
Abstract
Background:
We sought to assess the efficacy of prophylactic abdominal drainage to prevent complications after appendectomy for perforated appendicitis.
Methods:
In this post hoc analysis of a prospective multi-center study of appendicitis in adults (≥ 18 years), we included patients with perforated appendicitis diagnosed intra-operatively. The 634 subjects were divided into groups on the basis of receipt of prophylactic drains. The demographics and outcomes analyzed were surgical site infection (SSI), intra-abdominal abscess (IAA), Clavien-Dindo complications, secondary interventions, and hospital length of stay (LOS). Multivariable logistic regression for the cumulative 30-day incidence of IAA was performed controlling for age, Charlson Comorbidity Index (CCI), antibiotic duration, presence of drains, and Operative American Association for the Surgery of Trauma (AAST) Grade.
Results:
In comparing the Drain (n = 159) versus No-Drain (n = 475) groups, there was no difference in the frequency of male gender (61% versus 55%; p = 0.168), weight (87.9 ± 27.9 versus 83.8 ± 23.4 kg; p = 0.071), Alvarado score (7 [6–8] versus 7 [6–8]; p = 0.591), white blood cell (WBC) count (14.8 ± 4.8 versus 14.9 ± 4.5; p = 0.867), or CCI (1 [0–3] versus 1 [0–2]; p = 0.113). The Drain group was significantly older (51 ± 16 versus 48 ± 17 years; p = 0.017). Drain use increased as AAST EGS Appendicitis Operative Severity Grade increased: Grade 3 (62/311; 20%), Grade 4 (46/168; 27%), and Grade 5 (51/155; 33%); p = 0.007. For index hospitalization, the Drain group had a higher complication rate (43% versus 28%; p = 0.001) and longer LOS (4 [3–7] versus 3 [1–5] days; p < 0.001). We could not detect a difference between the groups in the incidence of SSI, IAA, or secondary interventions. There was no difference in 30-day emergency department visits, re-admissions, or secondary interventions. Multi-variable logistic regression showed that only AAST Grade (odds ratio 2.7; 95% confidence interval7 1.5–4.7; p = 0.001) was predictive of the cumulative 30-day incidence of IAA.
Conclusions:
Prophylactic drainage after appendectomy for perforated appendicitis in adults is not associated with fewer intra-abdominal abscesses but is associated with longer hospital LOS. Increasing AAST EGS Appendicitis Operative Grade is a strong predictor of intra-abdominal abscess.
Acute appendicitis usually is divided into two types, uncomplicated and complicated. Complicated appendicitis, defined as perforated or gangrenous, is associated with a higher rate of post-operative infection complications, such as surgical site infection (SSI) and intra-abdominal abscess (IAA) [1,2]. Peritoneal irrigation and drainage traditionally are used to treat grossly contaminated complicated intra-abdominal infections, but studies have not shown any advantages of intra-operative irrigation for prevention of IAA [3,4].
Previous studies in children with perforated appendicitis have reported a significantly lower incidence of IAA in the group treated without drainage, and abdominal drainage may be associated with negative outcomes [5,6]. In adults, a recent meta-analysis by Cheng et al. included six trials involving 521 patients with complicated appendicitis who underwent emergency open appendectomy and found no significant differences between the drainage and no-drainage groups. However, the quality of the evidence was admittedly poor and was based on open appendectomy, an operation now rarely performed in the United States [7]. Large-scale database studies have reported that the laparoscopic approach is associated with two-fold higher odds of an IAA [8], and it is unknown whether peritoneal drainage would have greater benefit in this operation.
This study sought to assess the effectiveness of prophylactic abdominal drainage in preventing complications after laparoscopic appendectomy for perforated appendicitis. We hypothesized that prophylactic abdominal drainage is not associated with a lower incidence of post-operative complications, specifically IAA, during the first 30 days after discharge from the index hospitalization.
