
Abstract
Background:
Descending necrotizing mediastinitis [DNM] is a serious complication of odontogenic infections, being associated with a high mortality rate. The diagnosis, classification, and management depend on computed tomography [CT] findings. Incision, drainage, and debridement represent the principal management. This study aimed to assess the prognosis in odontogenic DNM.
Methods:
The DNM type I was managed by transcervical mediastinal drainage, while in DNM type II, a right or left posterolateral thoracotomy was used. Data were compared among survivors and deceased to detect the risk factors affecting the prognosis.
Results:
This study included 63 patients. Transcervical mediastinal drainage was performed in 57 patients with Endo Type I while drainage through a right posterolateral thoracotomy was performed in the other five patients with Endo Type I and one patient with Endo Type IIA. Of patients in the study, 82.5% survived while 17.5% died because of multiple organ failure. Multiple complications and severe sepsis or septic shock as risk factors were statistically significant.
Conclusion:
A CT scan is the modality of choice for diagnosis and classification of DNM. Incision and drainage of the maxillofacial infection with mediastinal drainage and debridement represent the main management. Multiple complications and severe sepsis or septic shock were associated with poor prognosis.
Descending necrotizing mediastinitis [DNM] is one of the serious and life-threatening complications of cervicofacial infections [1]. Approximately 60%– 70% of the cases of DNM occur secondary to odontogenic infections, particularly if there is involvement of the second or third mandibular molars [2,3]. The extraction of impacted third molars and implant surgical procedures has gradually raised the incidence of DNM [4,5]. Descending necrotizing mediastinitis has an aggressive course and may be complicated by sepsis, pyothorax, peri-carditis, multiple organ failure, and death.
The mortality rate was higher than 50% before the antibiotic era [6]. Later, although a wide range of antibiotic agents is available, DNM is still associated with a high mortality rate (approximately 11%–40%) mainly because of delayed diagnosis and inappropriate surgical management [2,7,8].
Early diagnosis and treatment are very important to decrease morbidity. History and physical examination provide high suspicion. Any patient with oropharyngeal or odontogenic infection with neck swelling or pain possibly from DNM should have computed tomography (CT) of the neck and chest to evaluate the spread of infection. The CT scanning immediately confirms mediastinitis with high accuracy and also helps in treatment planning [9].
The principal CT findings of odontogenic infection are peri-coronal or peri-apical shadows of the focal tooth and soft tissue abscess with or without gas formation. The CT findings of mediastinitis include localized mediastinal fluid collections or abscesses, pleural or pericardial effusions, gas bubbles in the mediastinal soft tissues, lymphadenopathy, and venous thrombosis. In addition, diffuse mediastinitis may be seen, characterized by increased density of the mediastinal fat with resultant loss of definition of normal fat planes [10–13].
Management of DNM includes intravenous antibiotic agents, airway management, and surgical drainage of the cervical and mediastinal collections in addition to management of the source of infection. The transcervical approach is used for drainage and debridement of infections that are in the anterior superior mediastinum above the carina while the transthoracic approach is used for infections that spread more inferiorly [2,14–16].
The aim of this article was to study the demographics, concomitant diseases, etiologic factors, clinical presentation, management, and outcomes of DNM from odontogenic infections in our centers during the past 10 years to detect the risk factors affecting prognosis.
In addition, we supposed that the existence of multiple concomitant diseases and complications may be associated with a poor prognosis. Also, we expected that a team approach could provide better management and may improve the outcome.
Methods
Study design, setting, and population
This was a retrospective study conducted at Sohag University Hospitals, Sohag, Egypt. It included all patients with DNM secondary to odontogenic infection who presented and were treated between July 2008 and July 2018.
Inclusion criteria
Patients who had clinical manifestations of odontogenic maxillofacial infection, radiologic findings of mediastinitis, proof of DNM surgically, and presence of etiologic relation between an odontogenic infection and the occurrence of DNM were included in the study.
