
Abstract
Background:
In more than 10% of emergency laparotomies in non-trauma patients, primary fascial closure is not achievable because of excessive visceral edema, which leaves the patient with an open abdomen (OA). An OA harbors an inherent high risk of serious complications, and temporary closure devices are used to achieve delayed fascial closure. A potential new strategy in preventing OA is immediate closure during the emergency procedure with a non-crosslinked biologic mesh.
Methods:
This is a prospective comparative cohort feasibility study in 13 teaching hospitals in the Netherlands. Non-trauma patients who underwent emergency laparotomy in which regular sutured primary fascial closure was not achievable because of excessive intra-abdominal edema were eligible. In one cohort, Biomesh (n = 20), the abdominal cavity was immediately closed at the emergency laparotomy with a non-crosslinked biologic mesh. In a parallel cohort, Control (n = 20), the resulting OA was managed by temporary abdominal closure (TAC; inlay polyglactin [Vicryl™] mesh [n = 7]) or commercial (ABTheraTM) abdominal negative pressure therapy device (n = 13)). The primary end point was the proportion of closed abdominal cavities at 90 days.
Results:
At 90 days, 65% (13/20) of the abdominal cavities were closed in the Biomesh cohort versus 45% (9/20) in Controls (p = 0.204). In the Biomesh cohort, seven of 20 (35%) patients had at least one major complication versus 15 of 20 (75%) patients in the Control cohort (p = 0.011). Both the median number of intensive care unit (ICU) and mechanical ventilation days were significantly lower in the Biomesh cohort; one versus 10 (p = 0.002) and 0 versus four (p = 0.003) days, respectively. The number of abdominal reoperations was significantly lower in the Biomesh cohort (median 0 vs. two, p < 0.001; total number five vs. 44).
Conclusions:
If primary fascial closure cannot be achieved at the emergency laparotomy in non-trauma patients, immediate abdominal closure by use of a non-crosslinked biologic mesh prevents OA management. This results in a non-significant higher proportion of closed abdominal cavities at 90 days compared with OA management with TAC techniques, and in a significant reduction of major complications and reoperations, and a shorter ICU stay.
In at least 10
Several temporary abdominal closure (TAC) techniques have been described to avoid evisceration and damage to the abdominal content and to increase chances of delayed closure, such as abdominal negative pressure therapy (NPT), inlay synthetic mesh, Bogota bag, or dynamic retention sutures. Currently, in Europe, abdominal NPT (with or without mesh-mediated traction) and an absorbable inlay synthetic mesh that covers the abdominal wall defect, are the two most commonly used TAC techniques. Abdominal NPT, however, necessitates several reinterventions, and still a fascial defect remains frequently [2].
Absorbable inlay synthetic mesh inevitably ends in a large incisional hernia and has been referred to as “planned ventral hernia strategy” for this reason. Full healing of the skin defect by scar tissue over the abdominal defect might take months and may need skin grafting. These large incisional hernias impair abdominal wall function and often require additional reconstructive surgical procedures.
A potential and new strategy for abdominal closure during emergency laparotomy to prevent OA is the use of an intra-peritoneal non-crosslinked biologic mesh (also termed “intra-peritoneal onlay mesh” [IPOM] biomesh), which can be implanted with and without (i.e., bridging) approximation of the midline fascia. Several studies on the use of a biologic mesh in the elective hernia repair setting have been published [5–12], but studies in the acute setting are lacking.
A biologic mesh in the intra-peritoneal position has several potential advantages in the emergency setting in which primary facial closure cannot be achieved. The mesh can seal off the abdominal cavity (i.e., immediate closure), thereby avoiding the need for additional closure procedures in critically ill patients as is needed in most other TAC techniques. Further, a “planned ventral hernia strategy” is avoided.