Patients and Methods
After approval from our local Institutional Review Board, we performed a post hoc secondary analysis of the Eastern Association for the Surgery of Trauma (EAST) multi-center appendicitis study (“MUSTANG”), a prospective observational study that enrolled adults (age ≥18 years) presenting to the emergency department (ED) with suspected or confirmed appendicitis between January 2017 and June 2018. Our secondary analysis included only subjects with perforated appendicitis as diagnosed intra-operatively by the surgeon. Exclusions were pregnancy, a final pathology diagnosis other than appendicitis (e.g., adenocarcinoma), and records with missing data. The exposure of interest was receipt of prophylactic operative drainage after appendectomy, which was placed according to surgeon preference. The primary outcome was the 30-day incidence of IAA. The secondary outcomes were SSI, Clavien-Dindo complications, secondary interventions (percutaneous drainage or operation), ED visits within 30 days, 30-day hospital re-admission, and index hospitalization length of stay (LOS).
Descriptive statistics were calculated. Continuous variables are reported as mean ± standard deviation or median [interquartile range], depending on the parametric or non-parametric distribution, and analyzed using either the Student t-test or Mann-Whitney test, as appropriate. Categorical variables are reported as counts and percentages and analyzed using the χ2 test or Fisher exact test. A p value <0.05 was considered statistically significant.
The demographic features of subjects with and without loss to follow-up were compared. Multivariable logistic regression analysis was performed for intra-abdominal abscess up to 30 days after discharge controlling for age, Charlson Comorbidity Index (CCI), duration of post-operative antibiotics, prophylactic drain utilization, and AAST EGS Appendicitis Operative Grade. Finally, we attempted to compare drain and no-drain patients using a propensity score-matching analysis, examining the following clinically relevant variables: Age, sex, weight, WBC count, Alvarado score, CCI, and AAST Operative Grade. Propensity score matching was performed using the MatchIt package version 3.0.2 in R version 4.0.0. Good coverage of propensity was found in both groups, suggesting that matches were sufficient to proceed with this analysis. Then a follow-up regression was run to determine the association of the intervention on the matched data. All statistical tests were carried out using StataCorp. 2015; Stata Statistical Software: Release 14 (StataCorp LP, College Station, TX).
Results
Overall, 3,262 patients underwent appendectomy; after exclusions, the final cohort comprised 634 patients, with 159 (25%) in the Drain group and 475 (75%) in the No-Drain group (Fig. 1). The baseline demographics are presented in Table 1. There were no significant differences in the frequency of male gender (61% versus 55%; p = 0.168), weight (87.9 ± 27.9 versus 83.8 ± 23.4 kg; p = 0.071), Alvarado score (7 [6–8] versus 7 [6–8]; p = 0.591), WBC count (14.9 ± 4.8 versus 15.0 ± 4.5 103/mcL; p = 0.867), or CCI (1 [0–3] versus 1 [0–2]; p = 0.113). The Drain group patients were significantly older (52 [39–62] versus 48 [33–61] years; p = 0.017) and had a greater proportion of higher AAST EGS Appendicitis Operative Grade perforated appendicitis. A comparison of the demographic features of the subjects lost and not lost to follow-up is presented in Table 2.
