
Abstract
Background:
Sarcopenia is a syndrome that can be associated with unfavorable outcomes after colorectal cancer surgical procedures. The present study evaluates the relationship between sarcopenia and surgical site infections (SSIs) that can occur after colorectal cancer operations and that are a significant cause of morbidity.
Methods:
The research was designed as a retrospective study in which data were collected on patients who underwent colorectal cancer surgical procedures between January 2013 and July 2019. A diagnosis of sarcopenia was established based on the skeletal muscle index (SMI), calculated from pre-operative computed tomography scans. The SSI scores of patients with sarcopenia (sarcopenic group, SG) and those without sarcopenia (non-sarcopenic group, NSG) were compared, and a logistic regression analysis was performed to determine the risk factors for SSI.
Results:
A total of 209 patients with a mean age of 61.2 years were included in the study. Post-operative complications (Clavien-Dindo ≥1) developed in 97 (46.4%) patients, SSIs developed in 46 (22%) patients, and sarcopenia developed in 97 (46.4%) patients. The mean age was 64.8 years in the SG group and 58.1 years in the NSG group (p = 0.016). No significant relationship was found between the development of SSI and sarcopenia (20 (20.6%) patients in the SG vs. 26 (23.2%) patients in the NSG, p = 0.65). Those in whom superficial SSIs developed in the early period formed the largest group (20 patients). The most commonly detected micro-organism was Escherichia coli with a rate of 55%. In a multi-variable logistic regression analysis, only the non-laparoscopic approach was identified as a risk factor (odds ratio 3.83; 95% confidence interval 1.26–11.58; p = 0.017).
Conclusions:
The present study reports no relationship between sarcopenia and SSI after colorectal cancer operations. The authors consider that studies that endeavor to reduce the incidence of SSI, as a significant cause of morbidity after colorectal surgical procedures, should be supported.
Surgical site infections (SSIs) are the most common of all nosocomial infections, with a rate of approximately 38% [1,2]. This rate has been shown to be 3%–30% among patients undergoing colorectal cancer surgical procedures and is still an important cause of morbidity [2,3]. The SSIs prolong hospital stays and cause a delay in the administration of adjuvant therapy. Various risk factors have been identified for the development of SSIs, but the rate of infections after colorectal cancer operations still remains high, despite preventive measures [4].
Sarcopenia is a syndrome that causes a progressive and generalized loss of skeletal muscle. This condition is often associated with aging, but it has also been linked to such factors as poor nutrition, immobility, inflammatory diseases, and cancer, which can occur at any age [5]. Recent studies have shown that sarcopenia increases the risk of complications after colorectal cancer surgical procedures [6], and while there are a limited number of studies suggesting that sarcopenia increases the likelihood of post-operative SSIs, there have been other studies suggesting the contrary [7,8]. Accordingly, there is still a level of uncertainty regarding the effects of sarcopenia on SSIs that result in unfavorable patient outcomes.
Various methods have been put forward for the establishment of a diagnosis of sarcopenia, among which the measurement of lumbar muscle cross-sectional area on computed tomography (CT) scans has become popular because of the practicality of the approach. The present study evaluates the effect of sarcopenia on SSI after colorectal cancer operations using this measurement method.
Methods
Data for the present study were garnered through a retrospective review of the medical records of patients who underwent colon and rectal cancer surgical procedures in the gastrointestinal surgery clinic of the study center. The study was approved by the ethics committee of the study hospital with decision number 2019.4/2-179. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki, revised in 2013. Medical records in the hospital archive for the period between January 2013 and July 2019 were reviewed. When required, the data were confirmed through phone contacts with the patient.
Patients aged 20 years and older with an Eastern Cooperative Oncology Group (ECOG) performance status of ≤2 who underwent elective operation because of colon or rectal cancer were included in the study. Patients with a pathologic diagnosis other than adenocarcinoma, those with stage 4 disease, those undergoing a palliative procedure, those for whom abdominal CT scans obtained in the last month before operation were not available, and those necessitating additional organ resection to reduce the number of anastomoses were excluded from the study.
The patients were divided initially into two groups, based on the presence of sarcopenia. Diagnoses of sarcopenia were based on pre-operative CT scans. The total psoas area (TPA) of the bilateral psoas muscles in a sequence visualizing the two transverse processes at the lumbar 3 (L3) vertebra level was measured and calculated by the consulting radiologist. The Hounsfield unit scale (-29 to +150) was used to differentiate between skeletal muscle and other structures. The total area was proportioned to the height of the patient. According to general consensus, a skeletal muscle index (SMI) <545 mm2/m2 in males and <385 mm2/m2 in females points to sarcopenia [9].
