
Abstract
Background:
Acute native septic arthritis is a joint-threatening emergency. To date, however, no gold-standard treatment nor joint-specific treatment algorithms exist. We aimed to evaluate the etiologies, bacterial spectrum, treatments, and surgical outcomes of septic arthritis of the shoulder and knee.
Methods:
Seventy-one patients with septic arthritis of either the knee (n = 42) or the shoulder (n = 29) were followed over a mean period of 40 months (26–65). Data were collected according to the performed surgical procedure and pathway as well as the cause of infection, bacterial spectrum, and the Gächter classification. The prospective clinical examination included the Knee Society Score (KSS) or Constant Score (CS; shoulder group), pre- and post-operative pain, and return to previous activity.
Results:
Septic arthritis was caused primarily by post-interventional or post-traumatic conditions in the knee group and by hematogenous infection in the shoulder group. Staphylococcus aureus and S. epidermidis were most common, whereas Propionibacerium. were seen only in shoulder infections. Remission rates were 95% in the knee versus 90% in the shoulder group, whereas the mortality rate in the shoulder group was 10% (no one died in the knee group). While most knee infections could be managed with an arthroscopic approach, all shoulder infections necessitated an open approach. The mean KSS was 87.3 (49–100); the mean CS was 66.6 (37–95). Fifty percent of patients in the shoulder group versus 71% in the knee group reached their previous level of activity.
Conclusion:
The knee group exhibited post-interventional etiology, in line with high-virulence microbes and a high success rate with arthroscopic restoration. Septic shoulder arthritis showed hematogenous scattering, low-virulent microbes, and multiple interventions with a final open approach was always required. In contrast to the knee, in septic arthritis of the shoulder, a significant reduction in function has to be expected.
Native bacterial joint infections often have significant consequences for the patient and represent a therapeutic challenge. If left untreated or recognized too late, sepsis or multiple organ failure can lead to life-threatening clinical conditions. There are often delays in the treatment of patients with advanced infections, but early detection of a joint infection and rapid initiation of treatment are crucial for good treatment outcomes. Depending on the history, degree of expression, and anatomic accessibility, arthroscopic or open surgical procedures are used [1–3].
To date, there is no gold standard to manage these joint infections. The therapeutic principles are multi-modal. Depending on the response to immediate therapy, the joint can be rescued in the early stages. Otherwise, multi-step procedures and even joint resections with secondary replacement are necessary. In the most severe cases, procedures such as arthrodesis, amputations, or disarticulations are required.
Hematogenic infections are the most common entities [4], followed by post-interventional and post-traumatic causes—e.g., open fractures or severe tissue damage. Because of the increasing number of performed native joint interventions, the total number of post-interventional infections is increasing [5]. The incidence of large-joint infections depends on their localization as well as on previous clinical measures. Knee infections show different infection risk rates depending on the intervention factors: For joint puncture and arthroscopy the risk rate is 0.1% and for infiltration with corticoids or for ligament replacement surgical procedures, the risk rate is up to 1% [4]. Depending on the severity of an injury, the risk can be significantly increased.
Less common are injuries that directly penetrate the joint including deep lacerations, bruises, bites, and inflammations such as bursitis, subsidence abscesses, infected hematomas, phlegmons, erysipelas, necrosis, and hemarthrosis. In contrast, it is reported that the severity of shoulder infection is much more threatening than knee infections [6]. Incidence of infection after shoulder arthroscopy is 0.7%, whereas hematogenous infections occur more often [6].
Thus far, data on the different aspects of the genesis as well as the germ spectrum and severity of joint empyema on the shoulder versus the knee joint are largely lacking, although it is essential for effective treatment. It is generally understood that the cause, treatment, and outcome of shoulder infections are different from those of knee infections [7,8]. Most of the present literature and guidelines are published according to peri-prosthetic joint infections (PJIs), but this cannot be transferred to native joint infections.