Another important advantage is that, because of the initial strength of the non-crosslinked biologic mesh and the transfascial fixation, high fascial medializing traction is possible, increasing the chances of primary fascial closure at the initial emergency procedure. Thereby, approximation of the midline fascia may be achieved in situations in which this normally would not be possible without rupture. Using biologic mesh can therefore prevent an OA and its related short-term and long-term complications. Although costs of a biologic mesh during initial hospital treatment seem high, successful and immediate closure is likely to prevent even higher costs because of complications and reinterventions.
Here, we report the short-term results (90-day follow-up) of the CLOSE-UP feasibility study evaluating effectiveness of immediate abdominal closure in patients undergoing non-trauma emergency operation with excessive visceral edema, in which normal sutured primary fascial closure was not achievable.
Methods
This study was designed as a feasibility study to evaluate the use of a non-crosslinked biologic mesh in the acute setting. A prospective comparative cohort study was performed. All Medical Research Ethics Committees of the participating centers approved this study. The study protocol is included as Supplementary Study Summary.
Non-trauma adult patients requiring emergency abdominal surgery were included in 13 hospitals (one academic and 12 teaching hospitals) in the Netherlands between May 1, 2014, and September 30, 2017. Patients were eligible if they fulfilled one of the following conditions: (1) Midline laparotomy for abdominal infection or peritonitis, intestinal ischemia, or abdominal compartment syndrome (ACS), and regular sutured primary fascial closure was not deemed achievable by the surgeon at the end of the procedure despite adequate pharmacologic muscle relaxation; (2) burst abdomen within seven days after emergency midline laparotomy with contamination (and primary fascial closure during initial operation). If the fascial dehiscence could be closed primarily without special interventions, patients were not eligible.
Informed consent was obtained after the initial procedure, because the need to obtain informed consent before initial operation was waived by the Medical Research Ethics Committee of Amsterdam University Medical Centers. This article reports results according to the STROBE guidelines.
All patients were treated by the relaparotomy-on-demand strategy, which is the preferred strategy based on available evidence [1], and not by planned relaparotomy. Patients in whom source control during operation was not possible and a relaparotomy was scheduled, for example, for secondary source control or delayed anastomosis after ischemia were excluded. Patients with acute necrotizing pancreatitis, peritonitis from bowel perforation after endoscopy operated within 24 h after perforation, and patients with abdominal infection/sepsis because of a continuous ambulatory peritoneal dialysis catheter were excluded.
Further, patients with a life expectancy of less than six months or with liver cirrhosis Child-Pugh class B or class C were excluded. Patients who died within 90 days of initial operation were excluded from analysis because informed consent to use their data had not been obtained and they were not available for CT-scanning to assess abdominal closure end point at 90 days.
Cohorts
The study was initiated in centers with experience in elective hernia operations using a non-crosslinked biologic mesh to ensure the right technique was chosen, because the use of non-crosslinked biologic mesh in elective or acute setting is not widespread yet. These centers (the academic hospital and seven teaching hospitals) included patients in the intervention cohort, the Biomesh cohort. Four of these seven teaching hospitals also included patients from the Control cohort. Patients from the Control cohort were included by nine teaching hospitals of which five hospitals had no experience using a non-crosslinked biologic mesh.
Which treatment patients received (intervention or one of the two control treatments) was based solely on the preference of the surgeon. Twenty patients were included for each cohort for final analysis, based on the ability to assess an estimated primary outcome difference of 40% and a dropout of 30% because of withdrawal of informed consent or non-device–related death.
In the Biomesh cohort, the abdominal cavity was closed using an intra-peritoneal non-crosslinked biologic mesh (Strattice,TM LifeCell/Allergan, Bridgewater, NJ). The biologic mesh was, where possible, used as a leverage to pull close the midline by parachuting transfascial sutures, which put the shear stress on the biologic mesh and not on the midline fascia. In patients in whom this was not possible, the biologic mesh was used as a bridging repair (Fig. 1). The VAC® (KCI, San Antanio, TX) wound dressing system was allowed for management of the post-operative surgical site in case of exposed bridging Strattice biomesh. Clear protocols were followed to keep the exposed bridging Strattice protected (with a non-occlusive/non-adherent barrier) and wet.

