
Abstract
Background:
Intra-cranial bacterial infection is a serious complication in emergency neurosurgical patients, and few data are available on the trends of these infections and the rates of antibacterial drug resistance.
Methods:
We surveyed retrospectively the patients with intra-cranial bacterial infection in our emergency neurosurgical center between January 2009 and December 2018. Demographic characteristics, causative bacteria, and antimicrobial susceptibility test results were collected.
Results:
A total of 100 patients with intra-cranial bacterial infection, 1.41% of our patients, were enrolled. There were 123 strains of bacteria cultured from the cerebrospinal fluid (CSF), consisting of 96 strains of gram-negative (GN) bacteria and 27 strains of gram-positive (GP) bacteria. Compared with the GP bacteria, the percentage of GN bacteria increased to 75.0% of the total near the end of the study. Compared with Acinetobacter baumannii, Klebsiella pneumoniae also showed an uptrend. Most of the bacteria were multi–drug-resistant (MDR). We further analyzed the consistency of CSF and sputum cultures from the same patient. The ratio of Klebsiella pneumoniae and Acinetobacter baumannii to the corresponding strains in the CSF were 77.0% and 62.0%.
Conclusions:
The bacteria recovered from the CSF were mainly GN. The tendency of GN bacteria showed an uptrend, especially for Klebsiella pneumoniae. Furthermore, most of the bacteria were MDR.
Central nervous system (CNS) bacterial infection is one of the most serious complications after neurosurgery, leading to a poor prognosis and prolonged hospitalization [1]. The incidence of such CNS infections ranges from 0.3% to 7.8% [2]. There are some studies reporting the prevalence and risk factors for CNS bacterial infection after neurosurgery [2,3]. However, all of them focused on infection after elective operations. There thus is a lack of data regarding CNS infections after emergency neurosurgery, which is considered a risk factor for CNS infection.
The epidemiology of bacterial infections changes with time. Previously, gram-positive (GP) bacteria predominated in post-operative intra-cranial infections [4–8]. However, reports on gram-negative (GN) bacterial infection in the CNS increased significantly in recent years [3]. More importantly, the rate of multi–drug-resistant (MDR) strains, including those that produce extended-spectrum β-lactamases (ESBLs), have risen quickly, which causing difficult-to-treat ventriculitis/meningitis and higher mortality rates [9].
Because patients having emergency neurosurgery are vulnerable to CNS infection that results in poor outcomes, especial with MDR GN strains, it is crucial to know the prevalence and antibiotic resistance of infecting bacteria to enable prompt and effective empirical therapy.
Patients and Methods
This study was approved by the Ethics Committee of the Evaluation of Biomedical Research Projects of Huashan Hospital. It was a retrospective and non-interventional study, so informed consent was not required.
All patients admitted to the emergency neurosurgical center of Huashan Hospital, a university teaching hospital, from January 2009 to December 2018 were evaluated retrospectively. The neurosurgical center is one of the greatest centers for critical neurosurgical patients in China. Patients whose ages ranged from 18 to 70 years having positive central nervous system (CSF) bacterial cultures were included. Patients with evidence of concomitant chronic meningitis or encephalitis not caused by microbial infection or using immunosuppressive agents or having immunodeficiency syndrome were excluded. The severity of the patients' condition was measured by the Glasgow Coma Scale (GCS). Other data collected were age, gender, diagnosis, incidence of pneumonia, pathogenic organisms identified from the CSF, and antibiotic susceptibility testing. Pathogenic organisms were considered multi-drug resistant (MDR) if they were reported as intermediate or resistant to at least one representative drug in three of the seven categories, namely cephalosporins, fluoroquinolones, aminoglycosides, carbapenems, extended-spectrum penicillin, macrolides, and β-lactam/β-lactamase inhibitors [10].
SPSS 20.0 software (The IBM SPSS Software Company, Armonk, NY USA) was used for statistical analysis. The continuous measurement data in accordance with normal distribution were expressed as mean ± standard deviation (SD). The independent t-test was used for comparison among groups when variance was uneven using the rank sum test. Enumeration data were described by frequency or percentage. P < 0.05 was statistically significant.
Results
Patient characteristics and outcomes
In total, 7,079 consecutive patients were admitted to the emergency neurosurgical center from January 2009 to December 2018. Of these, 100 (1.41%) with CNS bacterial infection were enrolled in this study, including 80 males and 20 females. The type of injury was traumatic brain injury (TBI) (60 patients), intra-cerebral hemorrhage (ICH) (34 patients), subarachnoid hemorrhage (SAH) (three patients), arteriovenous malformation (AVM) (two patients), and cerebral infarction (one patient). The average age and GCS of the patients were 46.22 ± 13.81 and 8.19 ± 3.30, respectively. There were 77 patients who had craniotomy and 23 who underwent intra-cranial pressure (ICP)/Ommaya device implantation. Some 17 (16.87%) patients were infected with two or more bacteria. The demographic and clinical characteristics of the patients are shown in Table 1.