Our primary objective was to determine the success rate, defined as a remission of the joint infection, of treatment and to identify the most appropriate surgical procedure (arthrotomy vs. arthroscopy). The secondary objectives were to identify the different bacterial spectra, etiology, and functional outcome.
Methods
Characteristics
Between January 2013 and September 2016, 71 patients with a primary shoulder or knee infection were treated in a single center specializing in musculoskeletal infections. Patients were divided into either the knee (n = 42; male: 30; female: 12) or the shoulder group (n = 29; male: 19; female: 10). Patients with recurrent infections, osteomyelitis adjacent to the joint, or peri-prosthetic infections and rheumatoid arthritis were excluded. Patients were followed over a minimum of 24 months (Table 1). The mean follow-up duration was 41 months (range, 26–65; SD: 10).
Patient Characteristics and Outcome Measures
Data were collected retrospectively according to the performed surgical procedure and pathway as well as the cause of infection, bacterial spectrum, and the Gächter classification [9] as a surrogate for infection grade. A prospective clinical examination included the Knee Society and Function Score in cases of knee infection and the Constant Score for shoulder infections. The pre- and post-operative pain scores were assessed and the percentages of the return to previous activity.
The study was approved by the Institutional Review Board (IRB) and conducted in agreement with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments and comparable ethical standards.
Diagnostics
Effective antibiotic therapy necessitates reliable bacterial detection; we therefore pre-operatively performed a sterile joint puncture (sent as blood culture) and obtained three to five tissue samples and a joint puncture intra-operatively. Cultures were investigated over 14 days to detect low-grade species. In addition, blood and synovial diagnostic tests were performed along with radiographic scans and also magnetic resonance imaging or computed tomography on an as-needed basis. Presence of infection was detected as described previously [4.10] and as summarized in Table 2. The Gächter classification was used to detect the severity of infection [9].
Diagnostic Algorithm
MRT = magnetic resonance therapy; PMN = polymorphonuclear neutrophil.
Surgical procedure
All surgical procedures were performed by one of four experienced surgeons in a beach chair-position (shoulder) or supine position (knee) under general anesthesia with no pre-operative single-shot antimicrobial prophylaxis. Systemic antimicrobial agents were administered after obtaining the tissue samples. Patients were treated by arthroscopy or arthrotomy according to the individual orthopedic surgeon's decisions in the first stage; the further intervention type and success were followed up and compared.
In cases of septic arthritis of the shoulder, a standard deltopectoral approach was used to enter the shoulder joint or an arthroscopic procedure using two to three portals was performed. In cases of septic arthritis of the knee, a standard arthroscopic approach was used or an open operation was performed using a standard anteromedial parapatellar approach. Joint lavage with at least 20 L of saline was performed routinely.
Synovectomy was performed in patients with marked synovial hypertrophy and intra-synovial abscesses [11]. In both the open and arthroscopic approach, irrigation and debridement were performed carefully. A synovectomy was performed from stage III and IV, using the Gächter classification. Inserted implants or grafts were checked for stability. Fixation materials for the grafts such as sutures, tight ropes, buttons, or screws were defined as implants, whereas peri-prosthetic infections were excluded from the study. In the case of early infections, the principle of implant or graft retention attempt only applies to the initial stages (up to Gächter stage II). In cases of instability, re-infection, or multi-stage procedure, the graft/implant was removed. In every case, a drain was left in the joint after operation.
Calculated systemic antibiotic therapy was initiated after intra-operatively collecting of microbiological samples during the first intervention. The calculated systemic therapy was performed using a broad-range antibiotic agent that provided good penetration of the soft tissue—in most cases, sulbactam–ampicillin. The antibiotic agents were adjusted three days after the procedure in accordance with the results of sensitivity testing.
Antibiotic agents were selected according to the principles of antibiotic stewardship, taking into account sensitivity and tolerability. Six weeks of systemic antibiotic therapy was administered: An initial intravenous therapy of two weeks followed by four weeks of pathogen-specific highly bioavailable oral antimicrobial treatment [12,13]. No anti-infective solutions, spacers, or local antibiotics were used. Clinical and laboratory monitoring for efficacy and toxicity were performed. Monitoring of outpatient antimicrobial therapy followed published guidelines [14].