Techniques of non-crosslinked biologic mesh use. The StratticeTM biologic mesh could be used as a leverage to pull closed the midline by parachuting transfascial sutures that put the shear stress on the biologic mesh and not on the midline fascia. Drawings by Pieter Zwanenburg, PhD fellow, Amsterdam UMC. Color image is available online.
In the Control cohort, the OA was managed according to current surgical practice techniques of TAC; either by covering the abdominal content with an inlay absorbable synthetic mesh (planned ventral hernia), with or without the abdominal VAC (KCI) wound dressing system for management of the post-operative surgical site, or by abdominal NPT with ABThera™ (Acelity/KCI) [13], depending on the preference of the surgeon, experience, and local protocol. The procedure at which a patient is included in the study is termed “initial emergency laparotomy.” To avoid too much heterogeneity, but to reflect current practice, we only accepted these two TAC practices as controls. Further surgical technical details are included as Supplementary Study Summary.
Outcomes
The primary end point was the proportion of closed abdominal cavities at initial emergency laparotomy, after the initial active treatment period, and after 90 days. Secondary end points were the occurrence of one or more of the major complications (as shown in Supplementary Table S1) within 90 days of study inclusion, hospital stay after study inclusion (days), ICU stay after inclusion (days), duration of mechanical ventilation after inclusion (days), and the number of abdominal reoperations and abdominal radiologic interventions. Other secondary end points, such as incisional hernia and quality of life, as well as cost-effectiveness will be reported after adequate follow-up.
Blinded outcome assessment of the proportion of closed abdominal cavities at 90 days after initial operation, compared for Biomesh and Control groups, was performed. An adjudication committee consisting of two experienced complex abdominal wall surgeons (JW, CV) and an experienced radiologist (PL) of a non-participating specialized abdominal wall center, blinded for treatment assignment, reported closure or non-closure based on the combination of a report of standardized physical examination by an independent assessor, photographs of the abdomen (frontal and lateral views), and an intravenous contrast-enhanced computed tomography (CT).
The definition of a closed abdominal cavity was complete seal of the abdominal cavity with a 100% intact layer (fascia or mesh) by way of full midline approximation or a bridging repair, the absence of abnormal protrusion of the contents of the abdominal cavity or pre-peritoneal fat. [14]
Statistical analysis
Statistical analyses were performed with SPSS, Version 23.0, released in 2012 (IBM Corporation, Armonk, NY). Descriptive statistics were performed to determine frequencies and percentages. The mean was used in data with a normal distribution, and the median was used in data that did not have a normal distribution. All analyses were performed according to the intention-to-treat principle. The occurrences of end points were compared between the two treatment groups. Continuity-corrected chi-square statistic or the Fisher exact test was used where appropriate. Differences in other outcomes were assessed with the Mann–Whitney test.
Results
Patients
A total of 53 patients were included between May 1, 2014 and September 30, 2017, to obtain the required number of 40 patients surviving at least 90 days for follow-up of the primary end point (Fig. 2). In 13 patients, we did not obtain definite informed consent. In 10 patients (18.9% of the total eligible cohort) because of death before the primary end point (at 90 days). In three patients because they were not willing to participate. Among the 40 patients, 20 patients in the Biomesh cohort and 20 patients in the Control cohort were included in the analyses.