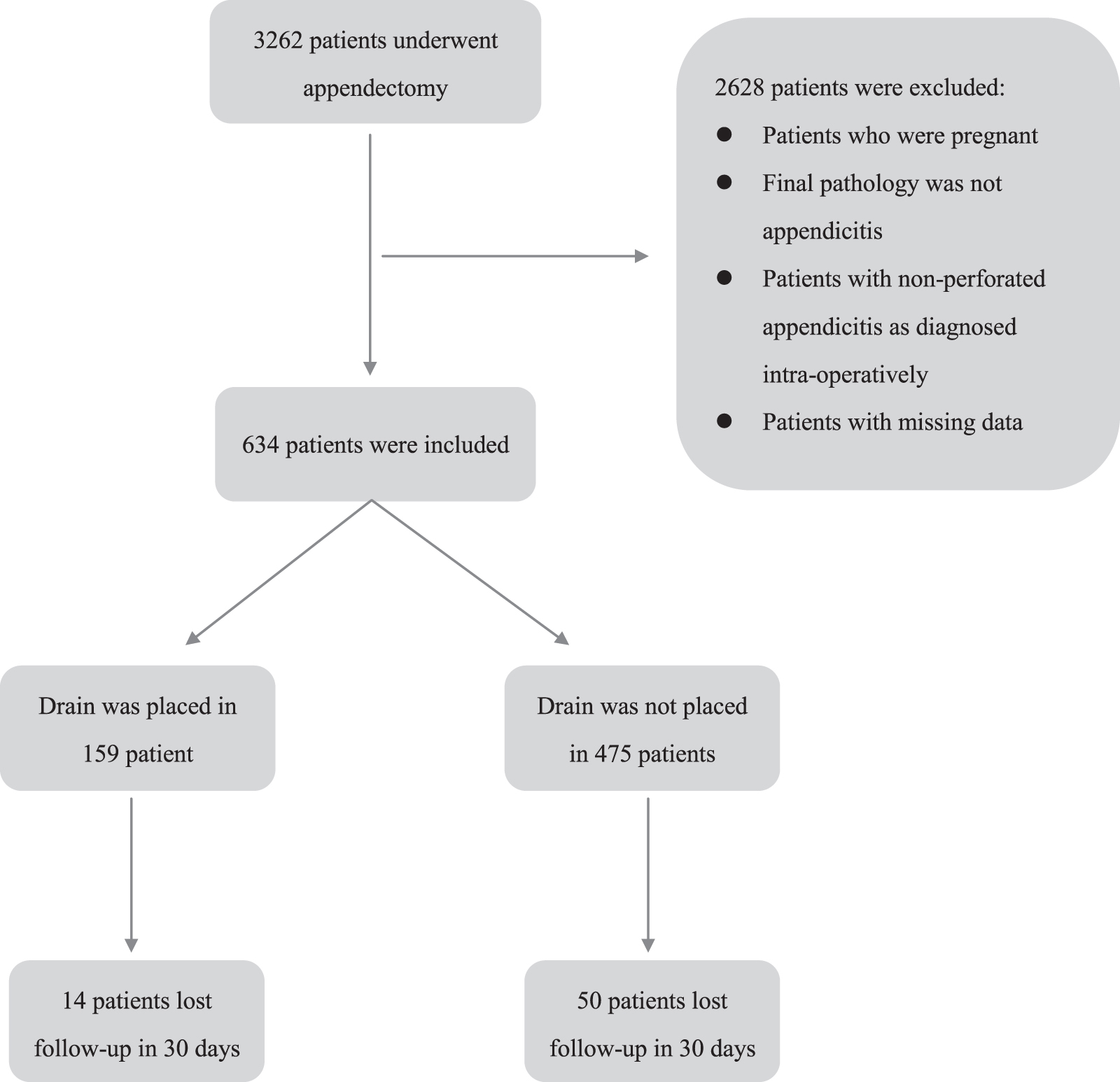
Flow chart of patient selection.
Demographics
Statistically significant p values are printed in
Percentages represent column percentages.
AAST = American Association for the Surgery of Trauma; CCI = Charlson Comorbidity Index; WBC = white blood cell.
Comparison of Demographics between Patients Lost and Not Lost to Follow Up
Statistically significant p values are printed in
Percentages represent column percentages.
AAST = American Association for the Surgery of Trauma; CCI = Charlson Comorbidity Index; WBC = white blood cell.