After 6 weeks of high-efficiency antimicrobial therapy, the antibiotic agents were stopped. If there was evidence of ongoing infection, a repeat radical debridement procedure was performed including tissue sample testing, followed by further antimicrobial therapy. In this case, implants or grafts were removed in every case. Post-operatively, all patients were seen by a physiotherapist and were allowed to bear weight as they were able to use crutches in cases of knee infection. Range of motion was not limited.
Patient monitoring
Monitoring of the patients was performed according to published guidelines [14.15]. Evaluation of the patient included a physical examination and examination of wound healing, current clinical symptoms, drug allergies and intolerances, comorbid conditions, prior and current microbiology results from aspirations and surgical procedures, and antimicrobial therapy. A test for C-reactive protein as well as complete blood cell count and electrophoresis was performed pre-operatively and in further patient monitoring. A plain radiograph was obtained from all patients before and after operation. Blood cultures for aerobic and anaerobic organisms as well as procalcitonin were obtained in cases of pyrexia in patients.
Success rate, outcome measures, and statistics
Clinical outcome was assessed after a minimum follow-up of 24 months. “Success” and “Remission” of PJIs were defined as the absence of clinical, radiologic, and biologic (i.e., inflammatory markers) signs of infection [15] after follow-up of individual patients. Validated scores according to pain, function, and range of motion were used. Constant shoulder Score [16] and Knee Society Score (including Function Score) [17] were used in the current version.