Exclusion criteria
Patients who had DNM without odontogenic infection and those who refused participation in the study or were unable to sign an informed consent were excluded from the study.
Ethical approval
This study was approved by the Institutional Review Board and Ethics Committee (see Supplementary Data: Approval form) and was conducted in accord with the principles of the Declaration of Helsinki (1975) as revised in 2000. All patients agreed to participate in the study and signed a written informed consent (see Supplementary Data: Consent form and Patient photographic release form).
Data collection
The collected data included the demographics of the patients, the clinical data, the treatment, and the outcome. Data were compared among surviving and deceased patients to detect the risk factors affecting the prognosis.
The extent of DNM was categorized according to the Endo classification [17] into Type I (infection above the bifurcation of the trachea), Type IIA (infection extended to the inferior part of the anterior mediastinum), and Type IIB (infection extended to the anterior and the posterior mediastinum).
Statistical analyses
Data from the record of each patient were collected in an Excel spreadsheet, processed using the Statistical Package for the Social Sciences, version 20. The continuous variables were assessed by t-test and were reported as the mean ± standard deviation (SD). The categoric and binary variables were studied using the chi square test or Fisher exact test and reported as percentages. The p values less than 0.05 were considered statistically significant. A bivariable analysis was used to assess all variables collected in this study to find variables with a p value less than 0.05.
Study protocol
Diagnosis and management were performed by a team including maxillofacial surgery, thoracic surgery, radiology, and anesthesia and intensive care. The radiologic diagnosis was performed via panorama x-ray, head and neck CT, and chest CT with contrast (Fig. 1).
For patients with airway obstruction, tracheostomy or endotracheal intubation was performed at first, then drainage and debridement of the neck and chest were performed within 12 h and administration of empiric antibiotic treatment in the form of amoxicillin-clavulanic acid and metronidazole via intravenous injection (Fig. 1). Then, antibiotic agents were modified in accord with the results of the microbiologic investigations.
All patients of DNM Type I (infection above the level of the fourth thoracic vertebra) were treated by transcervical mediastinal drainage through suprasternal fossa incision, applying blunt dissection to communicate the maxillofacial/cervical incisions with the suprasternal fossa incision. After identification of the abscess cavity, the pus was drained, and the necrotic tissues were debrided.
