
Abstract
Background:
Electronic surveillance using clinical and administrative data from multiple sources has been reported as a tool for surveillance of surgical site infections (SSIs), but experiences are limited. In this study, we aimed to assess the accuracy of a text-searching algorithm to detect SSIs in children based on the application of regular expressions of unstructured clinical notes collected through different information systems.
Methods:
We developed an information system data warehouse that integrates data provided by electronic health and administrative records for patients who underwent surgical procedures in index weeks when active SSIs surveillances was conducted. To capture whether the patient developed an SSI, we developed a customized application to analyze clinical notes and code descriptions applying a pattern-matching algorithm based on regular expressions. We described the SSI cases detected by the active surveillance and the text-searching algorithm. To assess the accuracy in identifying the SSIs through the two methods, we adopted a reference standard that calculated the total number of SSIs as those detected by active surveillance plus those derived by the text-searching algorithm that was missed by active surveillance.
Results:
Compared with the total number of SSIs used as a reference standard, both methods had a specificity of 100%, a positive predictive value of 100%, and a negative predictive value >99.5%. Sensitivity was 70% for the text-mining algorithm and 60% for the active surveillance. Accuracy was >99% with both methods. The kappa value was 0.46.
Conclusions:
Compared with conventional surveillance of SSIs, a text-searching algorithm is a valid tool for case finding that has the potential to reduce drastically the workload of conventional surveillance, which involved direct contact with all families.
Surgical site infections (SSIs) are one of the most frequent healthcare-associated infections (HAI), accounting for around 20% of all HAIs [1]. These infections are associated with longer post-operative in-hospital stays, additional surgical procedures, and a higher mortality rate, representing a negative impact on patient outcomes and healthcare costs [2–4]. The incidence of SSIs differs according to age, type of surgery, use of implants, and surgical incision classification [5–7]. In children, SSI rates within 30 days after surgery range from 2.3% to 6% [6,7].
Surveillance of SSIs is a crucial component of strategies to reduce their incidence, as it enables evaluation of clinical outcomes, monitoring of hospital and surgical team performance, and evaluation of the impact of quality improvement programs on risk reduction. A number of methods have been developed for the surveillance of SSIs [8], including in-patient surveillance, post-discharge follow-up, and automated analysis of administrative or clinical data [9–12].
Active surveillance of SSIs and post-discharge follow-up of patients by infection control teams generally are considered accurate and reliable methods to estimate the incidence of SSIs but are time-consuming and expensive [13]. Identification of SSIs from administrative data, such as diagnosis and procedure codes, requires fewer resources but may be inaccurate, because this depends on the quality and completeness of the electronic administrative data [14]. Electronic surveillance using clinical and administrative data from multiple sources (i.e., surgical, laboratory, radiology, and medication records, physicians' and nursing notes, and diagnosis at discharge) has been reported as a tool for surveillance of SSIs, but experiences are limited [15–17]. The aim of the present study was to assess the accuracy of a text-searching algorithm to detect SSIs in children based on the application of regular expressions of unstructured clinical notes collected through different information systems.
Patients and Methods
We conducted this study at the Ospedale Pediatrico Bambino Gesù (OPBG), an academic tertiary-care children's hospital located in Rome, Italy, with 607 in-patient beds and approximately 24,000 annual admissions. The study was approved by the Hospital Ethics Committee; there was no intervention on the participants.
At the time the study was performed, the Hospital Infection Control Committee (ICC) conducted active surveillance for SSIs on children aged 0 to 17 years undergoing surgical procedures during one index week per quarter [9]. During the index weeks, the list of patients undergoing surgical procedures was obtained from the operating list orders. These children were followed up by trained nurses to identify SSIs up to 30 days from surgery; to collect information on SSIs, data were drawn from clinical records if patients were still hospitalized or through a telephone interview with parents if they had been discharged home. The SSIs were classified according to the case definitions of the Centers for Disease Control and Prevention, Atlanta, GA USA [18] (Table 1). Infections present at the time of surgery were excluded.
Surgical Site Infection (SSI) Case Definitions (Adapted from Reference 19)
For the current study, we developed an information system data warehouse that integrates data provided by electronic health and administrative records for patients who underwent surgical procedures in the SSI active surveillance index weeks from the first quarter of 2016 to the fourth quarter of 2018 (12 index weeks). The electronic sources of data included surgical intervention records, hospital discharge notes, emergency admission records, out-patient visits, and laboratory findings (Table 2). The data warehouse was developed in collaboration with the hospital information technology team and the data management office.