For statistical analysis, an initial check for normal distribution of the values was performed using the D'Agostino–Pearson test. The Wilcoxon signed-rank test and Student t test were used to evaluate differences between the two groups for non-parametric and parametric data, respectively; results are presented as the mean and range (minimum and maximum values). The chi-square test was used for multi-variable analyses, and p ≤ 0.05 was considered statistically significant. All tests were two-sided.
The SPSS v22.0 was used for all statistical analyses (SPSS Inc., Chicago, IL). Sample size planning: 69 patients (case number planning was based on Pearson and Spearman correlations with an assumed correlation factor of 0.3 and a significance level of 5% with a power of 0.8).
Results
Patient characteristics
The mean age of patients in the shoulder group was 73 (range, 38–93) years, while that of patients in the knee group was 53 (range, 21–90) years.
Regarding the cause for infection, the knee group showed post-interventional and post-traumatic conditions, whereas in the shoulder group, hematogenous infection was the most common cause, being more than three times that in the knee group (Fig. 1).
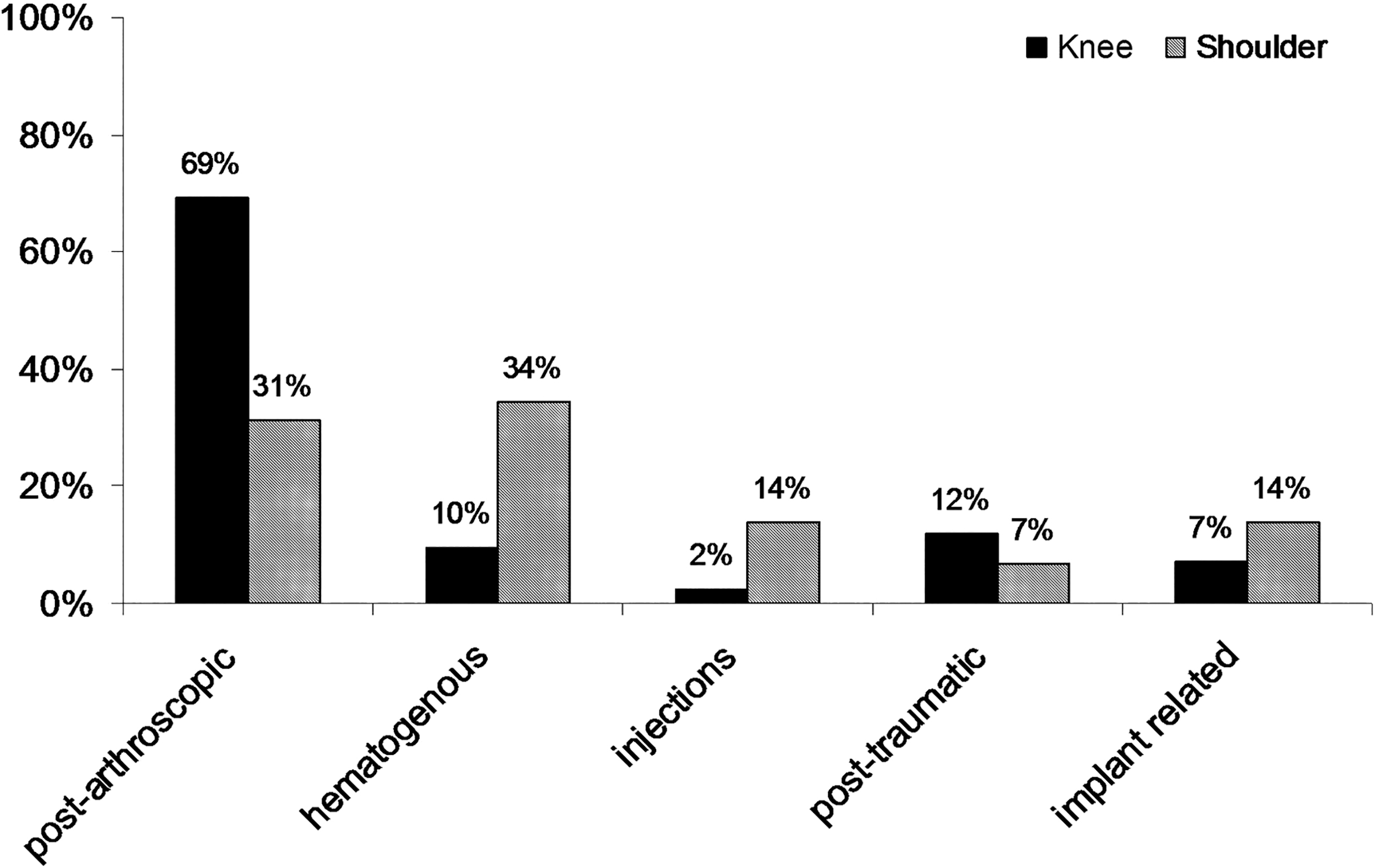
Etiology of septic arthritis of the shoulder and knee. Peri-prosthetic infections were excluded, whereas “implant-related” infections occur in implants fixating grafts and tissues.
Consequently, a different microbiologic spectrum was seen (Fig. 2). Staphylococcus aureus and S. epidermidis are the most common microbes in shoulder and knee infections. These highly virulent germs underline the post-interventional aspect of joint infections. Low-grade bacteria, however, were seen only in shoulder infections, indicating the hematologic etiologies in cases of the shoulder. Propionibacterium colonization is more often encountered around the shoulder than the knee. It is known that P. acnes heavily colonizes axillary skin. The severity of infection was assessed by using Gächter classification. There was no significant difference between the knee and shoulder groups (Table 1).
