pain, correct deformity, and to prevent neurologic deterioration. Contrary to common practice in other surgical specialties, retention of hardware in the context of deep SSIs after instrumented spinal procedures, or insertion of hardware in the context of primary spinal infections, are commonly performed in spine surgery. In patients with early-onset (<1 month) deep SSIs after instrumented spinal procedures, surgical management should include irrigation and debridement, application of vancomycin powder, retention of hardware and bone graft material, and primary closure using nylon sutures over a drain when feasible. In cases of late-onset (>1 month) SSIs associated with instrumented spinal procedures, it is advisable to consider removing hardware only if there is radiographic evidence of stable bony fusion. Otherwise, the authors suggest continuing with suppressive antibiotic treatment until such evidence is obtained (Fig. 3). In patients with primary spinal infections, there is sufficient evidence and justifiable common belief that instrumented stabilization should be performed with no hesitation when there are indications such as spinal instability, gross bone loss, progressive deformity, and intractable pain. However, indications for various surgical management strategies may differ, and every patient needs to be evaluated on a case by case basis.
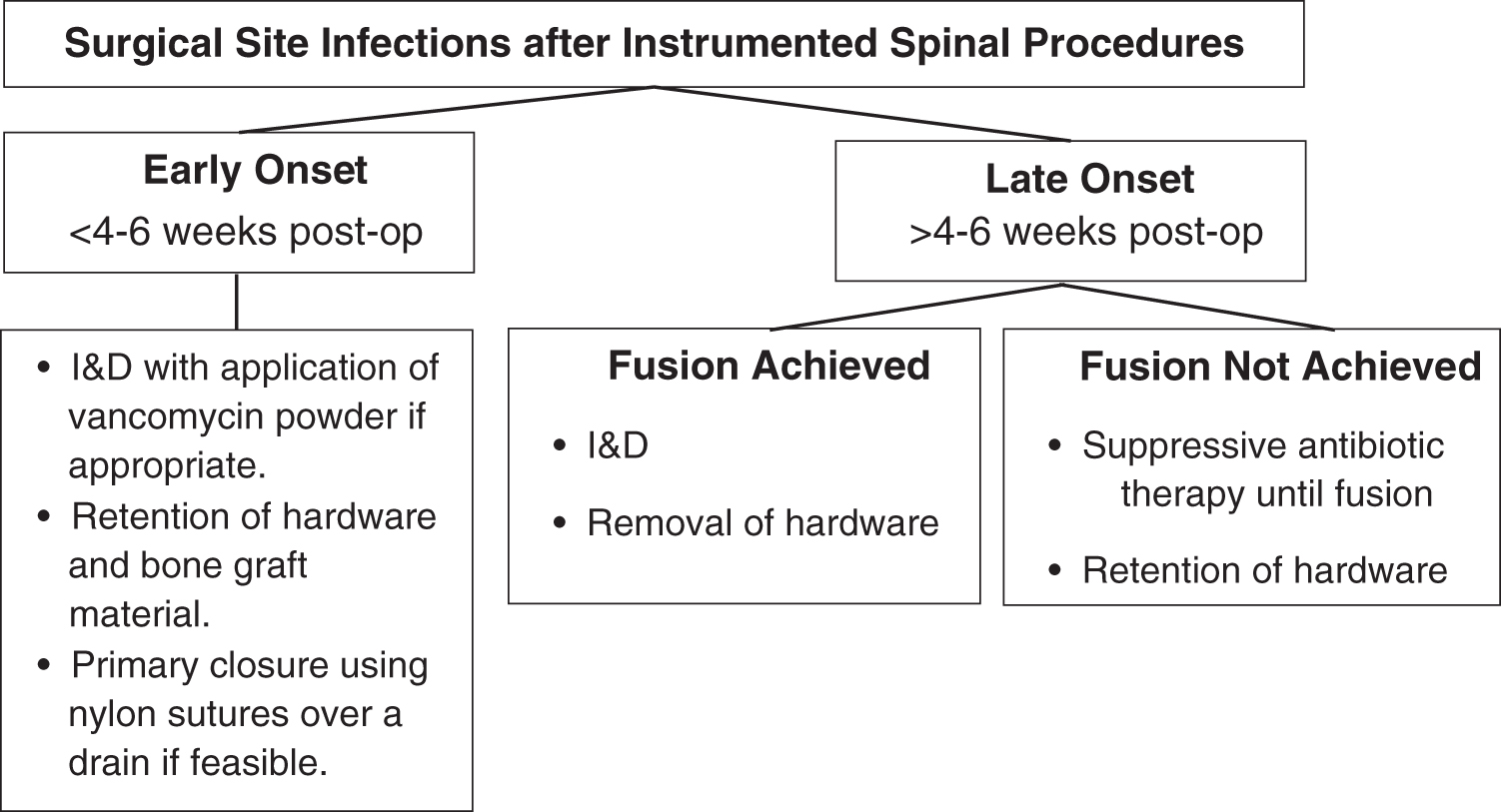
Schematic representation of authors' suggested strategy in cases with surgical site infections (SSIs) after instrumented spinal procedures. I&D = irrigation and debridement.
Footnotes
Funding Information
The authors state that no funding was received for this study.
Author Disclosure Statement
The authors declare that there is no conflict of interest regarding the publication of this article.