
Abstract
Background:
Fungal infections are associated with increased morbidity and death. Few studies have examined risk factors associated with post-operative fungal intra-abdominal infections (FIAIs) in trauma patients after exploratory laparotomy. In this study, we evaluated potential risk factors for acquiring post-operative FIAIs and their impact on clinical outcomes.
Methods:
This was a retrospective analysis of trauma patients admitted from 2005 to 2018 who underwent exploratory laparotomy and subsequently had development of intra-abdominal infection (IAI). Demographics, comorbidities, culture data, antimicrobial usage, Injury Severity Scores (ISS), and clinical outcomes were abstracted. All post-operative IAIs were evaluated and stratified as either bacterial, fungal, combined, and with or without colonization. All groups were compared. Risk factors for the development of post-operative IAI and clinical outcomes were analyzed by Student t test and chi-square test. Multi-variable logistic regression was used to determine independent predictors of post-operative FIAIs.
Results:
There were 1675 patients identified as having undergone exploratory laparotomy in the setting of traumatic injury, 161 of whom were suspected of having IAI. A total of 105 (6.2%) patients had a diagnosis of IAI. Of these patients, 40 (38%) received a diagnosis of FIAI. The most common fungal pathogens were unspeciated yeast (48.3%), followed by Candida albicans (42.7%), C. glabrata (4.5%), C. dubliniensis (2.25%), and C. tropicalis (2.25%). There were no significant differences in demographics, comorbidities, and percentage of gastric perforations between FIAI and bacterial IAI (BIAI) groups. Patients with FIAIs, however, had a 75% temporary abdominal closure (TAC) rate compared with 51% in BIAIs (p = 0.01). The FIAI group had higher ISS (27 vs. 22, p = 0.03), longer hospital days (34 vs. 25, p = 0.02), and longer intensive care unit (ICU) days (17 vs. 9, p = 0.006) when compared with BIAI. The FIAI group also had a five-fold greater mortality rate. Logistic regression identified TAC as an independent risk factor for the development of post-operative FIAIs (odds ratio [OR] 6.16, confidence interval [CI] 1.14–28.0, p = 0.02).
Conclusions:
An FIAI after exploratory laparotomy was associated with greater morbidity and death. A TAC was associated independently with increased risk of FIAI after exploratory laparotomy in the setting of traumatic injury. Clinicians should suspect fungal infections in trauma patients in whom post-operative IAI develops after undergoing exploratory laparotomy using TAC techniques.
Severely injured trauma patients constitute a unique surgical population that is at risk for serious infections because of their immunocompromised status [1]. In addition, the mechanism of many traumatic injuries, such as blunt or penetrating traumas, pose further infection risk for these patients by contamination from external pathogens because of compromised epithelial barriers as well as their own enteric florae.
Fungal infection has a 30%–70% increased risk of morbidity rate in trauma and a mortality of up to 38% with fungemia [2–6]. Trauma patients with abdominal injuries have increased incidence of both fungal colonization and fungal infection of the abdominal cavity from enteric and external fungal species; however, there have been few studies investigating outcomes and risk factors for acquiring fungal intra-abdominal infections (FIAIs) in post-operative trauma patients. We investigated the incidence of FIAI in trauma patients undergoing exploratory laparotomy, analyzed independent risk factors associated with FIAI, and examined subsequent clinical outcomes.
Methods
We retrospectively analyzed our Institutional Review Board-approved and prospectively maintained trauma registry containing more than 37,000 patients collected over a 14-year period from 2005 to 2018. Patients who underwent exploratory laparotomy because of either blunt or penetrating trauma were abstracted. Those patients with a clinical suspicion of post-operative intra-abdominal infection (IAI) were identified using intra-abdominal fluid cultures obtained at least 48 h after the initial operation based on the Surgical Infection Society (SIS) guidelines [7–9].