The demographic data of the patients and the development of post-operative SSI were compared between the two groups. The surgical site was evaluated for the presence of infection, as per the diagnostic criteria set out by the Centers for Disease Control and Prevention (CDC). The SSIs were divided into three groups: Superficial, deep, and organ/area [10]. An SSI developing within one week of operation was defined as early SSI, while those developing between one week and 30 days post-operatively were defined as late SSI. All SSI diagnoses were made by surgeons working in the gastrointestinal surgery department. An SSI diagnosis of outpatients was made during the post-operative follow-up.
The weight-height measurements of the patients in the week before operation, the body mass index (BMI >30 classified as obese), and the hemoglobin values were recorded. Patients who previously underwent abdominal operation for any reason, those undergoing therapy for diabetes mellitus, and those receiving neoadjuvant chemotherapy were recorded. Those who had smoked within the last month were considered to be active smokers.
The patients were also evaluated for the use of immunonutrition, referring to a nutrition style that preserves and strengthens immune response and that suppresses exaggerated and harmful inflammatory response [11]. Immunonutrition is provided in our clinic as a five-day course before and after operation, as recommended by guidelines [11,12], and involves the daily intake of 20 g glutamine, 4.3 g arginine, 0.43 g ribonucleic acid, 1.4 g omega-3 fatty acid, and antioxidants. The patients who use immunonutrition regularly were also recorded, as well as those undergoing ostomy opening, operative time, amount of intra-operative blood loss, pathologic stage, patients experiencing post-operative complications (according to the Clavien-Dindo classification, patients ≥1), and length of hospital stay.
Statistical analysis
Normally distributed data were expressed as mean ± standard deviation. Categoril variables were expressed as number and percentage. Clinical variables were compared using the Student t test and Pearson chi-square test. Factors affecting SSIs were evaluated using a logistic regression analysis. Variables with a p value less than 0.1 in a uni-variable analysis were included in the multi-variable logistic regression analysis; a p value less than 0.05 was considered to be significant in all tests. All statistical analyses were performed using SPSS statistics version 25.0 (IBM, Armonk, NY).
Results
Excluded from the study were 11 patients who underwent operation in our clinic but for whom pre-operative CT data were absent, and five patients with missing data. The study included 209 patients undergoing colon cancer surrical procedures whose pre-operative CT images were available. Of the total, 118 (56.5%) patients were male; the mean age was 61.2 years; 42 (20.1%) patients had diabetes mellitus; and 54 (25.8%) patients were active smokers. Post-operative complications occurred in 97 (46.4%) patients, and SSIs occurred in 46 (22%) patients. The demographic data of the patients are presented in Table 1.
Clinical Characteristics of the Patients
Values are presented as mean ± SD (standard deviation) or n (%). BMI = body mass index; ASA = American Society of Anesthesiologists.
Of the total, 97 (46.4%) patients had a diagnosis of sarcopenia. The mean age was 64.8 years in the sarcopenic group (SG), which was significantly higher than in the non-sarcopenic group (NSG) (p = 0.016). Both TPA and SMI were found to be associated with sarcopenia (p < 0.001 and p = 0.001, respectively). Age distribution of SMI is presented in Figure 1 (a,b). Post-operative complications were found to be unrelated to sarcopenia (46 [47.4%] patients in the SG; 51[45.5%] patients in the NSG; p = 0.78).