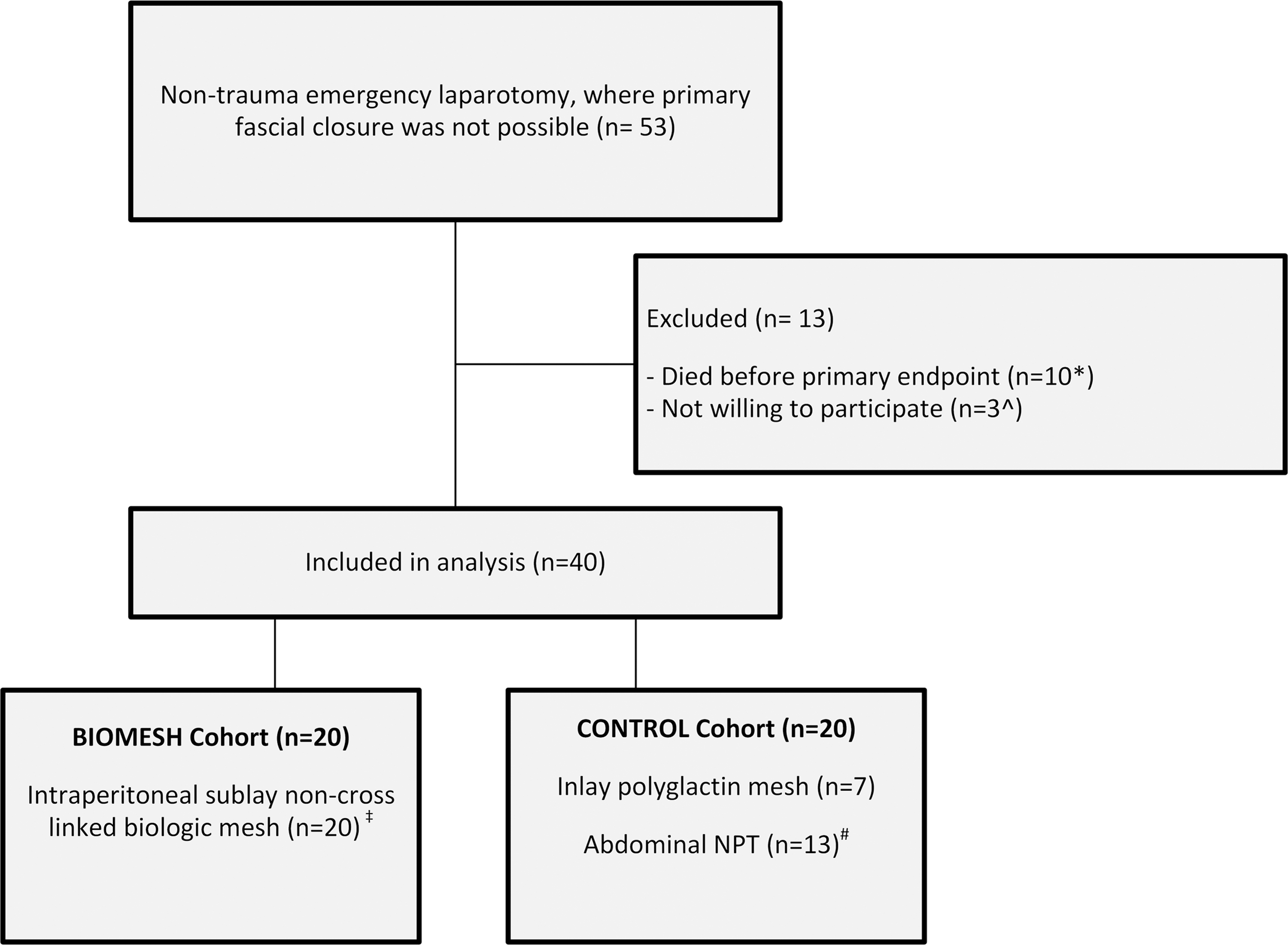
Flowchart of inclusion. NPT = negative pressure therapy. *Four patients with Strattice,™ four patients with ABThera,™ and two patients with polyglactin mesh; ^One patient with Strattice,™ one patient with ABThera,™ and one patient with polyglactin mesh; ‡all Strattice™ non-crosslinked acellular dermal matrix (biologic mesh); #all Abthera™ Negative Pressure Therapy (NPT).
Baseline characteristics
The median age was 61.5 years (range 38 to 83 years), and 65% were male patients. Table 1 summarizes all baseline characteristics.
