
Abstract
The aim of this brief report is to raise awareness of necrotizing soft-tissue infections caused by Clostridium tetani in intravenous drug users, highlight the potentially unique dangers of this infection in this specific patient population, and outline the course of treatment currently considered the standard of care.
Tetanus is an acute, often fatal, disease caused by the exotoxin tetanospasmin, produced by the bacterium Clostridium tetani, and is characterized by muscle spasms and autonomic nervous system dysfunction. The symptoms include trismus, muscle tenderness, muscle clonus, abdominal rigidity, laryngospasm, diaphoresis, tachycardia, and hypertension. Since 1947, reported cases of tetanus in the United States have declined by >95% and deaths from tetanus by >99%, largely as a result of the use of tetanus antitoxin for wound management and the introduction of tetanus vaccines [1] (Fig. 1). However, intravenous drug abuse (IVDA) still carries a high risk of tetanus, particularly in heroin users who inject themselves subcutaneously [2]. This infection likely is attributable to the presence of Clostridium tetani spores, which can be a contaminant of quinine, a medication sometimes used to dilute heroin [3]. Intravenous drug abuse carries a wide range of other potential health risks and in particular of cutaneous, soft tissue, and systemic infections [4]. In pathogenic tetanus infections, patients are susceptible to systemic complications, high morbidity, including sepsis and multi-organ system failure, and death.

Annual rate* of tetanus deaths—National Notifiable Diseases Surveillance System, United States, 1947—2008.
Case Presentation
A 25-year-old female with a medical history of intravenous drug use and hepatitis C infection presented acutely to the emergency department with complaints of right lower-extremity pain, swelling, and an open wound. The patient reported she had had a chronic wound in this area for several months. Over the past week, she noted that the wound had increased in size and had become more painful, with a greater amount of drainage and a foul odor. She complained of decreasing ability to ambulate on the affected extremity because of pain and numbness of the right foot. The patient endorsed recent intravenous drug use and of injecting into the right leg. She denied any other symptoms. A consult request was placed to the surgical staff at our tertiary care center for comprehensive surgical and medical management.
On initial examination, the patient was toxic appearing and difficult to arouse but otherwise hemodynamically normal. Noted on the right lower extremity was significant tissue necrosis, waxy-appearing obvious exposed subcutaneous fat, and approximately 15 cm of anterior tibia bony exposure (Fig. 2A). There was significant pitting edema from the knee to the toes. On the posteromedial lower leg, there was a large blister that was flaccid and full of actively draining purulent fluid (Fig. 2B). The patient had palpable dorsalis pedis and posterior tibial pulses but diminished sensation in the dorsum of the right foot and decreased strength secondary to pain. The patient did not appear to be in extremis. Of note, her heart rate was 85 beats per minute, blood pressure 113/68 mmHg, temperature 36.2°C, breaths 15 per minute, and oxygen saturation 99% on room air. Laboratory studies revealed a white blood cell count of 39.7 × 103 cells/dL, hemoglobin 6.5 g/dL, sodium concentration 135 mEq/L, potassium concentration 5.4 mmol/L, serum creatinine concentration 1.6 mg/dL, and serum lactate concentration 5.5 mmol/L. The patient's calculated Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score was 6 points, placing her at intermediate suspicion for necrotizing soft-tissue infection (NSTI) [5].

Wound at presentation. (
The patient was started on vancomycin, clindamycin, and piperacillin/tazobactam. She was taken urgently to the operating room for a guillotine below-knee amputation. Over the subsequent 24 hours, the patient experienced clinical decline. She was unable to clear her lactate elevation despite aggressive fluid resuscitation, receiving >3 L of intravenous crystalloid, specifically 0.9% saline. She became hyponatremic to 129 mmol/L, and her white blood cell count rose to 41.2 × 103/mcL. She was dyspneic, and a chest radiograph revealed moderate-sized pleural effusions layering superiorly bilaterally (Fig. 3).