Of the patients with suspected IAI, individual charts were reviewed to stratify further patients who had FIAIs and those who had bacterial IAIs (BIAIs). Patients who had positive intra-abdominal culture results for fungal species in addition to receiving anti-fungal therapy for ≥ four days were classified as having FIAIs, whereas patients who had positive culture results for bacterial species and were treated with antibiotic agents for ≥ four days were classified as having BIAIs. Four days of antibiotic therapy was determined previously to be sufficient treatment for patients with IAIs after an adequate source control procedure in the STOP-IT trial [10].
Patients with FIAIs were classified further into those with FIAI alone or FIAI in addition to BIAI. Patients identified as having only BIAIs included those who had additional fungal colonization, defined as the presence of fungal species in intra-abdominal fluid cultures without ≥ four days of anti-fungal treatment, as well as those who had no fungal colonization (BIAI alone). An additional group of patients were identified who had either no bacterial or fungal species in culture, classified as patients without IAI, or those who had fungal species without bacteria in culture and did not receive ≥ four days of anti-fungal treatment, classified as fungal colonization only (Fig. 1). These patients were excluded from the study.
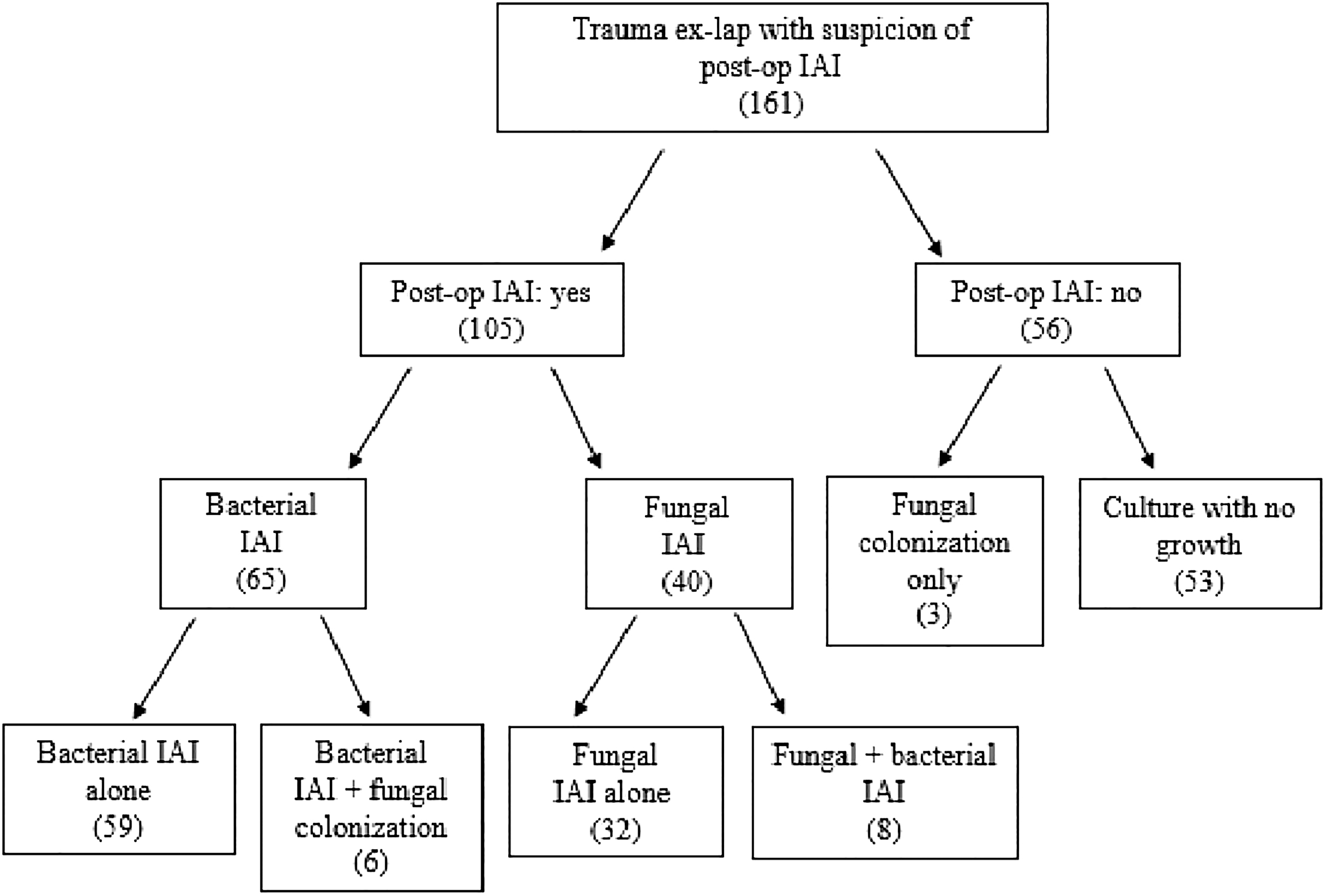
Post-operative Intra-abdominal infection study cohort diagram. The flowchart demonstrates study cohort selection and group division. Ex-lap = exploratory laparotomy; post-op = post-operative; IAI = intra-abdominal infection.