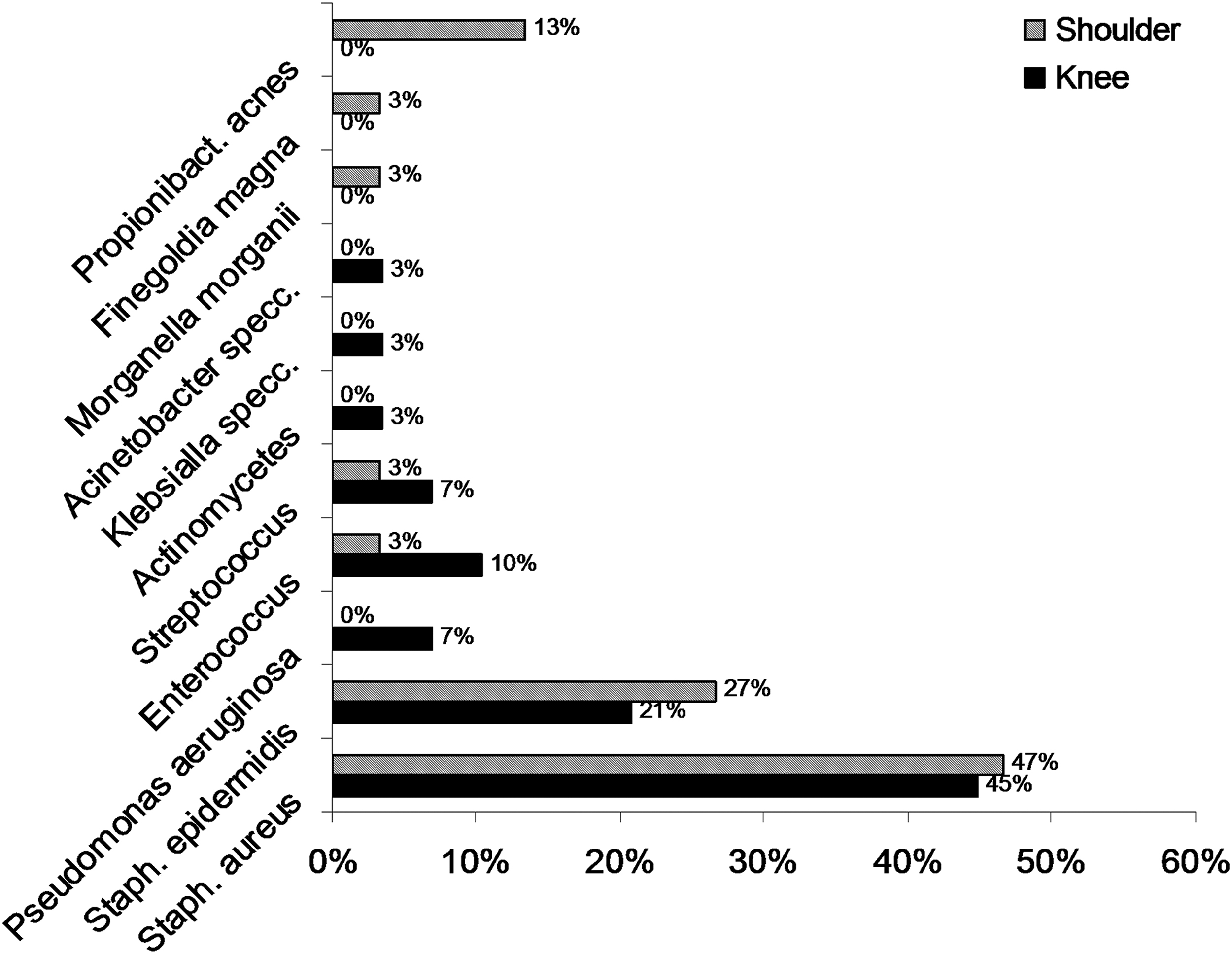
The different bacterial spectra of septic arthritis of the knee and shoulder. Staphylococcus aureus and S. epidermidis are the most common microbes, and these highly virulent microbes underlie the post-interventional etiology. Low-grade bacteria, such as Propionibacterium acnes, however, are seen only in shoulder infections, indicating the hematologic etiology.