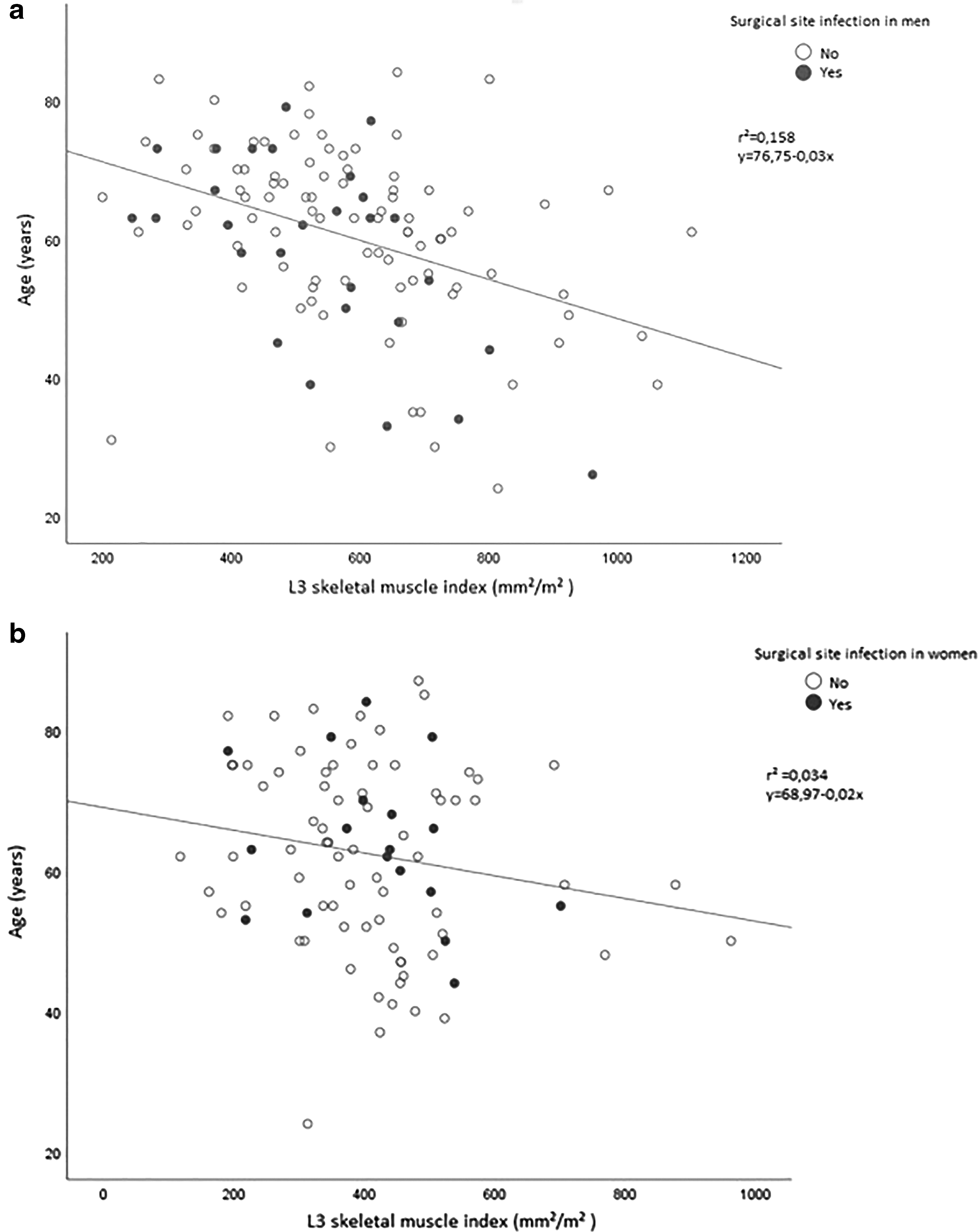
Scatterplots depicting the relationship between age and skeletal muscle index, and the incidence of surgical site infection in (
No significant difference was identified between the groups in terms of the distribution of potential risk factors for SSIs, such as diabetes mellitus, smoking, peri-operative use of immunonutrition, history of neoadjuvant therapy, laparoscopic approach, amount of intra-operative blood loss, duration of operation, and pre-operative hemoglobin levels. Although the length of hospital stay was longer in the SG, the difference was not statistically significant (p = 0.07). No significant relationship was found between the development of SSI and sarcopenia (20 [20.6%] patients in the SG vs. 26 [23.2%] patients in the NSG, p = 0.65). It was also seen that sarcopenia had no effect on the depth of infection and the time of detection (Table 2).
Demographic and Clinical Factors Associated with Sarcopenia
SD = standard deviation; BMI = body mass index; TPA = total psoas area; SMI = skeletal muscle index; ASA = American Society of Anesthesiologists; SSI = surgical site infection.
The SSIs occurred in the early period in 30 of the 46 patients in whom SSIs developed, and in the late period in 16 patients. Those in whom superficial SSI developed in the early period formed the largest group of patients (20). Deep SSIs were detected in a total of 13 patients, and eight patients had SSIs involving an organ/area (Table 3). A micro-organism was recovered from the surgical site in 26 patients, with the most commonly isolated organism being Escherichia coli (55%) followed by Staphylococcus aureus (20%), Klebsiella pneumoniae (13%), and Enterococcus faecalis (9%).
Location of Surgical Site Infection
Factors leading to SSI were investigated. In a uni-variable logistic regression analysis, non-laparoscopic operation (odds ratio [OR] 4.51; 95% CI 1.53–13.27; p = 0.006) and operative time exceeding 180 min (OR 2.15; 95% conficence interval [CI] 1.09–4.16; p = 0.026) were found to be associated with SSI. In a multi-variable analysis, non-laparoscopic operation (OR 3.83; 95% CI 1.26–11.58; p = 0.017) was found to be an independent risk factor for SSI (Table 4).