The collected patient data included demographics; Charleston Comorbidity Index (CCI); injury-related variables such as Glasgow Coma Scale (GCS) score at admission, Injury Severity Score (ISS), Abbreviated Injury Scale (AIS), mechanism of injury, traumatic bowel perforation location, and the presence of other intra-abdominal coinjuries; operative-related variables such as the use of drains, abdominal packing, temporary abdominal closure (TAC) management, duration of open abdomen (OA), number of abdominal re-operations before definitive abdominal closure, and type of abdominal wall closure; and post-operative variables such as time to IAI diagnosis, the number of antibiotic agents used, types of anti-fungal therapies, the use of total parenteral nutrition (TPN), intensive care unit (ICU) admission, and the presence of enteric leak, biloma or urinoma. Outcomes were classified as in-hospital death, hospital length of stay (LOS), ICU LOS, and ventilator days.
Variables and outcomes were compared between the BIAI and FIAI cohorts using uni-variable analysis. Frequencies were compared by chi-square test, and continuous variables were compared using the Student t test. After uni-variable analysis, logistic regression analysis with the forward method was run using the SAS 9.4 program to determine independent risk factors for development of post-operative FIAI. Multi-variable logistic regression analysis with the forward selection method was performed using all variables in the study. The independent variables that had a p-value of <0.25 in bivariable analysis were then selected for the final model. The last step model of the forward method was selected, taking into account the Hosmer-Lemeshow Goodness-of-Fit test (p > 0.05) [11–13].
Results
A total of 1675 patients were identified as having undergone exploratory laparotomy because of either blunt or penetrating trauma. Among these, 161 patients had intra-abdominal fluid cultures obtained at least 48 h after initial operation because of clinician suspicion for post-operative IAI. There were 56 patients excluded because of either negative fungal and bacterial intra-abdominal fluid culture results or the presence of fungal colonization without IAI. A total of 105 patients with post-operative IAIs were identified, with incidence of 6.2% (Fig. 1).
The average age of these patients was 33.4 ± 14.4 years; 90 (85.7%) were male, and 85 (81%) were black. The most common location of bowel injury was the large intestine (72.4%).
There were 40 (38.1%) patients with a diagnosis of FIAI, and 65 (61.9%) patients with a diagnosis of BIAI. There was no significant difference in the mean time (days) to diagnosis of IAI between the fungal and bacterial groups (11.2 ± 6.00 vs. 11.4 ± 6.60, p = 0.90).
Ninety-eight percent of patients received a diagnosis of IAI after abdominal closure of the initial operation, but only two patients had positive intra-abdominal culture results identified at the time of abdominal closure. Of these two patients, one had an identified bowel perforation from ischemia, and the other patient had an anastomotic leak.