For patients with infections below the level of the fourth thoracic vertebra, a right posterolateral thoracotomy incision was performed to get access to both the anterior and the posterior mediastinum to achieve proper drainage and debridement. If the infection involved only the left mediastinum or the left side of the chest, then a left thoracotomy incision was indicated (Fig. 1).
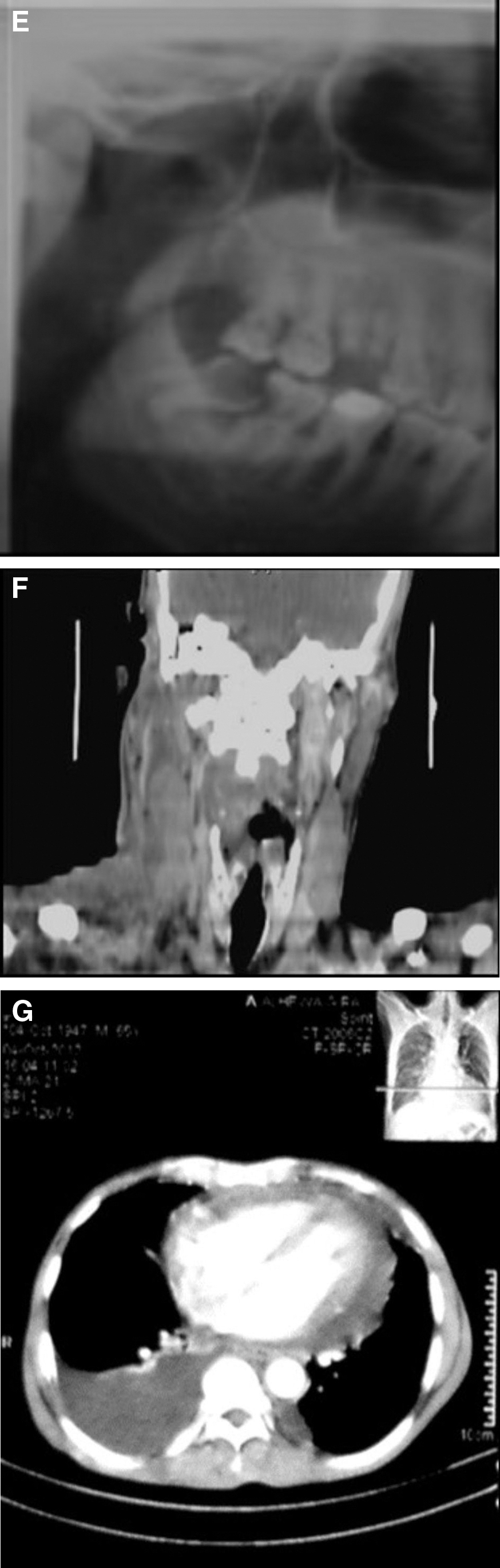
A 47-year-old patient with right-sided cervicofacial infection and right-sided descending necrotizing mediastinitis secondary to peri-apical infection of the right lower third molar was treated by incision drainage and debridement of cervicofacial infection and mediastinitis. (
Results
This study included 63 patients. They were 24 (38.1%) males and 39 (61.9%) females. Their ages ranged between 21–80 years with a mean of 51.7 ± 13.2 years. The mean duration from the appearance of the manifestations of the primary infection to the admission ranged from 5–28 days with a mean of 9.2 ± 4.9 days.
All patients had dental pain, accompanied by swelling in the face and neck and limited mouth opening. In addition, they had fever, dysphagia, dyspnea, and chest pain. Thirty-three (52.4)] patients had concomitant systemic diseases. Seven patients (11.1%) had more than one concomitant disease. Diabetes mellitus was the most common one. It was found in 23 (36.5%) patients (Table 1).
Distribution of Concomitant Diseases
Regarding the etiology of DNM, the most common causes were peri-apical peri-odontitis in 40 (63.5%) and peri-coronitis 20 (31.7%). Other causes were tooth extraction in one (1.6%) patient, an infected peri-apical cyst in another one (1.6%), and an infected dentigerous cyst in a third patient (1.6%). The most common teeth responsible concerning the infection were the lower third molar in 21 (33.3%) patients and the lower second premolar in nine (14.3) patients. Other teeth were less common (Table 2).
Distribution of the Teeth Responsible for the Infection
Head and neck CT showed the infected neck spaces. A total of 294 spaces with a mean of 4.6 ± 3.4 were involved. The most common spaces to be involved were the submandibular space in 54 (85.7%) patients, pterygomandibular space in 45 (71.4%) patients, and submasseteric space in 32 (50.8%) patients. Other spaces were involved less frequently (Table 3).
Distribution of Infected Neck Spaces Based on Head and Neck Computed Tomography
Multiple spaces were involved in the same patient
Chest CT detected localized mediastinal fluid collections with increased attenuation of mediastinal fat in 63 (100%) patients, free gas bubbles in the mediastinum in 57 (90%), enlarged mediastinal lymph nodes in 54 (85.7%), localized and/or free pleural effusions in 52 (82.5%), lung infiltrates in 25 (39.7%), and peri-cardial effusions in 19 (30.1%). Endo Type I was found in 62 (98.4%) patients and Type II A in one (1.6%) patient, while no patient was classified as having Type IIB infection.