Uni-Variable and Multi-Variable Analysis of Risk Factors for Surgical Site Infection
OR = odds ratio; CI = confidence interval; ASA = American Society of Anesthesiologists; BMI = body mass index.
Discussion
Sarcopenia is defined as a syndrome that occurs with aging secondary to other diseases and is characterized by a loss in muscle mass and strength [13]. The mean age was significantly higher in the SG (p = 0.016), although sarcopenia can also develop in the presence of cancer, regardless of the patient's age. In a previous review of the literature, sarcopenia assessed by CT was found to be associated with overall survival in gastrointestinal malignancies and post-operative morbidity [14]. The present study identified sarcopenic patients via muscle mass measurements on pre-operative CT scans. No significant difference was noted between the groups in terms of patient-related values and operative factors. Although the mean age was higher in the SG, age did not appear as a risk factor for SSI in a univariable analysis.
The SSIs continue to be a significant cause of morbidity after colorectal cancer surgical procedures. Although various methods to reduce the incidence of infections have been reported in recent years, the rate of infection has not dropped below negligible levels, and the length of hospital stay continues to be long [15]. A large number of risk factors have been identified after colorectal operations in which diabetes mellitus, obesity, prolonged operative time, and a non-laparoscopic approach have been commonly implicated [16,17].
In recent years, there have been a number of studies reporting the effects of sarcopenia on SSI. The study by Lieffers et al. [7] was the first to demonstrate a relationship between sarcopenia and post-operative infections after colorectal cancer surgical procedures, although the study did not differentiate between infection types. Nishigori et al. [18] reported a relationship between sarcopenic obesity and SSI in patients undergoing a laparoscopic total gastrectomy (p = 0.03). In their study, the negative consequences of sarcopenic obesity were emphasized, but a rate of 20% for SSI is considerably high for gastric operation, and the rate of SSI was similar to that reported in the present study.
A study evaluating SSIs reported that sarcopenia is an independent risk factor for sarcopenia in 69 patients undergoing restorative proctocolectomy because of ulcerative colitis (p = 0.03) [19]. The rate of SSI in our study of 209 patients who underwent colorectal cancer operation was 22%, similar to that reported in the literature, although no relationship was found between sarcopenia and SSI (p = 0.65).
The overall rate of complications in our study was 46.4%, with a similar distribution of complications across the groups (p = 0.78). Parallel to this, the rate of SSI was similar between the groups, and this finding supports the notion that sarcopenia has no specific effect on SSI. Studies demonstrating the negative effects of sarcopenia on SSI have not provided an explanation of the mechanism behind this effect [18,20].
In a similar study, SSIs were more commonly observed in the sarcopenic group after hepato-biliary-pancreatic surgical procedures, although the length of hospital stay was similar between the groups. A considerably large number of studies have reported that sarcopenia prolongs the length of hospital stay [21–23]. In the present study, the length of hospital stay was longer in the SG (10.5 vs. 12.3 d), but this was not supported by a significant difference in the statistical analysis (p = 0.07). The authors attribute this finding to the overall complication rates and the rate of SSI being similar between the groups.
When the risk factors for SSI are examined, only the non-laparoscopic approach turned out to be significant in the multi-variatble analysis. Advanced age, obesity, intra-operative blood loss, diabetes mellitus, not using peri-operative immunonutrition, colostomy or ileostomy opening did not appear to be a risk factor for SSI. Operative times of ≥180 min appeared to be significant in the uni-variable analysis, but it was significant in the multi-variable analysis. These results are partially consistent with those in the literature.
The present study has several limitations, the first of which is the single-center and retrospective study design, which may have biased the patient selection and the collection of study data. Despite its retrospective design, however, some data were collected prospectively without changing the follow-up strategy. Parameters such as grip strength, walking speed, and fatigue were not evaluated, and 11 ineligible patients who lacked CT scans acquired within the last 30 days pre-operatively could not be evaluated for sarcopenia. Prospective studies involving a larger number of patients may reduce the complications.
Another factor that can be regarded as a limitation is that no cutoff values were determined for the SMI. While we could have defined a cutoff value, the study was conducted using a universally accepted value because sarcopenia shows significant differences across race, gender, and age groups.
Conclusion
The present study did not identify sarcopenia as a risk factor for the development of SSI colorectal cancer operation. This result may differ from those reported for other gastrointestinal tract disorders; although colorectal surgical procedures are associated with the highest rate of SSI, and the present study found that only the laparoscopic approach reduced the rate of SSI. The authors consider that studies must be supported that endeavor to reduce the incidence of SSI, as a significant cause of morbidity after colorectal surgical procedures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.