The index hospitalization and 30-day outcomes for all subjects and those separated by AAST Operative Severity Grade are summarized in Table 3. Drainage use increased as AAST EGS Appendicitis Operative Severity Grade increased: Grade 3 (62/311; 20%), Grade 4 (46/168; 27%), and Grade 5 (51/155; 33%); p = 0.007. For all subjects, the Drain group had a higher rate of Clavien-Dindo complications (43% versus 28%; p = 0.001) and longer hospital LOS (4 [3–7] versus 3 [1–5] days; p < 0.001) during the index hospitalization. There was no difference between the groups in the incidence of SSI (1% versus 2%; p = 1.0), IAA (7% versus 8%; p = 0.863), or secondary interventions (6% versus 6%; p = 1.0) during index hospitalization.
Index Hospitalization and 30-Day Outcomes
Statistically significant p values are printed in
ED = Emergency department; IAA = intra-abdominal abscess; LOS = length of stay; SSI = surgical site infection.
For 30-day outcomes, there was no difference in ED visits (15% versus 10%; p = 0.876), hospital re-admissions (10% versus 8%; p = 0.393), secondary interventions (6% versus 6%; p = 0.625), cumulative IAA (14% versus 13%; p = 0.889), or cumulative SSI (3% versus 5%; p = 0.504). The propensity score-matching analysis resulted in 144 pairs, and the comparisons of index hospitalization and 30-day outcomes are displayed in Table 4. On this matched comparison, the difference between groups in hospital LOS remained significantly higher in the Drain group (4 [3–6] versus 3 [2–5]; p < 0.001), but the difference in Clavien-Dindo complications was no longer significant (42% versus 33%; p = 0.1447). When separated by AAST Operative Severity Grade, the proportion of patients with an ED visit within 30 days was significantly higher in the No-Drain group only for Grade 3 (18% versus 4%; p = 0.01654). Multivariable logistic regression analysis demonstrated that only AAST Grade (odds ratio 2.7; 95% confidence interval 1.5–4.7; p = 0.001) was predictive of cumulative 30-day incidence of IAA (Table 5).
Propensity Score-Matched Analysis: Index Hospitalization and 30-Day Outcomes
Statistically significant p values are printed in
ED = ermergency department; IAA = intra-abdominal infection; LOS = length of stay; SSI = surgical infection.
Multivariable Logistic Regression Results: 30-Day Intra-Abdominal Abscess a
Statistically significant p values are printed in
AAST = American Association for the Surgery of Trauma; CI = confidence interval; OR = odds ratio.
Discussion
In this post-hoc analysis of 634 patients with perforated appendicitis, 159 patients (25%) received prophylactic abdominal drainage after appendectomy. We could not detect any difference between the groups in the incidence of SSI, IAA, or secondary interventions up to 30 days after index hospitalization discharge. Indeed, the Drain group had a higher rate of Clavien-Dindo complications and longer hospital LOS in the overall unmatched analysis and a longer hospital LOS in the propensity score-matched analysis.
Our results suggest that prophylactic drainage after appendectomy for perforated appendicitis in adults does not confer clinical advantages, and our study supports the current European Association for Endoscopic Surgery (EAES), World Society of Emergency Surgery (WSES), and Agency for Healthcare Research and Quality (AHRQ) recommendations that surgical drains should not be used routinely after appendectomy for complicated appendicitis [9–11]. One possible explanation for the lack of benefit of drainage is that once the source of infection has been removed and the peritoneum has been cleansed, it may be best to allow the endogenous peritoneal defense mechanisms to complete the eradication of bacteria without being disturbed by a foreign body (i.e., a peritoneal drain) [12].
Our results are concordant with those of previous studies. In a retrospective study, Schlottmann et al. [13] compared the effectiveness of abdominal drainage for complicated acute appendicitis between 2005 and 2015. In 225 patients undergoing laparoscopic appendectomy, 56 patients received abdominal drainage. Those investigators reported no difference in the overall morbidity or the rate of post-operative IAA. However, the use of abdominal drainage was associated with a prolonged hospital stay, as in our study. The earlier study was limited by its retrospective nature and small sample of subjects with abdominal drains. Our study analyzed data collected prospectively from 28 medical centers across the United States, representing a broad range of geographic regions and practice settings and had a larger sample. A case-control–matched study conducted in Switzerland [14] included 260 patients with complicated appendicitis seen from 2003 to 2007, with 130 patients receiving abdominal drainage. The investigators reported that patients without drains had a significantly lower rate of complications and notable benefits in terms of recovery time and LOS. That study also was limited by its retrospective design. Additionally, those investigators examined only surgical complications as primary outcomes. Our study included several other clinically important patient-centered outcomes during both index hospitalization and the period up to 30 days after discharge.