Within the FIAI group, the most common pathogen was unspeciated yeast (48.3%), followed by Candida albicans (42.7%), C. glabrata (4.5%), C. dubliniensis (2.25%), and C. tropicalis (2.25%). For both the positive bacterial and fungal cultures, 87% of these were obtained via percutaneous abdominal fluid aspiration, 10% were obtained peri-operatively, and the remainder were obtained from drains placed near the fluid collection.
All patients in the study received prophylactic antibacterial therapy. Nine (13.8%) patients in the BIAI group and seven (17.5%) patients in the FIAI group received prophylactic anti-fungal therapy on presentation for injuries with abdominal contamination. Within the BIAI group, there were no differences in the top three most prevalent bacterial organisms regardless of the initial anti-fungal treatment (Bacteroides fragilis, Escherichia coli, and Enterococcus faecalis). In the FIAI group, there were also no differences in the prevalence of fungal species regardless of receiving initial anti-fungal therapy (C. albicans, C. glabrata, and unspeciated yeast) (Supplementary Tables 1–4).
There were no significant differences between the BIAI and FIAI groups in demographics, CCI, rate of traumatic gastric perforation on presentation, AIS score, or injury type (blunt vs. penetrating). Patients with a diagnosis of FIAIshad significantly higher ISS (27.0 ± 11.8 vs. 22.3 ± 9.50, p = 0.03). Post-operative FIAIs were more common in patients who underwent exploratory laparotomy because of gunshot wounds (GSW) (77.5% vs. 67.7%, p = 0.046) and motor vehicle collisions (MVC) (15% vs. 13.9%, p = 0.046).
Patients sustaining liver (50.0% vs. 29.2% p = 0.03) or splenic (27.5% vs. 12.3%, p = 0.0496) injuries were also more likely to have a diagnosis of post-operative FIAI (Tables 1 and 2). Eight (73%) patients in the FIAI group and all patients in the BIAI group with splenic injury were treated with splenectomy. There was no significant difference in the infection rate of the splenic bed between the two groups, however.
Demographics and Co-Morbidities of Patients with Post-Operative Intra-Abdominal Infection *
No statistically significant differences were found.
IAI = intra-abdominal infection; SD = standard deviation; CCI = Charlson Comorbidity Index.
Relationship between Post-Operative Fungal Intra-Abdominal Infection and Injury-Related Variables
Percentage sum of bowel injury location may be greater than 100% because of multiple locations of injury for a single patient.
Other intra-abdominal co-injuries that necessitated surgical intervention
Statistically significant differences are shown in
IAI = intra-abdominal infection; GCS = Glasgow Coma Scale; SD = standard deviation; ISS = Injury Severity Score; AIS = Abbreviated Injury Scale; MVC = motor vehicle collision; GSW = Gunshot wound.
Patients with FIAIs had a significantly higher TAC rate when compared with those with BIAIs (75% vs. 51%, p = 0.014). Between the two groups, no significant differences were found in the duration of OA, type of abdominal wall closure, the use of abdominal packing or drains at the initial operation, or the number of abdominal re-operations (Table 3). No significant differences between FIAIs and BIAIs were found in the number of antibiotic agents used, TPN usage, or ICU admissions.
Relationship between Post-Operative Fungal Intra-Abdominal Infection and Operative Related Variables
Number of abdominal re-operation (laparotomies) performed before definite abdominal closure.
Statistically significant differences are shown in
IAI = intra-abdominal infection; TAC = temporary abdominal closure; SD = standard deviation.
A significant difference was found in the incidence of enteric leak 48 h after initial operation between the FIAI and BIAI cohorts (42.5% vs. 23.1%, p = 0.04). Included in the patients in whom enteric leaks developed were those having anastomotic leaks or slowly evolving injuries with eventual necrosis. Of the patients identified with enteric leaks, 15.6% had gastric leaks, 53.1% had small bowel leaks, 31.3% had large bowel leaks, and 3.13% had rectal leaks. There was no significant difference in the incidence of biloma or urinoma between the FIAI and BIAI groups (37.5% vs. 21.5%, p = 0.08) (Table 4). On multi-variable logistic regression with the forward method, TAC (odds ratio [OR] 6.16, conidence interval [CI] 1.14–28.0, p = 0.02) and the presence of post-operative enteric leak (OR 4.23, CI 1.09–16.4, p = 0.04) were independent risk factors for the development of post-operative FIAIs (Table 5).