Baseline Characteristics
IQR = interquartile range; BMI = body mass index; ASA = American Society of Anesthesiologists.
Operative characteristics and abdominal cavity management
The indications for emergency laparotomy, operative characteristics, and details on initial abdominal cavity management are shown in Table 2. Overall indications for first laparotomy, being either index laparotomy preceding emergency operation for complications or initial emergency laparotomy, are supplied in Supplementary Table S2.
Operative Characteristics
ACS = abdominal compartment sydrome; IQR = interquartile range; NPT = negative pressure therapy; NPWT = negative pressure wound therapy; N/A = not applicable
The size of the fascial defects that failed primary closure was comparable for the Biomesh and the Control cohorts. In the Biomesh cohort, immediate closure of the abdominal cavity was achieved in 20 of 20 (100%) patients during initial emergency laparotomy using biologic mesh either as reinforcement of full midline fascial approximation (11 of 20) or as a bridging closure (nine of 20), whereas none of the Control patients had immediate abdominal cavity closure. Instead, the Control group had OA management with some form of TAC.
In six of 20 patients of the Biomesh cohort, no skin closure was possible, and additional standard negative pressure wound therapy (NPWT) (no ABThera) was applied on top of the biologic mesh. In the Control cohort, 13 of 20 patients were treated with abdominal NPT using ABThera and another seven of 20 patients with an inlay polyglactin (Vicryl®) mesh, of whom one patient had standard NPWT on top of the inlay polyglactin mesh.
Actual applied negative pressure in the patients treated with ABThera had varied between 75 and 125 mm Hg. The ABThera dressings were changed up to four times before the last attempt to fascial closure. During the initial active treatment period in the Control group, nine of 13 patients treated with ABThera ultimately had a closed fascia in midline after a median of 10 days (interquartile range [IQR] 6.5–13.5). In three of 13 ABThera patients, a mesh was used (one polyglactin), one polypropylene, and one double polyglactin/polypropylene (Vypro®)) as reinforcement or to bridge at the final step to close the abdomen. One other patient had a frozen abdomen that was left open with drains.
Abdominal cavity closure and post-operative morbidity during the first 90 days
The proportion of closed abdominal cavity at 90 days was non-significantly higher in the Biomesh cohort compared with the Control cohort (13/20 [65%]) versus 9/20 (45%), p = 0.204) (Table 3). Of the 13 patients with a closed abdomen in the Biomesh cohort, five had a bridging repair. Patients in the Biomesh cohort has significantly less major complications within 90 days: Seven of 20 (35%) in the Biomesh group versus (15 of 20 [75%]) in the Control cohort experienced the composite primary end point of major complication (p = 0.011).
Post-Operative Outcomes (within 90 Days after Study Inclusion)
IQR = interquartile range; ICU = intensive care unit.
The median number of days in the ICU as well as the median number of days on mechanical ventilation was significantly lower in the Biomesh cohort than in the Control cohort: One versus 10 days (p = 0.002) and 0 versus four days (p = 0.003), respectively. Five (25%) patients in the Biomesh cohort needed a total of five reoperations compared with 15 (75%) patients in the Control cohort who underwent a total of 44 reoperations (mostly for ABThera changes). The median number of abdominal reoperations in the operating theater was significantly lower in the Biomesh cohort compared with the Control cohort (0 vs. two; p < 0.001).
The number of radiologic abscess drainages was non-significantly higher in the Biomesh cohort. When combining abdominal reoperations and radiologic interventions, 55% of the patients in the Biomesh cohort and 80% of the Control cohort needed an abdominal reintervention (p = 0.091).
In one patient, the biologic mesh was found partly dissolved during relaparotomy for fascial dehiscence, probably because of prolonged severe intra-abdominal infection. A new Strattice was inserted with subsequent healing. In one patient in the Biomesh group, an enterocutaneous fistula developed compared with two patients in the Control group. On investigation of the patient with biologic mesh in whom a fistula developed, we found that the standard NPW therapy was applied directly onto the biologic mesh without using Mepitel® or Adaptic® as an interface according to study protocol.