Other authors have reported contradictory findings. In a retrospective study, Pakula et al. [15] found that the placement of pelvic drains after laparoscopic appendectomy in patients with perforated or gangrenous appendicitis was associated with a significantly lower rate of pelvic abscess (6% versus 20%) despite a higher incidence of abscess on pre-operative computed tomography scans in the drain group. In a cohort including both open and laparoscopic appendectomies for perforated appendicitis, Beek et al. [16] described peritoneal drainage as being associated with a significantly lower re-intervention rate (11% versus 26%), and a significantly lower rate of complications (19% versus 33%).
However, it is important to note several caveats when interpreting the study by Beek et al. A significant proportion of their cases (nearly 50%) were open appendectomies or laparoscopic conversions to open operations. Thus, their conclusions may not be applicable to surgeons and centers with lower rates of open appendectomy. In a recent survey of American surgeons, only a minority (2%) reported open appendectomy as the preferred initial approach to perforated appendicitis [17]. Also, as discussed in the original “MUSTANG” study, the authors found that 98% of appendectomies were performed by laparoscopy [18].
Second, their definition of “re-interventions” included prolonged use of intravenous antibiotics (> 3–5 days), which occurred in nearly 10% of the no-drain group. Hospital re-admission also was included in the definition of “re-intervention” and was significantly more common in the no-drain group. It is debatable whether these two complications should be considered re-interventions, and it is unclear whether the re-intervention rate would still be significantly different in the groups after removal of these two categories.
Finally, the “overall complications” definition included post-operative abdominal pain (“abdominal complaints after surgery requiring prolonged clinical observation or additional biochemistry or radiological tests”), which occurred in 15% of the no-drain group and none of the drain patients. Indeed, this was the only sub-category of complications that was significantly more common in the no-drain group. This vague definition and questionable “complication” are difficult to assess in a retrospective chart review study and are subject to both selection and investigator bias.
Limitations
Our study has some limitations that must be acknowledged. First, because of the nature of post hoc analysis, the decision to place a drain was left to the individual surgeon's judgment. Because subjects were not randomized to the Drain/No Drain groups, there is a possibility of selection bias. For example, patients with more extensive peritoneal contamination may have been assigned to receive a drain, whereas those with minimal contamination received no drain. We attempted to control for such selection bias by performing propensity score-matched analysis and also by analyzing subjects according to the validated AAST EGS Appendicitis Operative Grade schema [19]. Drainage use rose as AAST EGS Appendicitis Operative Severity Grade increased; however, there is no difference in the incidence of intra-abdominal abscess in each AAST grade. This implies that although drains were placed more commonly in patients with more extensive peritoneal contamination, there was no significant difference in outcome. However, it still is possible that there were subtle differences between groups that were not detected using that framework.
Second, there were some patients lost to follow-up, and it is possible that this loss was non-random. Although there was no difference between the groups regarding the proportion of patients lost to follow-up, it is plausible that infectious complications were more common in one or the other group of those subjects lost to follow-up. As demonstrated in Table 2, the patients lost to follow-up had lower Alvarado scores and lower AAST Severity Grade; this may reflect the bias that patients with more severe disease are more likely to follow up.
In spite of these limitations, our study suggests that routine drain placement after appendectomy for perforated appendicitis is not beneficial and indeed is associated with a prolonged LOS. This topic is ripe for future research, as there are no definitive high-quality “landmark” trials, and community equipoise is evident.