The pathway of treatment and sequence of surgeries was analysed in both
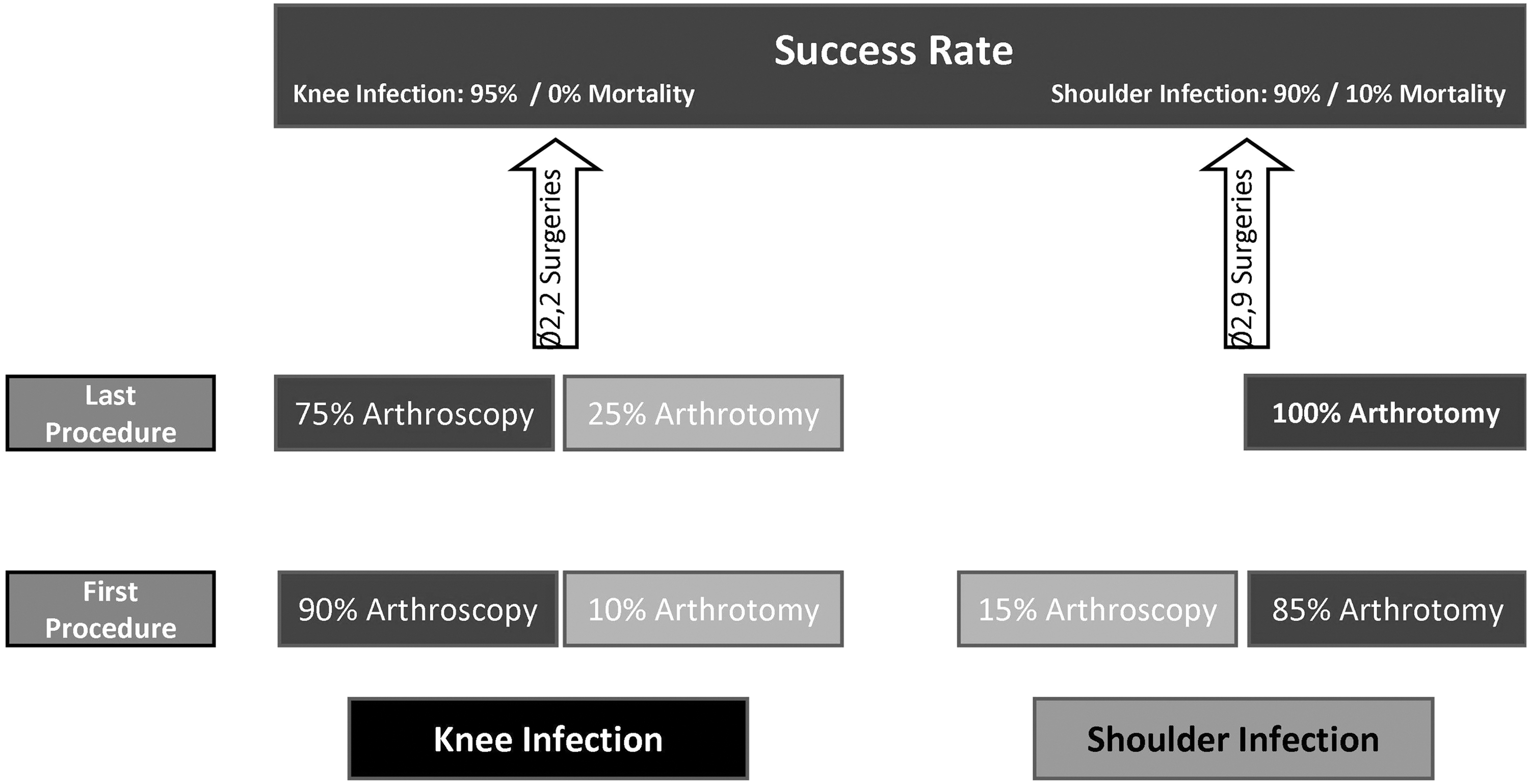
Retrospective analysis of the surgical management. All patients in the shoulder infection group had to be treated finally using an open approach. Most of the knee infections could be managed arthroscopically within all interventions; 15% had to be switched to arthrotomy. In 30% of the knee infections, a single-step procedure was sufficient, but in shoulder infections, this was possible in only 17% of cases.