The white blood cell (WBC) count at admission ranged between 1.8–32.8*10^9/L with a mean of 14.7 ± 6.1*10^9/L. The neutrophil percentage ranged between 49.9%–96.2% with a mean of 84.8% ± 9.6%. Bacteriologic examinations of the collected drainage were negative in 50 (79.4%) patients and positive in 13 (20.6%) patients. The isolated organisms were Streptococcus spp. in nine patients (14.3%), while Staphylococcus aureus, Pseudomonas aeruginosa, Escherichia coli, and Achromobacter xylosoxidans were isolated each in one patient.
All patients underwent surgical treatment through incision and drainage of infected neck spaces and radical surgical debridement. Transcervical mediastinal drainage through suprasternal fossa incision was performed in 57 (90.5%) patients with Endo Type I. Drainage through a right posterolateral thoracotomy was performed in six (9.5%) patients who were five Endo Type I patients and one Endo Type IIA patient. A tracheotomy was indicated in 15 (23.8%) patients.
Of the 63 patients included in the study, 52 (82.5%) patients survived and 11 (17.5%) patients died because of multiple organ failure. The mean length of hospital stays for the 52 survivors ranged between 8–46 days with a mean of 24.5 ± 16.8 days. Complications were reported in 18 (28.6%) patients. Seven (11.1%) patients had more than one complication. The most common complications were pleural effusion in eight (12.6%) patients and pneumonia in six [9%] patients while other complications were detected at a lower rate (Table 4).
Distribution of Study Subjects Based on Complications
Data analysis was performed to detect death risk factors. Comparing the variables between the survivor and deceased patients revealed that the p values of the existence of multiple complications (0.019) and that of severe sepsis or septic shock (0.004) are less than 0.05, so they were considered statistically significant. This indicated that the existence of multiple complications and severe sepsis or septic shock are risk factors. The p values for other variables were higher than 0.05 and were not statistically significant, so they were not associated with the outcome (Table 5).
P Value for Comparing the Variables between the Survivor and Deceased Patients
Discussion
Descending necrotizing mediastinitis is an acute suppurative infection of the mediastinum. It occurs mainly secondary to either odontogenic or oropharyngeal infection [2]. In our series, odontogenic DNM was more prevalent in males between 40–60 years. In accord with Qu L et al [18], the most common source of the odontogenic DNM was peri-apical peri-odontitis. Most patients had multiple space infections.
The submandibular and the pterygomandibular spaces were the commonly affected spaces in odontogenic DNM. This involvement can be attributed to the presence of the roots of the second and third lower molars below the level of the mylohyoid line. Therefore, a peri-apical abscess can extend easily to the submandibular and the para-pharyngeal spaces [19]. Also, the posterior portion of the submandibular compartment provides a pathway to the sublingual and the para-pharyngeal spaces, and then to the retro-pharyngeal space. This is the main pathway for spread of the infection to the mediastinum [20].
In our study, most of the patients had dental pain, accompanied by swelling in the face and neck and limited mouth opening. Also, they had fever, dysphagia, dyspnea, and chest pain. We think that the diagnosis of DNM is difficult. It is based mainly on clinical presentation and CT radiographic features. It should be anticipated in patients presenting with toothache, trismus, cervicofacial swelling with dysphagia, dyspnea, chest pain, and swelling [21].
In this study, head and neck CT showed the source of infection, the infected neck spaces, and the extent of infection to the mediastinum. In accord with the literature, the CT was found to be reliable in the diagnosis of DNM and also to evaluate the progress and the efficacy of the offered therapy. Further, CT can assist in treatment planning of the optimal surgical approach for drainage and debridement by visualizing the spread of infection in the chest.
In addition, CT is important for monitoring the success of the treatment and the follow-up [13,22]. In accord with many studies [10,23,24], CT findings of increased mediastinal fat attenuation, localized mediastinal fluid collections with or without the presence of gas bubbles were encountered in all patients with DNM. Other CT findings such as peri-cardial effusion, pleural effusion, lung infiltrates, and lymphadenopathy are present in variable percentages with pleural effusion and mediastinal lymphadenopathy being the second most common findings followed by lung infiltrates and peri-cardial effusion.