Source Databases of Information System Data Warehouse and Variables Extracted and Adopted within Text-Mining Algorithm
ICD = International Classification of Diseases.
As shown in Fig. 1, this set of records constituted the data sources layer of the information system architecture. To select the data collected in these systems and store them in the integrated database, an extract, transform, and load tool (ETL tool in Fig. 1) was implemented, adopting the IBM Cognos Business Intelligence suite. In particular, this tool accomplished this task through the following two steps: (1) it extracted the list of surgical interventions performed during the SSI active surveillance index weeks; and (2) it detected from the source systems all the events related to the patient that occurred within 30 days from the surgical intervention and loaded them into the integrated database.
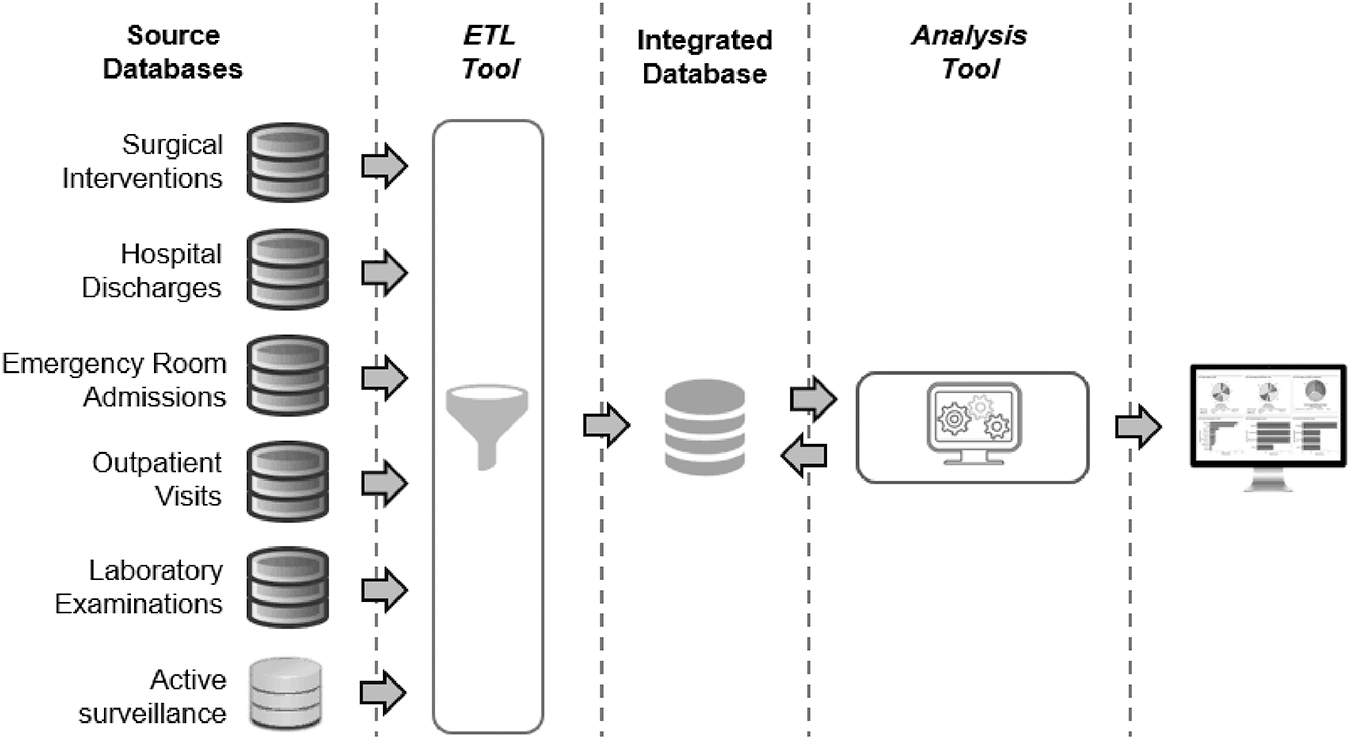
Description of information system high-level architecture underlining its components: Source databases where data were collected; the ETL tool that transforms these data and stores them in the integrated database (data warehouse); the customized application developed to analyze the integrated data, which provides an interface to the user with results of text-mining algorithm.
