
Abstract
When patients with significant comorbid risk factors undergo surgical procedures, they are at high risk for development of post-operative infectious complications, including surgical site infection (SSI). Obese patients characteristically fit within this risk category, and thus it is of paramount importance to establish evidence-based strategies to mitigate these infectious complications. The use of an antimicrobial prophylactic regimen is a well-established practice and is based on the principle of the “right drug, at the right time, in the right place.” The subject of this article is to review the current evidence-based data on antimicrobial prophylaxis in obese patients undergoing bariatric surgical procedures.
Obesity is a multi-factorial condition that is increasing worldwide, and it is considered a major health problem to be challenged globally. It is associated with several impairments to the quality of life, quite often related to other comorbid conditions (e.g., type 2 diabetes mellitus and hypertension) [1]. A bariatric surgical procedure is an invasive approach that has been successful in producing massive weight loss and substantial improvements in obesity-related comorbidities [2]. It is also considered a safe procedure, with a small number of short-term complications, among which the most frequent are surgical site infection (SSI), gastrojejunostomy leak, pulmonary embolism, and gastrojejunostomy stenosis [3].
Patients with obesity are at risk to present with post-operative infectious complications, and SSI is the most prevalent condition [4]. Specifically, for the bariatric patient, this accounts for increased length of stay, increased health costs, and long-term post-operative complications, such as incisional hernia, being responsible for significant damages to the post-operative course of these patients [1,4]. Thus, it is plausible to assume that patients undergoing bariatric surgical procedures require special attention, focusing on evidence-based risk reduction strategies in pre- and peri-operative management, mitigating the risk of infection.
This review assesses the relevant literature regarding the use of antibiotic prophylaxis in patients undergoing bariatric surgical procedures for the prevention of SSI, focusing upon what would be the ideal agent and regimen for this type of operation. The following question was asked according to Population, Intervention, Comparison, and Outcome criteria: “Is there an ideal antibiotic prophylaxis regimen for patients undergoing bariatric surgery?”
Methods
Randomized clinical trials as well as prospective, retrospective, and cross-sectional studies that analyzed the use of specific antibiotic prophylaxis regimens in preventing SSI after bariatric surgical procedures were reviewed. In situ, in vitro, and animal studies, previous literature reviews, and case reports were excluded from analysis. The analysis included both men and women with obesity undergoing bariatric operation who had received antibiotic prophylaxis.
The authors reviewed studies involving any prophylaxis agents that were administered either intravenously (IV), orally, topically, or by intramuscular injection. Studies where antibiotic agents where administered to treat any infection present on admission were excluded from our analysis.
The main outcome studied in this review was the rate of SSI. The definition and diagnosis of SSI often varied between published studies, but has the common feature of pus expressed from the surgical incision or an intra-abdominal infectious process within the manipulated structures at operation. Besides the occurrence of SSI, we also focused on the tissue concentrations of the most common prophylactic agents, to assess whether the antibiotic level within the surgical site during the intra-operative period were appropriate for the common surgical pathogens.
We searched in the Pubmed/MEDLINE, Cochrane Library and Scientific Electronic Library Online (SciELO) databases, using the following combination of terms: “antibiotic prophylaxis” AND “bariatric surgery.” This review covered all studies published between 2004 and 2019 in English, Portuguese, and Spanish languages. The selection of articles was performed by two different authors from title and abstract screening. Divergences between evaluators were resolved through consensus.
Results
The initial database search found a total of 56 articles, including 50 in Pubmed/MEDLINE, three in Cochrane Library, and three in SciELO. After the exclusion of duplicates, 51 articles remained, among which 24 were selected after title and abstract screening. Three studies were excluded because they did not meet the eligibility criteria. Twenty-one full-text articles were screened. Five studies were excluded after full-text screening. Two of them were excluded for being review articles. The other three articles were excluded because of limited data on how many patients received each specific regimen of antibiotic prophylaxis. Figure 1 summarizes the process of selecting studies.