Discussion
In this feasibility study, we describe a new technique to prevent OA management in non-trauma emergency patients in whom primary fascial closure is not deemed achievable because of visceral edema. By immediate closure of the abdominal cavity at the initial emergency procedure with a non-crosslinked biologic mesh, as reinforcement or bridging, OA management as well as a planned ventral hernia were prevented. A non-significant higher proportion of closed abdominal cavities was reached at 90 days post-operatively with the use of a non-crosslinked biologic mesh (65% vs. 45%, p = 0.204). Post-operative major complications (p = 0.011), reoperations, and number of ICU and ventilation days were significantly reduced compared with OA management with TAC practice. Long-term results such as incisional hernia rates, quality of life, and cost-effectiveness have to be awaited, however.
In the present series of non-trauma emergency operation patients, a mortality rate of 18.9% was found, which is comparable with that in the literature [3]. Recent literature on the management of OA revealed that early closure has significantly lower deaths and post-operative complications in non-trauma patients in comparison with delayed closure [15]. Smith et al. found that by delaying closure for eight or more days, the risk of death within a 90-day follow-up is twice as high [16]. With present technique using a non-crosslinked biologic mesh, a 100% immediate closure of the abdominal cavity was achieved at the initial emergency procedure and as such the need for OA management with TAC devices was prevented.
We found that a median of 10 days (IQR 6.5–13.5) and up to four dressing changes were needed for the ABThera management of OA in the Control cohort before abdominal cavity closure was achieved or no longer plausible. Delayed closure seems to lead to high morbidity as reflected by more abdominal reoperations and longer mechanical ventilation, ICU stay, and overall hospital stay. Of patients in the Biomesh cohort, in whom normal sutured primary fascial closure was deemed impossible because of visceral edema, even 55% had full midline fascial approximation by making use of the strength of the biologic mesh. This strength enables high fascial traction and works as a leverage for closure with transfacial parachuting sutures, thereby directly preserving abdominal wall integrity in an abdomen in which this could otherwise not be achieved in this setting.
This article focuses on short-term outcomes with biomesh-assisted immediate primary closure as the main goal, to reduce the short-term risks associated with an OA. Previous studies on biologic mesh in the contaminated setting show poor results regarding hernia recurrence with hernia rates approximately 30% [17]. In the Biomesh cohort, 65% (13/20) abdominal cavities were still closed at 90 days post-operatively compared with 45% (9/20) in the Control cohort. Although this was a non-significant result (p = 0.204), it does show a trend in favor of the use of biologic mesh.
Because there is a difference between assessing the abdominal wall on CT-scan as the gold standard compared with clinical investigation, the actual hernia recurrence in the literature will be higher [18]. During long-term follow-up, it has to be seen whether this will result in symptomatic hernias and subsequently additional surgical procedures [18]. The percentage of non-closed abdominal cavities, however, seems to be in line with the current literature. Of the seven of 20 non-successful closed cavities in the Biomesh cohort, four had a bridging technique in closing the abdominal cavity. As such, of the patients who had a bridging technique, only 44% had a non-successful closed abdominal cavity at 90 days. This is lower than hernia recurrences reported in the literature when using biologic meshes in which recurrences of up to 80% were noticed [19–21].
A recent review article of Kockerling et al. [22] does not support the use of biologic or biosynthetic mesh in OA. Looking more into detail, however, all studies on management of the OA with a biologic mesh, as discussed in this article, had a different strategy. Most of them used a period of abdominal NPWT in which the septic situation was managed before applying the biologic mesh for delayed closure (i.e., staged approach), and therefore results are not comparable to the present study.
A possible explanation for the (non-significant) primary end point could be that the use of abdominal NPT with ABThera in the Control cohort was higher during the trial than originally expected. At the design of the trial (2012), in common practice the ratio of Vicryl:ABThera was 3:1, whereas during the trial, this ratio was about 1:2. The use of ABThera resulted in a 69% (nine of 13 patients) primary fascial closure after abdominal NPT treatment.