The mean number of interventions in the knee and shoulder groups was 2.2 and 2.9, respectively. While 30% of knee infections involved a single-stage procedure, in shoulder infections, this was possible in only 17% of cases, and for the remaining 83%, two to six procedures were required (Table 1). We monitored the success rate according to the surgical approach. At the beginning of the treatment, there was an effort to manage the infection using an arthroscopic approach in 90% of knee and 15% of shoulder infections; however, it was only possible to finalize treatment by using an arthroscopic approach in 75% of those in the knee group, while all patients in the shoulder group finally had to be treated with an open approach to manage the infection (Fig. 2).
Patients were examined after a minimum follow-up of 24 months. The mean Knee Society Score and Function Score were 87.3 (49–100) and 85.2 (35–100), respectively. The mean Constant Score in the shoulder group was 66.6 (37–95) (Table 1). In contrast to only 50% patients in the shoulder group, 71% in the knee group were able to reach the previous level of activity. In the shoulder group, 46% of patients experienced a serious disability in using their arm and required help in their daily life.
The post-operative state was associated with a significant reduction in pain level compared with the pre-operative state (knee group: 2/10 and shoulder group: 3/10 versus knee group: 7/10 and shoulder group: 6/10, respectively) on the visual analogue scale. One-third of both groups showed pain even without weight bearing all the time of follow-up and one-third only during physical activity. There was a significant reduction in the pain level in both groups, however, when comparing pre-operative and post-operative levels (Table 1).
Discussion
We aimed to evaluate the etiologies, management, and outcomes of the two most frequent native joint infections—knee and shoulder infection. To our best knowledge, there is yet no comparable study in the literature. The study contains data of 71 patients: 42 native knee infections and 29 shoulder infections. Shoulder patients on average were significantly older, which appears consistent with the different infection etiology (hematologic vs. post-traumatic).
In both groups, the most common pathogens were high-virulence S. aureus and S. epidermidis. These bacteria are the most frequent, because of the mostly post-interventional or post-injection etiology of the infection [11,18]. Overall, more men than women were found, one explanation being the post-traumatic etiology. Active patients with joint and sports injuries are reported to be predominantly male.
Unfortunately, in this study Propionibacterium and other low-virulence microbes were present only in shoulder infections. One previous study reported that Propionibacterium colonization is more often encountered around the shoulder than the knee [19]. The P. acnes heavily colonizes axillary skin. The cells of P. acnes are more resistant to various commonly used antimicrobial agents than planktonic cells and can form biofilms in vitro [20]. Further, more than 30% of patients with shoulder infection showed a hematogenous etiology compared with the knee group, which typically showed post-interventional etiology of arthroscopic and injection interventions. Some studies recognized different aspects of etiologies and bacterial spectrum, but with no subsequent targeting regarding individualized therapy [21].
Septic arthritis of the knee and particularly of the shoulder is relatively rare compared with PJIs, and the literature surrounding the optimal treatment and outcomes after native joint infections is lacking. To date, only a few studies have compared different surgical procedures [7,18,21,22].
Age seems to play an important role, because we noted that patients with shoulder infections had a higher mean age than those with knee infections (73 vs. 53 years, respectively), which is consistent with different etiology. Gächter stages were in agreement with current literature, presenting about 70%–80% of both groups with a Gächter stage of 1 or 2 [7,8].
In 30% of knee infections, a single-step procedure was sufficient, but in shoulder infections, this was possible in only 17% of cases. Further, it was possible to manage 75% of knee infections arthroscopically, and only 15% of patients required therapy switching from arthroscopic to an open procedure. In contrast, all cases of shoulder infection had to finally switch to arthrotomy.