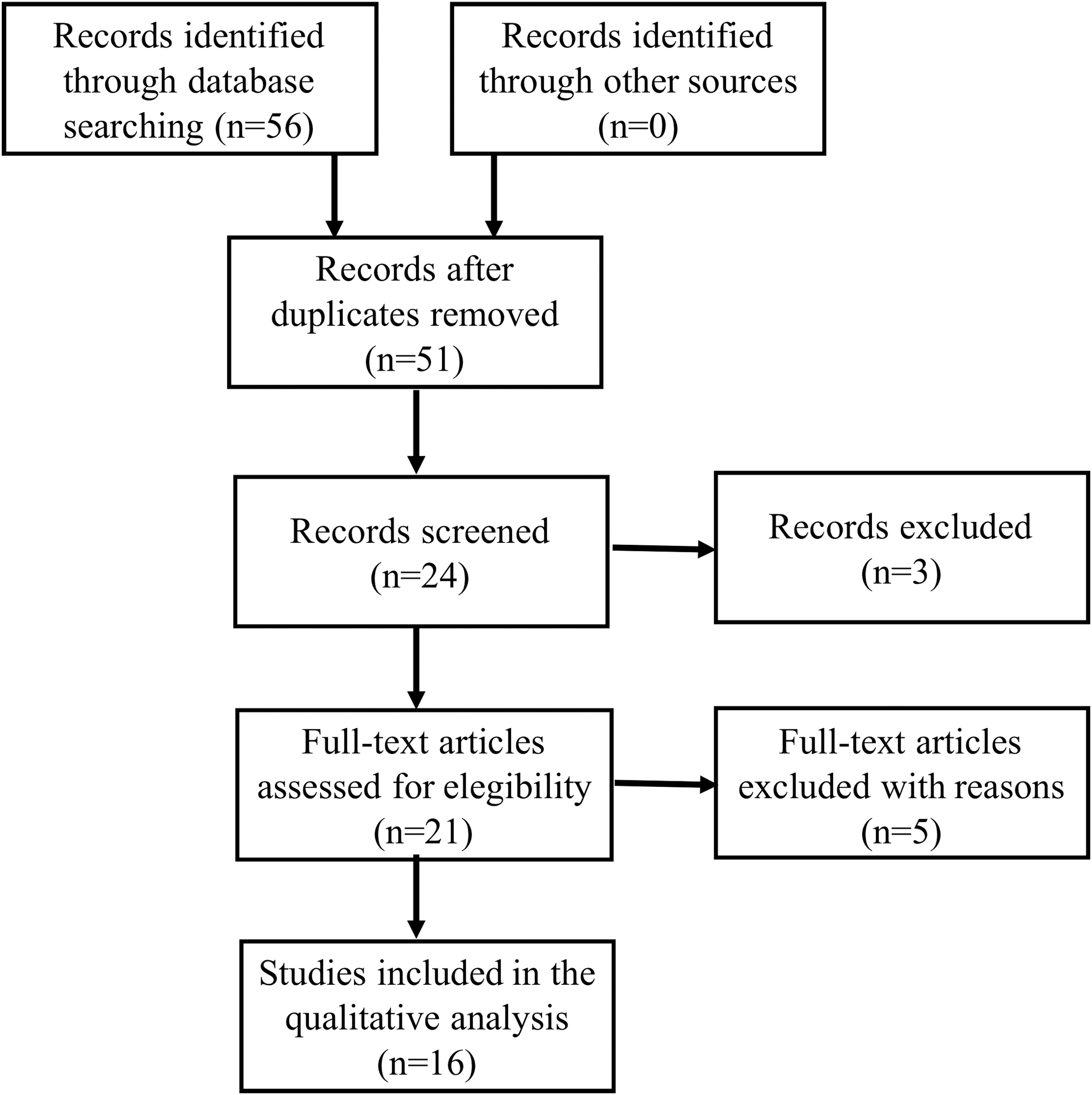
Flowchart of the studies selection.
Overall, 3,497 patients were analyzed within the included studies. A total of 10 antibiotic agents were assessed: Cefazolin, cefoxitin, ertapenem, ampicillin/sulbactam, ceftriaxone, clindamycin, kanamycin, levofloxacin, metronidazole, and bacitracin. Sleeve gastrectomy (SG) was performed in seven studies, Roux en Y gastric bypass (RYGB) in 10, gastric banding (GB) in one, and biliopancreatic diversion (BPD) in one other study. The majority of the studies included in this review documented a higher prevalence of women undergoing bariatric operations.
Table 1 summarizes the detailed data regarding all of the antibiotic prophylaxis regimens from each of the 16 studies that were selected for this review.
Characteristics of the Included Studies
Included other types of elective surgery besides bariatric surgical procedure.
SSI = surgical site infection; BMI = body mass index; F = female; IV = intravenous infusion; ORYGB = open Roux-en-Y gastric bypass; PS = prospective study; SG = sleeve gastrectomy; CI = continuous infusion; NR = not reported; LRYGB = laparoscopic Roux-en-Y gastric bypass; LSG = laparoscopic sleeve gastrectomy; RS = retrospective study; RYGB = Roux-en-Y gastric bypass; CC = case-control study; SC = subcutaneous infusion; IP = intraperitoneal irrigation; GB = gastric banding; BPD = biliopancreatic diversion.
Discussion
Overview
Three studies that have used cefazolin found a SSI rate of 0.0%; however, two of them included a small number of patients, which might have undermined these rates [6–8]. Chen et al. [7] found that the administration of 2 g (IV bolus just before the surgical incision) was sufficient to provide adipose tissue concentrations of cefazolin above the minimum inhibitory concentration (MIC) of Staphylococcus aureus (1 mg/L) for up to 4 h. They concluded that, because of this pharmacokinetic pattern, no redosing would be necessary for RYGB.