In the protocol, this was estimated at 40% based on available literature, whereas the data on ABThera were scarce and consisted of small series with unclear indications for the OA. Later trials with ABThera provided primary fascial closure rates of 69% at 90 days after the initial procedure [23] and 75% at 30 days [24]. Nevertheless, in the study of Kirkpatrick et al. [23], a little more than half (53%) of the included patients had peritonitis, and in the study of Cheatham et al. [24], this was even lower (22%).
Further, NPWT with mesh mediated traction as a dynamic closure method in the management of OA is preferred over static closure methods [25]. Looking at the literature in the management of OA with NPWT with mesh mediated traction shows that this method provides 80%–100% delayed primary fascial closure [26]. The patients in the included studies in this systematic review also included trauma and vascular patients, meaning they probably lacked contamination from intestinal or infectious complications. When these are present, the delayed primary fascial closure rates drop, and risk of intestinal fistulas increases [26].
Reported hernia incidences in patients available for follow-up among the studies ranges from 21% to 54% after 21 to 63 months. Even 66% was reported after one year in a large prospective study [18]. It remains, therefore, of interest to assess hernia incidences during the long-term follow-up of the current study.
After achieving immediate closure of the abdominal cavity with a non-crosslinked biologic mesh, it seems to be possible to manage adequately the formation of intra-abdominal abscesses by percutaneous radiologic reinterventions, without the need for reoperations. This requires close observation of the clinical condition of the patient with CT imaging, however, in case of any suspicion of an infectious problem, with experienced interventional radiologists who can adequately manage all abdominal fluid collections that develop after closure of the abdominal cavity.
With a reduction in major post-operative complications, ICU stay, and mechanical ventilation days, an earlier closure of the abdomen and a higher closure rate using a biologic mesh in the acute setting seems to be an advantage over temporary abdominal closure techniques. High short-term morbidity in critically ill patients, as observed in the Control cohort, harbors a risk of long-term complications. In particular, stay in the ICU and mechanical ventilation have been associated with substantial risk of complications, both physical and mental [27–31].
Therefore, early closure of the abdominal cavity with a biologic mesh, either reinforced or bridged, seems essential to prevent further increase of morbidity related to reoperations, thereby enabling early recovery from septic and unstable metabolic conditions, with prevention of organ failure and other complications. The so-called neofascia that is created with the non-crosslinked biologic mesh closes the abdominal cavity and can serve as a protective layer against the external environment. Moreover, a biologic mesh can usually withstand a contaminated environment and can therefore be implanted in a hostile abdomen [32–34]. As such, it can prevent additional operation as required with most TAC techniques, and it can promote early recovery.
A study [35] performed in Switzerland with synthetic mesh-augmented closure of the OA showed reduced reoperations, reduced duration of ICU stay and hospital stay compared with abdominal NPT while deaths and the incidence of fistula did not differ. Hernia-free survival significantly increased. This study also underlines the benefits of closure of the abdomen as soon as possible compared with TAC. It is difficult to determine whether these patients are comparable to those in the current study in terms of contamination because this is not mentioned in patient characteristics. Moreover, termination of OA after initial treatment was at a median of three days, showing not all OA were closed immediately and only 26% of the fascia was closed compared with 55% in our study because of mesh-mediated traction.
Selection bias is always at risk in non-randomized studies and especially in this heterogeneous population of non-trauma OA patients. We excluded patients who died within 90 days to be able to compare closed abdominal cavities at 90 days. The number of excluded patients was comparable in both groups. Because death is also a major complication, including these patients would have been preferable; however, no informed consent could be achieved as a result of their death because no CT scan could be performed. Therefore, we chose to exclude them. The number of patients with a burst abdomen was slightly higher in the Biomesh cohort. This could have led to some selection bias with fewer severely ill patients in the Biomesh cohort. The defect size was comparable with the Control cohort patients and the level of contamination higher, however.