To capture whether the patient suffered an SSI, we developed a customized application (analysis tool in Fig. 1) to analyze clinical notes and code descriptions applying a pattern-matching algorithm based on regular expressions (Fig. 2). The application was implemented adopting the Qt framework (https://www.qt.io), a free and open-source widget toolkit that supports the creation of graphic user interface applications. It also provides an embedded regular expression engine that enabled us to implement the algorithm presented in this paper easily to capture an SSI within the explored narrative texts. In particular, the algorithm was based on a set of search items that suggest the presence of an infection within 30 days after surgery. The first group of terms aims to capture whether an infection had been detected during the child's examination (Group 1.1 in Fig. 2), whereas the second one verifies whether this infection involved the surgical site (Group 1.2 in Fig. 2). The adopted algorithm first verifies if, within the same sentence, there is a term of one group followed by a term of the other group. If a sentence matches this regular expression, the algorithm verifies if this positive result is a false positive that could be generated by the presence of a negative term (Group 2 in Fig. 2). An isolate from a site culture also was associated with a possible SSI. The terms were selected according to the literature (15–17) by the ICC team, which consists of the hospital Medical Director as chairman, infectious disease physicians, infection control nurses, physicians who are experts in infection control, microbiologists, pharmacists, chief surgeons, and physicians and nurses of clinical departments.

Description of algorithm based on standard expressions to analyze clinical notes and code descriptions. Group 1 includes list of terms to capture whether an infection had been detected during child's examination (Group 1.1) and if this infection involved the surgical site (Group 1.2). Group 2 includes list of terms to verify if results of Group 1 could be generated by presence of a negative term.
All possible SSI cases detected by the algorithm were investigated by an ICC physician expert in infection control, who reviewed the clinical records of the patients. Possible SSI cases were defined as confirmed if they met the criteria reported in Table 1.
In this paper, the feasibility of the information system and the text-mining algorithm have been tested considering the surgical procedures carried out during 12 SSI active surveillance index weeks from the first quarter of 2016 to the fourth quarter of 2018.
We described the SSI cases detected by the active surveillance and the text-searching algorithm. To assess the accuracy in identifying the SSIs through the two methods, we adopted a reference standard that calculated the total number of SSIs as those detected by active surveillance plus those derived by the text-searching algorithm that were missed by active surveillance. We then calculated sensitivity, specificity, the positive predictive value, the negative predictive value, accuracy, and the F score of the two surveillance methods. We also calculated Cohen's kappa coefficient to capture the level of agreement of the two methods.
Results
A total of 3,434 surgical procedures were performed during the study period and included in the analysis. Through active surveillance, 2,944 (85.7%) procedures were traced, whereas the remaining patients were lost to follow-up. Among patients who were followed actively, there were 18 SSIs, 15 (83.3%) of which appeared after discharge.
The text-searching algorithm explored the clinical notes of the 3,434 patients undergoing surgical procedures; of these, 1,100 (32.0%) had at least one hospital follow-up visit within 30 days after surgery, and 118 (3.5%) were still hospitalized at 30 days. The algorithm identified 48 possible SSIs, 9 (18.7%) of which were in the active surveillance group, and an additional 12 (25.0%) were confirmed after chart review. The total of the confirmed cases was 21 (43.7%), of which 47.6% occurred after hospital discharge.
The two methods together identified a total of 30 SSIs. Among the 12 SSI cases that were missed by active surveillance, 9 (75%) occurred in children who were lost to follow up, and 3 (25%) were in children whose families were interviewed by telephone and did not report signs or symptoms of SSI. All of the nine SSI cases that were missed by the text-searching algorithm involved children who were discharged home and did not return to the hospital for a follow-up visit within 30 days of surgery.
Table 3 describes the performance of active surveillance and the text-searching algorithm in detecting SSIs. Compared with the total number of SSIs used as a reference standard, both methods had a specificity of 100%, a positive predictive value of 100%, and a negative predictive value >99.5%. Sensitivity was 70% for the text-mining algorithm and 60% for the active surveillance. Accuracy was >99% with both methods. The kappa value was 0.46.
Surveillance Performance of Active Surveillance and Text-Mining Algorithm
CI = confidence interval.