Alincoara et al. [8] used cefazolin 2 g with an addition of 1 g in IV continuous infusion and found that its concentration in the adipose tissue remained above the MIC of the most prevalent pathogens, including gram-positive cocci (1 mg/L) and gram-negative cocci (4 mg/L), in all patients during the entire operative time.
Alternatively, Cinotti et al. [6], using cefazolin 4 g IV, found 0.0% of SSI with a sample of 116 patients, including obese and superobese patients. This study has also observed that this dose was able to provide high fatty-tissue antibiotic concentration, above the MIC of S. aureus, in patients with a body mass index between 40 and 50 kg/m2, presenting good coverage for the entire operative time. Chopra et al. [1], in a case-control study, using a dose of 1–2 g cefazolin, observed post-operative infection rates of 11.3% (1 g) and 23% (2 g), respectively.
Edmiston et al. [9], using a cefazolin dose 2 g 30–60 min before the beginning of the procedure plus another 2 g 3 h after the skin incision, observed an infection rate of 18.4%. They also assessed the serum and tissue concentrations and determined that this antimicrobial regimen resulted in intra-operative subtherapeutic concentrations of cefazolin within the surgical site in the bariatric population.
Grégoire et al. [10] compared four different regimens of administration of cefazolin in patients undergoing bariatric operation and found that doses of 2 g and 3 g, administered 30 min before the surgical incision, did not achieve sufficient concentrations in the adipose tissue. The administration of cefazolin 4 g, however, was able to provide levels above the MIC of Staphylococcus spp and Streptococcus spp (≤ 2 mg/L) for up to 2 h. They have also demonstrated that, in cases where the surgical procedure would last longer or when a pathogen exhibited a higher MIC (until 4 mg/L), cefazolin 3 g associated with 1 g in IV continuous infusion was optimal, providing adequate prophylactic coverage for up to 4 h.10
In 2007, Ferraz et al. [11] studied 716 patients undergoing open RYGB. They divided the sample into three groups according to the antimicrobial prophylaxis regimen: Ampicillin/sulbactam (185 individuals) two IV doses of 3 g; ceftriaxone (280 individuals) single IV dose of 1 g; and ertapenem (251 individuals) single IV dose of 1g. The incidences of SSI with the aforementioned regimens were 3.78%, 6.81%, and 1.99%, respectively. The best results were related to the use of ertapenem, and the difference was statistically significant (p < 0.05).
In a similar subsequent cohort, Ferraz et al. [2] divided 896 patients undergoing open RYGB into three groups according to the antimicrobial prophylaxis: Cefazolin, ertapenem, and ampicillin/sulbactam. Cefazolin 2 g, administered IV, exhibited the best results, achieving a SSI rate of 1.55% (ertapenem 1 g: 1.98%; ampicillin/sulbactam 3 g: 4.16%). This difference between the infection rates after each antibiotic used was not statistically significant, however.2
Two studies evaluated the efficacy of cefoxitin as a prophylactic agent in bariatric surgical procedures through an assessment of its pharmacokinetic and pharmacodynamic characteristics [12,13]. Moine et al. [12] used a weight-based dosing (40 mg/kg) of cefoxitin and studied its concentration in adipose tissue. They found that the tissue penetration was poor, with cefoxitin levels remaining below the MIC of Escherichia coli, Bacteroides fragilis, and S. aureus at 1 h post-dose.
Similarly, Brunetti et al. [13] analyzed adipose tissue concentrations of cefoxitin after the administration of 2 g of this antibiotic agent before bariatric operation, and found that this regimen was unable to provide effective serum or tissue concentrations in their sample at the time of skin closure.
De Werra et al. [14] studied the efficacy of a single dose of ertapenem 1 g through the assessment of serum antimicrobial activity for gram-positive and gram-negative bacteria. They observed that, with the aforementioned regimen, the growth of non-extended beta lactamase (ESBL)-producing E. coli, non-ESBL-producing Klebsiella pneumoniae, Proteus mirabilis, Citrobacter freundii, Enterobacter cloacae, S. aureus, and S. viridans were inhibited. Moreover, the SSI rate was 3.12%. Borracci et al. [15] also studied the use of ertapenem 1 g 30 min before bariatric operation in severely obese female patients and found that serum, peritoneal, and liver concentrations, with this regimen, were not sufficient in providing effective intra-operative concentrations.
Alexander et al. [16] have studied the association of cefazolin 1.5 g IV right before the incision with a subcutaneous injection of kanamycin 15–100 mcg at the skin closure in patients undergoing bariatric surgery. In their first cohort, they analyzed 400 patients, and the SSI rate found was 1.0%. Their most recent cohort analyzed 772 patients, and the SSI rate was 2.85% [17].