Relationship between Post-Operative Fungal Intra-Abdominal Infection and Post-Operative Variables
Statistically significant differences are shown in
IAI = intra-abdominal infection; SD = standard deviation; TPN = total parenteral nutrition; ICU = intensive care unit.
Multi-Variable Logistic Regression for Risk Factors Associated with Post-Operative Fungal Intra-Abdominal Infection
The last step model of logistic regression with forward method.
Statistically significant differences are shown in
CI = confidence interval; TAC = temporary abdominal closure; AIS = abbreviated injury scale; IAI = intra-abdominal infection/
Patients with FIAIs had significantly longer hospital LOS (34.2 ± 23.0 vs. 24.7 ± 17.6, p = 0.02), ICU LOS (16.7 ± 14.7 vs. 9.5 ± 11.3, p < 0.01), and ventilator days (7.96 ± 9.8 vs. 3.92 ± 6.65, p = 0.02) when compared with patients with BIAIs. There was a non-statistically significant increase in all-cause death between FIAIs and BIAIs (10% vs. 1.5%, p = 0.068) (Table 6).
Outcomes of Patients with Post-Operative Intra-Abdominal Infection
Statistically significant differences are shown in
IAI = intra-abdominal infection; LOS = length of stay; SD = standard deviation; ICU = intensive care unit,
We also investigated the relationship of various anti-fungal regimens and clinical outcomes within the FIAI cohort. On the basis of the anti-fungal agent used, patients with FIAI were separated into four groups: Fluconazole alone (40%), micafungin alone (27.5%), anidulafungin alone (7.5%), and multiple anti-fungal agents (25%). There were no significant differences between these groups in all-cause death, hospital LOS, and ventilator days.
Patients who received fluconazole had a significantly lower ICU LOS when compared witth the other three groups (p = 0.03) (Supplementary Table 5). After multi-variable logistic regression adjusting for ISS, however, location of bowel injury, other intra-abdominal co-injuries (liver and spleen), and TAC, there were no longer any significant differences in ICU LOS among patients treated with different anti-fungal agents (Supplementary Table 6).
Discussion
Previous studies have shown that maintaining an OA is associated with fungal contamination [14]. Occhionorelli et al. [15] also investigated OA techniques, such as TAC, and found that longer OA maintenance was associated with an increased risk of development of Candida species infections. This study, however, focused only on ICU post-operative patients [15].
Our findings expand on these previous studies by establishing TAC as an independent risk factor for acquiring post-operative FIAIs. The increased risk of FIAIs with TAC is likely because of the prevalence of fungal species in the external environment and the susceptibility of fungal contamination of the open surgical site on removal of epithelial barriers. This is further complicated by the immunocompromised status of critically ill trauma patients, which increases the risk for development of FIAIs from fungal contamination by environmental sources in the post-operative period.
We also found that patients who presented with liver or splenic injuries that necessitated operative intervention with bowel co-injury had increased association with FIAIs. The etiology of this association is unclear; however, liver and splenic injuries were not statistically shown by logistic regression to be independent predictors for FIAIs. Instead, the association is likely because of the severity of initial injury.
Interestingly, our study did not identify administration of TPN and initial traumatic gastric perforation as significant risk factors for the occurrence of FIAI. Previous studies have shown a significant correlation with TPN administration and the development of fungal infections, believed to be beause of atrophy of intestinal villi, which allows local invasion of enteric Candida [16] and facilitates Candida growth because of TPN-induced hyperglycemia [17]. Manolakaki et al. [18] showed that TPN administration was associated with increased risk of the development of Candida infection in the trauma population.