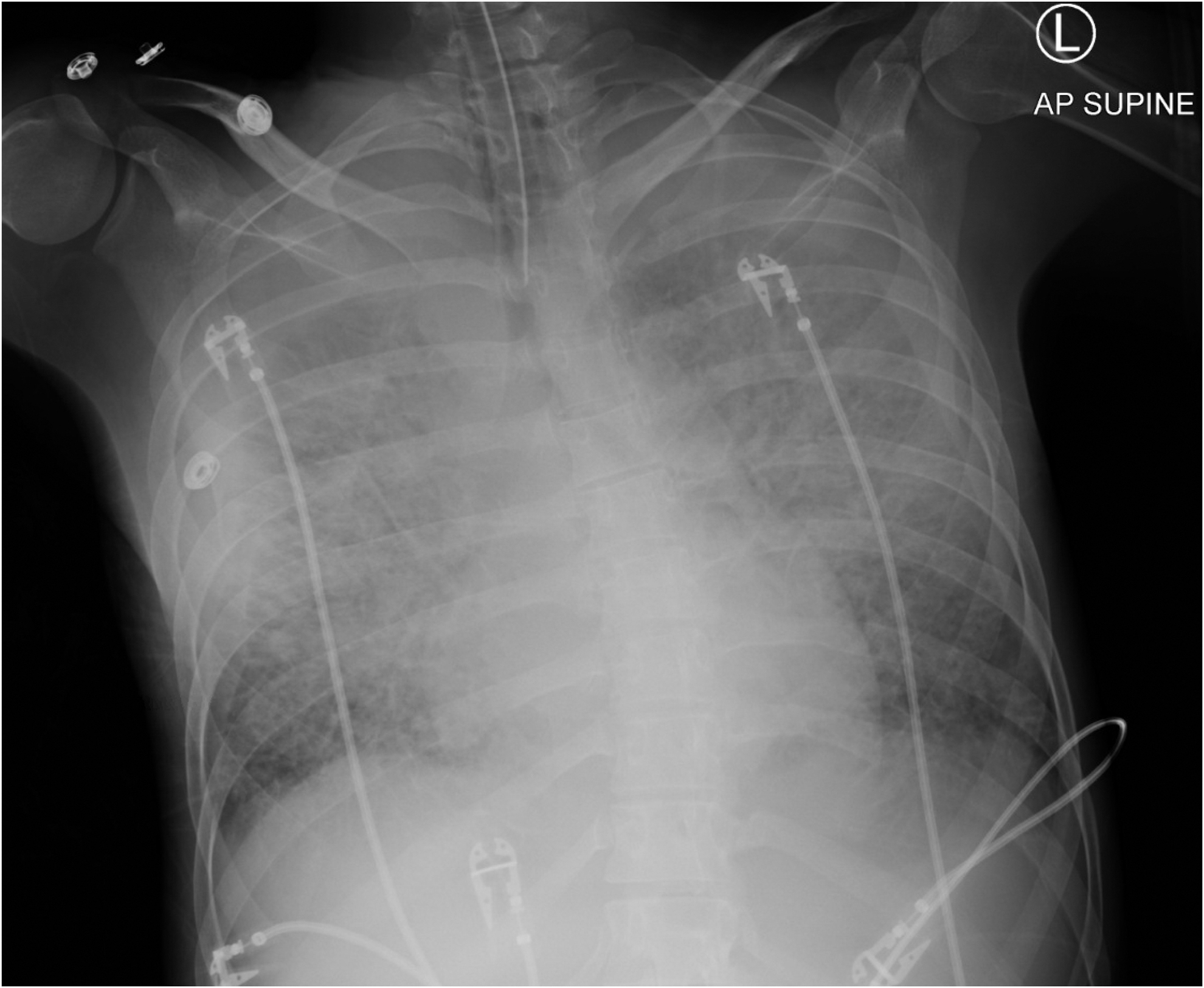
Portable chest radiograph.
With concern that there was spreading necrotizing soft-tissue infection as a source for her continued clinical decline, the decision was made to take the patient to the operating room on an emergency basis for re-evaluation under anesthesia. On this examination, there was mottling of the skin and minimal myonecrosis of the gastrocnemius muscle (Fig. 4). There was no gross pus noted. The skin of the posterior knee had some erythema and blistering. The decision was made to perform an above-knee amputation for definitive source control. The patient was hypoxic intra-operatively, likely secondary to significant volume overload; she remained intubated and was transferred to the intensive care unit. Unfortunately, shortly after arrival, she experienced cardiac arrest. Despite multiple rounds of cardiopulmonary resuscitation, the patient died. Four days after initial debridement, the tissue specimen sent to the microbiology laboratory for culture finalized, revealing abundant Clostridium tetani growth.

Below-knee amputation stump with myonecrosis.
Discussion
Necrotizing soft-tissue infection caused by tetanus can result in severe systemic complications, high morbidity, including sepsis and multi-organ system failure, and death [6]. This life-threatening disease is caused by a neurotoxin produced by Clostridium tetani, a spore-forming gram-positive bacillus widely distributed in soil and in the intestines of animals [1]. This toxin preferentially inhibits release of inhibitory γ-aminobutyric acid (GABA)-secreting neurons. Germination of C. tetani spores occurs under anaerobic conditions, such as in necrotic tissue that can result from puncture wounds typical of those found in the injecting drug user population. Most cases appear within eight days of exposure, but the incubation period can range from three to 21 days. Despite the dramatic reductions in the incidence of and death from tetanus, drug users who inject continue to be a specific high-risk population for pathogenic tetanus infections [7–9].