Discussion
In this study, we compared a conventional surveillance of SSIs based on active follow-up of children within 30 days of surgery with electronic surveillance based on a text-searching algorithm. This electronic surveillance had a sensitivity of 70% and a positive predictive value of 100%, documenting its reliability. Conventional surveillance methods of SSI based on patient follow-up and manual chart review are particularly time consuming; for this reason, they may be limited to selected types of surgery or to subsamples of patients undergoing surgical procedures [7]. Electronic surveillance tools based on administrative and clinical data can improve the detection of SSI cases, and previous studies have reported sensitivities ranging from 60.0% to 97.8% [20]. Site culture results, hospital re-admissions, and out-patient visits were considered by other authors as data required for electronic surveillance of SSI [21]. When we conducted this study, we did not have in-place complete electronic medical records; therefore, the text-searching algorithm explored only the electronic components of the medical records that were in place, which included hospital discharge notes, emergency visits, hospital admissions, surgical summaries, out-patient visits, and incision culture results. Mining of these electronic sources of information identified possible SSIs that were confirmed if cases were reported by active surveillance, or, if not, were confirmed through patient chart review by a physician expert in infection surveillance and control. Overall, the text-mining algorithm identified as possible cases 1.4% of the 3,434 patients who underwent surgical procedures; therefore, only a small proportion of possible cases were verified by the infection control team. Compared with conventional surveillance of SSIs, this semi-automated surveillance clearly has the potential of drastically reducing the workload of conventional surveillance, which implied active contact with all families. As expected, most of the SSIs appeared after hospital discharge [9]. Cases missed by the text-searching algorithm were patients who did not return to the hospital within 30 days after surgery, confirming that the algorithm was valid in detecting possible SSI cases seen by the hospital staff. In our study, cases missed by the algorithm in patients who did not return to the hospital within 30 days after surgery were identified through active surveillance with telephone calls to families and the administration of a structured questionnaire on SSI onset. In settings where follow-up visits are not scheduled routinely after surgical procedures, or where the rate of attendance at these visits is sub-optimal, a combination of surveillance methods should be used to monitor SSI occurrence.
A further advantage of this method is the completeness of the patients included in the denominator. In fact, the active follow-up surveillance based on telephone interviews of parents failed to trace 14% of the families. Cases not detected by this conventional surveillance method included SSIs that occurred in children whose parents did not respond to telephone interviews or were not able to report SSIs signs or symptoms. Because of the complexity in defining SSIs and the need to have complete information on the occurrence of these HAI infections, semi-automated electronic surveillance can aid in case finding.
This study has some limitations to be considered. It represents the experience of a single institution, and it was not possible to compare our results with those of other hospitals. To reduce inter-observer variability, chart review of possible cases was performed by only one physician expert in infection control; however, the implementation of the tool as a routine surveillance method will involve a larger number of trained infection control practitioners. We limited our analysis to a follow-up period of 30 days after surgery, which is the surveillance time frame recommended for procedures without implants [2]. Further analysis should be conducted to investigate the reliability of electronic surveillance based on a text-searching algorithm over longer follow-up periods. Validation of the tool also should be conducted and could consist of checking of the actual data with an independent data source, such as an infection control practitioner or infectious diseases physician/microbiologist who has not been involved in the initial data collection and determination, who independently examines a random sample of cases to determine their classification and subsequently cross-check against existing data.
Surveillance of SSIs is important to target quality improvement interventions, monitor temporal trends, identify alert signals, and perform external benchmarking [5–7]. The main objective of this study was to assess the validity of an electronic tool for SSI surveillance to be adopted at the hospital level. In fact, previous studies have shown that the validity of automated or semi-automated surveillance of SSI must be investigated carefully, because cases may be misclassified by administrative or clinical data [14–16]. The results we obtained enabled us to implement the text-searching algorithm as a tool for case finding applied to all surgical procedures. The availability of timely and complete data on SSI incidence enables evaluation of the quality of surgical care in all pediatric specialties. Moreover, the analysis of narrative texts, which commonly are collected in different hospital information systems, has the advantage that the proposed method can be replicated easily in different settings. Text-searching algorithms may be developed for the surveillance of other quality measures, including HAI, such as central-line-associated blood stream infections. A further development of this algorithm will be to consider risk factor stratification of SSI rates regarding the “factors associated with SSI development, such as “category of operative procedure,” “duration of operative procedure,” and “incision class.” The collection of data on a larger number of cases may enable design and validation of predictive scores of SSIs in children. This is a promising field to enhance the collection of outcome indicators and their use to improve the quality of care of children undergoing surgery.
Footnotes
Funding Information
No financial support was received.
Author Disclosure Agreement
No competing financial interests exist.