Demographic and Clinical Characteristics of 100 Patients with Central Nervous System Infection
Among the patients, 17 died. Table 2 compares the outcomes of survivors and non-survivors. There are no significant differences in gender (80% male versus 20% female; odds ratio [OR] 1.288 and 95% confidence interval [CI] 0.371–4.481; p = 0.69); age (45.30 ± 14.08 versus 50.71 ± 11.78 years; OR 2.244; 95% CI 0.676–7.445; p = 0.14), GCS (8.42 ± 3.23 versus 7.06 ± 3.47; OR 1.272; 95% CI 0.429–3.771; p = 0.12), type of injury (p = 0.65), or type of operation (p = 0.59) between the groups. Nevertheless, the mortality rate of GN bacterial infection was significantly higher than that of GP bacterial infection in unadjusted (95.2% versus 4.8%; OR 0.146; 95% CI 0.019–1.143; p = 0.04) and adjusted (adjusted OR [aOR] 1.174; 95% CI 0.875–1.575; p = 0.285) models. The data are shown in Table 2.
Demographic and Clinical Characteristics of Survivors vs. Non-Survivors
CI = confidence interval; GCS = Glasgow Coma Scale; GN = gram negative; GP = gram-positive; ICH = intracerebral hemorrhage; OR = odds ratio; TBI = traumatic brain injury.
Strains and tendency of CNS bacterial infection
There were 123 bacteria in CSF cultures, of which 96 (78.1%) strains were GN and 27 (22.0%) GP. There were 30 species bacteria. During the last 10 years, the percentage of GN bacteria increased from 55.6% to 75.0% (Fig. 1). The predominant GP isolate was Staphylococcus epidermidis (6.5%), followed by S. haemolyticus (2.4%). Acinetobacter spp. was the predominant GN organism and was isolated in 44 (35.8%) cases, followed by Klebsiella pneumoniae in 31 (25.2%) and Pseudomonas aeruginosa in 6 (4.9%) (Fig. 2). Thus, GN bacteria were predominant in emergency neurosurgical patients with CNS infection over the last 10 years.
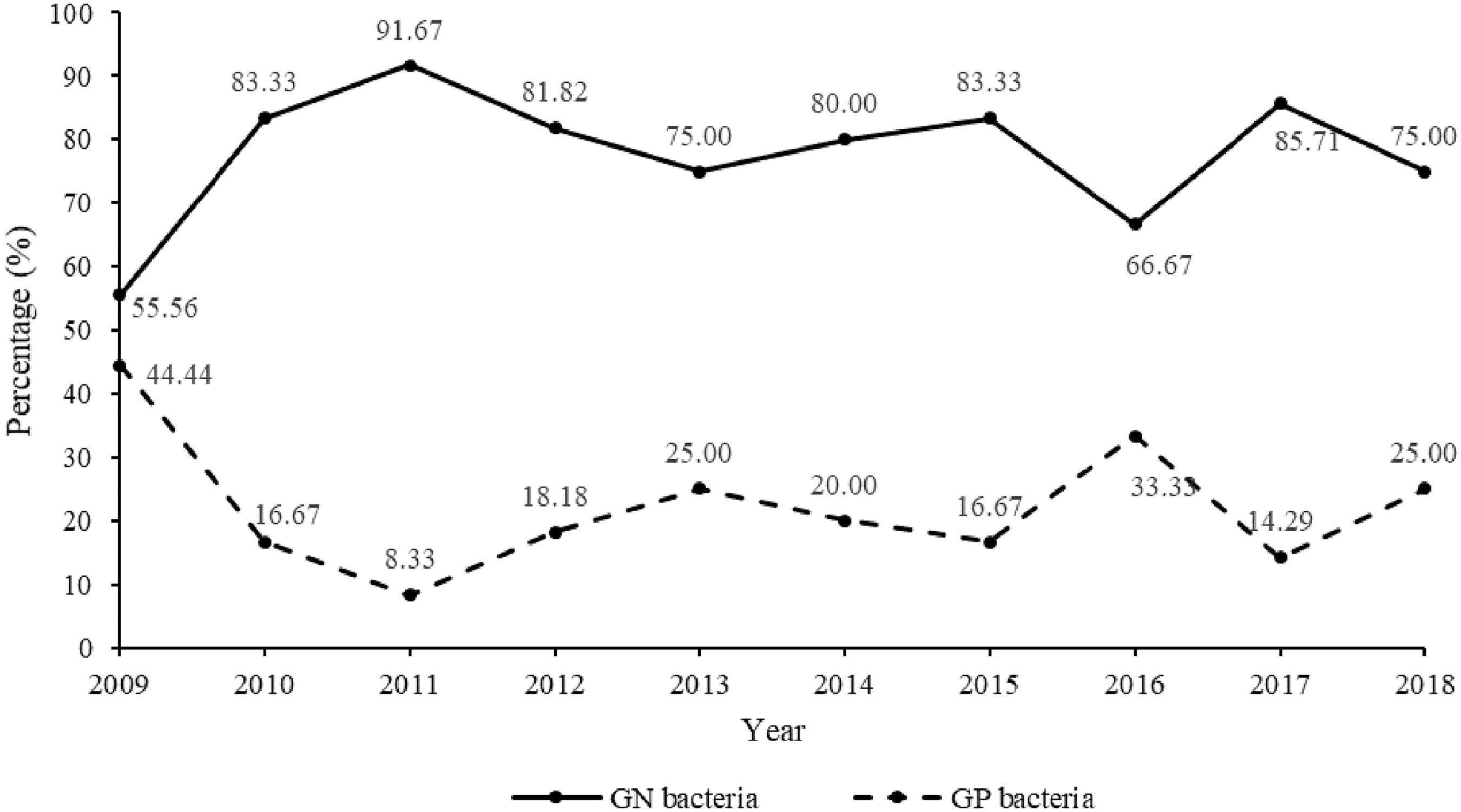
Percentage of gram-negative and gram-positive bacteria from 2009 to 2018.