On average, shoulder patients had to undergo an average of 2.9 operations as against 2.2 operations in the knee group. For this reason, we postulate different treatment pathways for both types of infection. In the first procedure, an arthroscopic approach in the knee joints is mandatory, but according to our data, a direct open approach could be advantageous in shoulder infections. This is consistent with the findings of Böhler et al. [8] who reported that open arthrotomy is the more effective treatment method in septic arthritis of the shoulder, with lower reinfection rates and a comparable functional outcome; whereas, in knee infections, an arthroscopy is a less invasive method and should be considered the routine treatment, according to their data [7].
Generally, the reinfection rate appears to be slightly higher in the shoulder than in the knee, where primary salvage rates between 82% and 90% have been reported [7,8,23]. Jiang et al. [6] reported higher incidences of peri-operative septicemia, higher in-hospital complications, and longer average length of stay in the arthroscopic surgical group of shoulder infections.
As per our report, the success rate of treatment in both groups was more than 90%, which, according to current literature, is within the range of average results for the knee group and above the average results for the shoulder group [6–8,18]. In the shoulder group, all patients who had treatment failure died at the end as a result of septicemia and multi-organ failure. This 10% mortality rate underlines the aggression of shoulder infection; by contrast, no patient died in the knee infection group. In line with our data, death after septic arthritis of the shoulder was reported to be >10% [24] and was reported in a comparable collective with about a 17% mortality rate [1].
There are only a few studies that also prospectively investigated patients with septic arthritis by taking into account the functional outcome. Mean Knee Society Score and Function Score were 87.3 and 85.2, respectively, in our study, and 71% percent were able to return to previous activity and even sports. In contrast to our data that show relatively good functional outcome in patients with knee infection, other studies mention that functional outcome in most of the presented cases was only fair and report an average of 2.6 necessary interventions per patient [2,25].
Most of the studies only refer to patients after the anterior cruciate ligament repair. In these cases, return to sports was 68%, but more severe symptoms and reduced functional outcomes were seen [26]. The mean Constant Score in the shoulder group was 66.6 (range, 37–95), which is in line with the findings of Attmanspacher et al. [27] who reported a Constant score of 61 points in their patients.
One-third of all patients in both groups experienced pain even without weight bearing at the time of follow-up, while one-third experienced pain only during physical activity. There was a significant reduction in the pain level in both groups, however, when comparing pre-operative and post-operative levels.
Overall, these results indicate a more limited function after shoulder versus knee infection in affected patients. This can also be seen in the ability to return to previous activities and sports. In contrast to only 50% of patients with shoulder infection, 71% of those with knee infection could return to previous activities. In sum, 46% patients in the shoulder group had a serious disability in use of their arm and required help in their regular life, and 10% therefore had to quit their job.
Conclusion
The literature surrounding the optimal management and outcomes after native joint infections is lacking. We report consistent data of native knee and shoulder infections of 71 patients with a prospective functional follow-up. The knee infection group showed post-interventional etiology in line with highly virulent bacteria and a high success rate with arthroscopic restoration; however, multiple interventions along with good functional outcome can be seen often.
Patients with septic arthritis of the shoulder showed hematogenous scattering and low-virulent germs. Propionibacterium were only present in shoulder infections, which is associated with a difficult resistance specter and biofilm formation. In contrast to the knee group, in shoulder infection, remission could almost exclusively be reached by arthrotomy, and only a restrictive functional outcome with a higher mortality rate can be achieved.
We therefore postulate that treatment algorithms should be clearly adapted to shoulder or knee joint, because etiology, bacteria, and surgical and functional outcomes are different. Septic arthritis of the knee joint, however, can be managed using an arthroscopic approach, and the shoulder should be managed using an arthrotomy.
Limitations
This study has several limitations, mainly because of the retrospective design of the study. Investigation of the surgical procedure was conducted in a retrospective manner and was not randomized. A randomized trial in a multi-center setting would be valuable to reach significantly higher numbers of patients. Further, there could have been e bias regarding the management of those infections in a specialized clinic for joint and musculoskeletal infections; possibly the severity of the infections was higher than usual, because patients are often referred to specialized clinics only for very serious infections.
Footnotes
Author Disclosure Statement
No competing financial interests exist.