Descending necrotizing mediastinitis is a poly-microbial condition. Proper antibiotic agents should be provided after the diagnosis to cover both aerobic and anaerobic bacteria [7, 20]. In this series, all patients received broad-spectrum empiric antibiotic agents immediately after admission. In this study, results of bacteriologic examinations of the collected drainage were negative in 50 (79.4%) patients and positive in 13 (20.6%) patients. The isolated organisms were Streptococcus spp. in nine patients (14.3%), while S. aureus, P. aeruginosa, E. coli, and A. xylosoxidans were isolated each in one patient.
The high percentage of negative cultures can be explained by the administration of broad-spectrum antibiotic agents immediately after the admission of the patients. It is reported that few bacterial cultures are positive, and the most common bacterium involved in DNM is Streptococcus. Other bacterial species include S. aureus, P. aeruginosa, and E. coli [18].
Early drainage and debridement are the cornerstone in the management of odontogenic DNM. The Endo protocol for treatment of patients with DNM was applied to our patients [17]. Incision and drainage of infected neck spaces and radical surgical debridement were performed for all patients. A transcervical mediastinal drainage through the suprasternal fossa incision was performed in 57 patients with Endo Type I while drainage through a right posterolateral thoracotomy was performed the other five patients with Endo Type I and one patient with Endo Type IIA. We think that Incision and drainage of infected neck spaces were essential to manage the primary infection and to avoid the spread of infection to the mediastinum.
Guan et al. [25] reported that DNM involving the anterosuperior mediastinum can be managed by transcervical mediastinal drainage. They advocated that an open thoracotomy is a suitable approach if mediastinitis spreads downward. In accord with Deu-Martin et al. [26], we found that right thoracotomy was better than left thoracotomy. It provided better exposure and access to the whole mediastinum, helped to achieve aggressive debridement of the mediastinum, and avoided the aorta, which interferes with the debridement and drainage in left thoracotomy. In agreement with Makeieff et al., [15] we found that the posterolateral thoracotomy approach provided the maximum exposure and access of the ipsilateral mediastinum, the pericardium, the prevertebral space, and para-esophageal planes.
Tracheotomy is necessary for airway management in advanced cases of DNM. In this study, 15 (23.8%) patients with airway obstruction were treated by tracheotomy. In accord with Uwa et al. [27], tracheotomy was performed as a therapeutic measure only in patients with airway obstruction and not as prophylaxis against airway obstruction.
In this study, 52 (82.5%) patients survived and 11 (17.5%) patients died because of multiple organ failure. This high survival rate can be explained by the fact that most of our patients were Endo Type I. We found that septic shock and the existence of multiple complications were associated with poor prognosis, which can be attributed to delayed presentation, late diagnosis, improper antibiotic agents, or inadequate drainage and debridement [26].
It was reported that death from DNM is still high in spite of the use of broad-spectrum antibiotics, the improved surgical procedures, and advanced intensive care facilities [8,28]. In accord with the literature, the mortality rate in our series was 17.5%. The studies reported that the mortality rate ranges from 11% to 40% [8,29,30]. We think that the team approach, early diagnosis, and proper management decrease deaths in patients with odontogenic DNM. Also, association with other comorbidities and the occurrence of complications may increase risks for poor prognosis.
In our study, the non-survivors had a longer hospital stay, late diagnosis, and elevated neutrophil count than survivors. These factors, however, were not significant.
Conclusion
Odontogenic infection is a common cause of DNM. The CT scan is the modality of choice for diagnosis, classification, and management of DNM. Incision and drainage of the cervicofacial infection in addition to mediastinal drainage and debridement represent the main treatment. The existence of multiple complications and severe sepsis or septic shock were associated with poor prognosis.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.