In a 2008 survey, 22% of the responders would leave a drain after an appendectomy for perforated appendicits [12]. It is interesting that in the MUSTANG observational study [18], 25% of patients with perforated appendicitis received a drain, indicating that clinical practice is similar to survey responses from more than a decade ago. We believe our multi-center contemporary study is a meaningful contribution to the body of literature supporting current guidelines and may better inform clinical practice. Additionally, by reporting event rates, our study can help future investigators calculate appropriate sample sizes for randomized trials. For example, assuming a cumulative 30-day incidence of IAA of 14% in the Drain group (Table 3), a non-inferiority trial would require a total sample of 358 subjects (179 per group) to exclude a difference in favor of the standard group by more than 10%, with a power of 80% at an alpha significance of 0.05.
Conclusions
Prophylactic drainage after appendectomy for perforated appendicitis in adults is not associated with fewer infectious complications but is associated with a longer LOS. The AAST Operative Severity Grade is a strong predictor of intra-abdominal infections as late as 30 days post-discharge. Randomized trials are required to establish superiority, non-inferiority, or equivalence of outcomes with drain omission in perforated appendicitis.
Footnotes
Acknowledgments
We are grateful to the following colleagues for their contribution to data collection in the original EAST Appendicitis Study. Without their work, this manuscript would not have been possible (alphabetically by center):
Baystate Medical Center: Doctors Reginald Alouidor and Kailyn Kwong Hing
Beaumont Hospital: Doctors Victoria Sharp and Thomas Serena
Boston Medical Center: Doctors George Kasotakis and Sean Perez
Carilion Clinic: Doctors Stacie L. Allmond and Bruce Long
Cooper University Hospital: Doctors Nadine Barth and Janika San Roman
Denver Health: Doctors Ryan A. Lawless and Alexis L. Cralley
Emory University: Doctors Rondi Gelbard and Crystal Szczepanski
Essentia Health: Doctors Steven Eyer and Kaitlyn Proulx
Geisinger Medical Center: Doctors Jeffrey Wild and Katelyn A.Young
Inova Fairfax: Doctors Erik J. Teicher and Elena Lita
Intermountain Medical Center: Doctors David Morris and Laura Juarez
Loma Linda University: Doctors Richard D. Catalano and David Turay
Marshfield Clinic: Doctors Daniel C. Cullinane and Jennifer C. Roberts
Massachusetts General Hospital: Doctors Haytham M.A. Kaafarani and Ahmed I. Eid
Mayo Clinic: Doctors Mohamed Ray-Zack and Tala Kana'an
Medical City Plano: Doctors Victor Portillo and Morgan Collom
Medical College of Wisconsin: Doctors Chris Dodgion and Savo Bou Zein Eddine
North Shore Medical Center: Doctors Maryam B. Tabrizi and Ahmed Elsayed Mohammed Elsharkawy
Ryder Trauma Center: Doctors D. Dante Yeh and Georgia Vasileiou
Ohio State University Wexner Medical Center: Doctors David C. Evans and Daniel E. Vazquez
St. Vincent Hospital Indianapolis: Doctors Jonathan Saxe and Lewis Jacobson
Oregon Health Sciences University: Doctors Brandon Behrens and Martin Schreiber
University of Arizona, Tucson: Doctors Bellal Joseph and Muhammad Zeeshan
University of California, Irvine: Doctors Jeffry Nahmias and Beatrice Sun
University of Florida, Jacksonville: Doctors Marie Crandall and Jennifer Mull
University of Maryland: Doctors Jason D. Pasley and Lindsay O'Meara
University of Southern California: Doctors Ali Fuat Kann Gok and Jocelyn To
Walter Reed National Military Medical Center: Doctors Carlos Rodriguez and Matthew Bradley
Funding Information
No funding was received for the production of this manuscript.
Author Disclosure Statement
D.D.Y. has received author royalties from UpToDate and research funding for an investigator-initiated trial from Takeda (formerly Shire). The remaining authors have nothing to disclose.