Williams et al. [18] have used a levofloxacin dose 500 mg IV associated with metronidazole 500 mg IV for antibiotic prophylaxis in RYGB. They also administered intra-peritoneal irrigation with bacitracin 50,000 U and kanamycin 1 g after the jejunojejunostomy. Using this protocol, they found no cases of SSI in a sample of 66 patients with obesity.
Commentary
Obesity increases the volume of distribution for several drugs, including antibiotic agents [2,19]. Therefore, the usual doses of these drugs might not be sufficient to reach satisfactory concentrations within the adipose tissue of patients with obesity, and weight-based dosing could be an interesting approach to solving this problem [9]. There is a lack in the literature, however, of studies comparing weight-based regimens with the usual antibiotic prophylaxis protocols.
Contrastingly, it has been suggested that, because of the hydrophilic nature and time-dependent concentration of cefazolin, it would not be plausible to implement doses higher than the usual (1 g, IV) for clean-clean-contaminated procedures in the obese patient [19]. Blum et al. [19] have stated that cefazolin 1 g IV as a bolus before the incision is enough to reach a peak serum concentration of 185 mcg/mL at incision, and 4 mcg/mL at 8 h in obese patients. It is important to point out, however, that serum concentrations do not correlate well in patients who demonstrate hypoperfusion, which is characteristic of the obese patient population.
Chopra et al. [20] proposed that patients undergoing bariatric surgical procedures involving the duodenum and above should receive first generation cephalosporins (e.g., cefazolin). Individuals undergoing procedures involving structures below the duodenum, such as RYGB, however, would benefit from the administration of agents with anaerobic activity also (e.g., cefoxitin or cefazolin + metronidazole). Nevertheless, the current review has shown (Table 1) that, even for patients undergoing RYGB, cefazolin exhibited better results for SSI prophylaxis when compared with cefoxitin.
Despite the fact that prophylactic regimens that present abroad spectrum of activity, such as ampicillin/sulbactam and ertapenem, are effective against the most common pathogens in post-bariatric operation SSI, these agents should be reserved as therapeutics for the management (and not prophylaxis) of established infections.20
For patients who are allergic the β-lactam agents, alternative agents, such as levofloxacin or clindamycin associated with an aminoglycoside, could be an option. In general, vancomycin, however, should not be viewed as an option for patients because it has been largely demonstrated that methicillin-resistant S. aureus is rarely the cause of infection in these patients [20]. Moreover, Freeman et al. [4] have reported a higher incidence of post-bariatric SSIs cause by gram-negative bacteria when vancomycin was used as a surgical prophylactic agent.
The major limitation of the current studies discussed in this article reside in the relatively small number of patients presented in many of the various studies and the scarcity of adequate control populations. It is difficult to establish solid conclusions regarding the optimal prophylactic agent, in part because of the heterogeneity of the data presented in the literature. Several antibiotic regimens have been used to prevent SSI in bariatric operations.
Some of the studies, however, have not included SSI rates in their analysis, focusing only on the tissue concentration of the agents used; others have assessed a limited population of patients with discordant co-morbid risk. This becomes somewhat problematic when there is no stratification of patients' demographics (e.g., smokers, those with diabetes mellitus, those who consume alcohol, etc.), which may lead to investigator bias.
Undoubtedly, cefazolin is the most used, most studied, and most effective agent for bariatric surgical procedures, according to the literature. Therefore, for the time being, the administration of this drug, right before anesthetic induction, should be considered as first choice for antibiotic prophylaxis in bariatric operations. Dosing, however, is still an issue, with several different regimens reporting miscellaneous results.
Conclusion
In times of antimicrobial stewardship, it is important to establish what would comprise the ideal antibiotic prophylaxis in obese patients undergoing bariatric surgical procedures, aiming to reach the lowest SSI rates, using the simplest agent in the lowest doses possible, thus avoiding bacterial resistance and increased health costs. Ironically, however, the lowest possible dose may very well lead to subtherapeutic tissue levels in the bariatric patient, and the fastest route to bacterial resistance is not antibiotic overuse but rather exposing a microbial population to a subtherapeutic concentration of antibiotic in a vulnerable comorbid patient population.
Therefore, it is of paramount importance that bariatric investigators seeking to discern the optimal surgical prophylactic regiment look to sufficiently powered randomized, controlled trials that include pharmacokinetic analysis of intra-operative tissue concentrations correlated with surgical outcomes.
Footnotes
Acknowledgment
The authors thank the late Prof. Edmundo Machado Ferraz for all his contribution and motivation in the surgical site infection and bariatric surgery fields.
Funding Information
This article did not receive financial support.
Author Disclosure Statement
No competing financial interests exist.