A major problem encountered during this study was slow patient accrual. Laparoscopy is quickly replacing open surgical procedures in many different medical fields, and in the last few years, abdominal sepsis is also approached laparoscopically more and more. Therefore, the number of non-trauma patients presenting with an OA is limited. Another limitation is the experience with biologic mesh of surgeons participating in the study. Only a few surgeons had experience with a biologic mesh in the elective setting; other surgeons were not prepared nor allowed to use biologic mesh in the acute setting for the first time.
Conclusions
This is the first study to investigate the role of immediate closure of the abdominal cavity with a biologic, non-crosslinked mesh in an acute setting in which OA management is prevented in all patients. Although the initial costs of a biologic mesh might be high, less complications and interventions, a shorter stay in the ICU, and fewer mechanical ventilation days may well compensate for these costs. Although this was not studied formerly, biologic mesh closure in the emergency setting may overall prove to be cost-saving. With a mortality rate of almost 20%, careful patient selection is important, and future studies should focus on this aspect.
Immediate closure of the abdominal cavity with a non-crosslinked biologic mesh in non-trauma patients undergoing emergency midline laparotomy presents significant benefits, based on present short-term results in the acute setting. Long-term outcomes on hernia rates, reconstructive surgery for hernia, and cost-effectiveness need to be awaited.
Footnotes
Acknowledgments
Adjudication committee: JW: J. Warusavitarne, CV: Miss C. Vaizey, and PL: P.F. Lung, St Mark's Hospital, London, United Kingdom.
CLOSE-UP Study Group
Gijs J.D. van Acker, MC Haaglanden, The Hague, the Netherlands; Caroline S. Andeweg, St. Jansdal Hospital, Harderwijk, the Netherlands; Eric J.T. Belt, Albert Schweitzer Hospital, Dordrecht, the Netherlands; Willem A. Bemelman, Academic Medical Center, Amsterdam, the Netherlands; Marcus A.M. Brouwers, Haga Hospital, The Hague, the Netherlands; Esther C.J. Consten, Meander Medical Center, Amersfoort, the Netherlands; Sebastiaan Festen, OLVG, Amsterdam, the Netherlands; N. Tjarda van Heek, Gelderse Vallei Hospital, Ede, the Netherlands; Tom M. Karsten, OLVG, Amsterdam, the Netherlands; Flip M. Kruyt, Gelderse Vallei Hospital, Ede, the Netherlands; Bas Lamme, Albert Schweitzer Hospital, Dordrecht, the Netherlands; Eric R. Manusama, Medical Center Leeeuwarden, the Netherlands; John K. Maring, Elisabeth Tweesteden Hospital, Tilburg, the Netherlands; Willem H. Steup, Haga Hospital, The Hague, the Netherlands; Jan H.M.B. Stoot, Zuyderland Hospital, Sittard, the Netherlands; Pieter J. Tanis, Academic Medical Center, Amsterdam, the Netherlands; Willem F. van Tets, OLVG, Amsterdam, the Netherlands; Tammo S. de Vries-Reilingh, Elkerliek Hospital, Helmond, the Netherlands; Daria K. Wasowicz, Elisabeth Tweesteden Hospital, Tilburg, the Netherlands; Johannes A. Wegdam, Elkerliek Hospital, Helmond, the Netherlands; Marinke Westerterp, MC Haaglanden, The Hague, the Netherlands.
Funding Information
This is an investigator-initiated study. LifeCell contributed to the study with an unrestricted institutional research grant.
Author Disclosure Statement
M.A. Boermeester reports institutional research grants from Baxter, Mylan, Ipsen, Acelity/KCI, Bard, LifeCell and Johnson & Johnson/Ethicon and New Compliance; and is a speaker or advisory board member for Acelity/KCI, Bard, LifeCell/Allergan, Gore, Bard, Smith&Nephew and Johnson & Johnson / Ethicon. For the remaining authors, no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.