Our findings did show an increased rate of FIAIs with administration of TPN; however, the increase was not statistically significant. The discrepancy between our findings and the significant findings of previous studies is likely because of the low number of patients receiving TPN (7.6%) in our study. An increased sample size would likely reveal a statistically significant association of TPN administration with the development of FIAIs.
It has been long understood that perforation of the gastric viscera results in increased exposure of the abdominal cavity to enteric contents and is associated with Candida infection [19–22]. A previous study by Horn et al. demonstrated that 51.7% of cultures obtained in surgical patients with perforated peptic ulcers were positive for fungal species [23]. Interestingly, our data show no statistically significant increase in the risk of development of FIAIs with initial traumatic gastric perforation. All patients who presented with gastric perforation in our study were victims of penetrating abdominal injury. We suggest that the discrepancy between our findings and previous studies is because of the close temporal relationship between inciting injury and operative intervention in trauma patients, and that these initial gastric perforations were resolved quickly and did not allow for significant exposure to enteric fungi.
Although initial traumatic bowel perforation was not associated with FIAI, our study found post-operative enteric leaks at >48 h from initial operation to be an independent risk factor for the development of FIAI. This difference is likely because of more prolonged exposure to enteric fungal species in post-operative enteric leaks compared with initial traumatic perforation, which is similar to the mechanism of FIAI development in subacute or chronic conditions such as perforated peptic ulcer disease.
In addition, we found that patients with FIAIs on average had 10 day longer hospital admissions, were admitted to the ICU for an additional eight days, and required four additional days on mechanical ventilation, consistent with previous studies investigating fungal infections [1,18]. The overall mortality rate of 4.8% was similar to that of previous studies investigating IAI [5.13].
While not statistically significant, there was a five-fold higher mortality rate in patients with FIAI compared with patients with BIAI. There was also a difference in the causes of death between the BIAI and FIAI cohorts. The cause of death of the patient in the BIAI group was respiratory failure and unrelated to IAI. Of the patients who died in the FIAI group, 50% died of septic shock from uncontrolled IAIs, and the remainder died of respiratory failure. With the trend of increased death with FIAIs, in addition to the increased incidence of FIAI-related sepsis as a cause of death in our study, we would expect to find significantly higher mortality rates associated with FIAIs compared with BIAIs with increased sample size.
Because FIAI was associated with worse clinical outcomes, we investigated the effect of different anti-fungal treatment regimens on patient outcomes within the FIAI cohort. Initial uni-variable analysis showed a significantly decreased ICU LOS in the fluconazole monotherapy group. This result differed from our expectation because broad anti-fungal regimens should have better coverage and result in improved outcomes.
This is likely explained by the effect of patient clinical severity on outcomes in addition to physician-dependent empirical selection of anti-fungal agents. Because fluconazole was favored for empirical monotherapy of Candida infection, patients with less severe presentations would likely have received fluconazole and also would be expected to have faster clinical improvement. This was supported by multi-variable regression controlling for injury-related variables that showed no significant differences in outcomes among different types of anti-fungal therapies.
Our study had several limitations. Notably, this was a single-center retrospective study, which may limit the applicability of our findings, especially with the variability in clinical outcomes from fungal and bacterial infection. Because it was a retrospective study, we were unable to control for the anti-fungal therapies provided. In addition, the diagnosis and decision to initiate anti-fungal therapy was made independently by the clinician at the time of treatment.
Conclusions
This study found that post-operative IAIs developed in 6.2% of trauma patients; FIAIs developed in 2.4% of the same population. The TAC was identified as an independent risk factor for FIAIs, and patients with FIAIs had significantly longer hospitalizations, ICU LOS, and duration of mechanical ventilation. Clinicians should have a high index of suspicion for fungal infections in post-operative trauma patients with TAC in whom IAIs develop. Future multi-center studies may evaluate further the association between TAC and FIAIs and the possible role of prophylactic anti-fungal therapy in these patients.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.