Prevention and treatment of infections secondary to tetanus includes active immunization, halting toxin production and uptake, management of muscle spasms, and supportive measures. The U.S. Centers for Disease Control and Prevention's Advisory Committee on Immunization Practices guidelines recommend that infants and young children receive a tetanus vaccine dose along with the diphtheria and pertussis (DTaP) vaccines, with one adolescent booster dose of tetanus toxoid, along with reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine. After receipt of Tdap, it is recommended that adolescents and adults receive a booster vaccine dose every 10 years [10]. Appropriate prophylaxis and antitoxin administration are imperative (Table 1). In the case of our patient, it was assumed that her immunizations were up to date, as she had recently undergone wound debridements at another institution. However, this information was not known at the time of emergency operative wound exploration. The issue is whether it would be of benefit to the patient of unknown immunization status to receive prophylactic tetanus immunization, given that she is at higher risk of morbidity and death.
Tetanus Prophylaxis and Antitoxin Administration.
Appropriate tetanus prophylaxis should be administered as soon as possible following a wound but should be given even to patients who present late for medical attention. This is because the incubation period is quite variable; most cases occur within 8 days, but the incubation period can be as short as 3 days or as long as 21 days. For patients who have been vaccinated against tetanus previously but who are not up to date, there is likely to be little benefit in administering human tetanus immune globulin more than 1 week or so after the injury. However, for patients thought to be completely unvaccinated, human tetanus immune globulin should be given up to 21 days following the injury; Td or Tdap should be given concurrently to such patients.
Tetanus toxoid may have been administered as DT, DTP/DTwP (no longer available in the United States), DTaP, Td, Tdap, or TT (no longer available in the United States).
Such as, but not limited to, wounds contaminated with dirt, feces, soil, or saliva; puncture wounds; avulsions; or wounds resulting from missiles, crushing, burns, or frostbite.
The preferred vaccine preparation depends upon the age and vaccination history of the patient:
• <7 years:DTaP.
• Underimmunized children ≥7 and <11 years who have not received Tdap previously: Tdap. Children who receive Tdap between age 7 and 11 years should receive another dose of Tdap at age 11 through 12 years.
• ≥11 years: A single dose of Tdap is preferred to Td for all individuals in this age group who have not previously received Tdap. Pregnant women should receive Tdap during each pregnancy.
250 units intramuscularly at a different site than tetanus toxoid; intravenous immune globulin should be administered if human tetanus immune globulin is not available. Persons with HIV infection or severe immunodeficiency who have contaminated wounds should also receive human tetanus immune globulin, regardless of their history of tetanus immunization.
The vaccine series should be continued through completion as necessary.
Booster doses given more frequently than every 5 years are not needed and can increase adverse effects.
DT = diphtheria-tetanus toxoids adsorbed; DTP/DTwP = diphtheria-tetanus whole-cell pertussis; DTaP = diphtheria-tetanus-acellular pertussis; Td = tetanus-diphtheria toxoids adsorbed; Tdap = booster tetanus toxoid-reduced diphtheria toxoid-acellular pertussis; TT = tetanus toxoid.
Wound management is an important element of tetanus infection control [11]. Injecting drug users may have foreign bodies within their wounds, and radiologic imaging can help guide their location and removal. Surgical debridement for source control, combined with empiric antibiotic therapy, is an important component of treatment of puncture wounds. Provided the patient is clinically stable, antibiotic therapy should be tailored to susceptibility testing of wound cultures [12]. Benzodiazepines are GABA type A receptor agonists and the first-line therapy for spasm control. The availability of mechanical ventilation is associated with improved outcomes for tetanus, as it allows spasms to be controlled by neuromuscular blocking agents or high doses of sedatives [3].
Conclusion
Tetanus is a potentially fatal condition caused by the exotoxin tetanospasmin, produced by the anaerobic bacillus Clostridium tetani. The infection is a major risk associated with injectable drug use. Prevention through stringent immunization prophylaxis can greatly reduce the risk of occurrence. In infected patients, early identification and subsequent treatment is paramount. Reluctance to admit drug using behavior because of the social stigma can be a hindrance to identifying at-risk patients. These patients often are lost to follow-up and do not complete their treatment course. In addition, prophylactic tetanus immunization should be considered for patients whose tetanus immunization status is unknown. Through proper education of both patients and those providers who care for them, tetanus infections related to injectable drug use can be mitigated.
Footnotes
Author Disclosure Statement
All authors report no conflicts of interest.