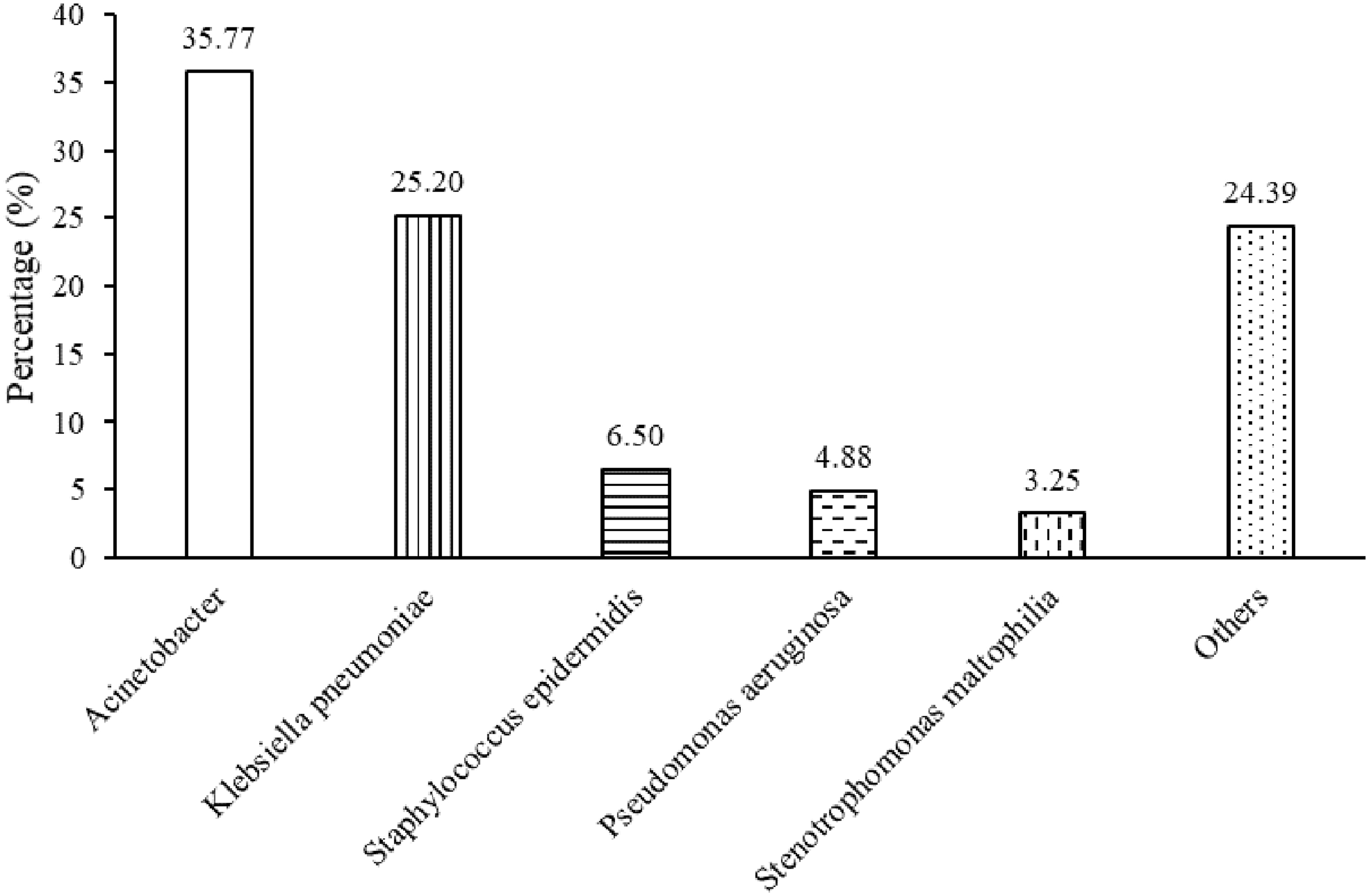
Positive strains in cerebrospinal fluid culture from 2009 to 2018.
All of the dead patients were infected with Acinetobacter baumannii and K. pneumoniae. Because all of these patients were infected with these two organisms, we focused on their preponderance over the last 10 years. The percentage of A. baumannii was relatively stable, ranging from 22.2 to 25.0. However, although the percentage of K. pneumoniae fluctuated below 27.3 from 2009 to 2016, it rose above 40 within the last two years (Fig. 3).
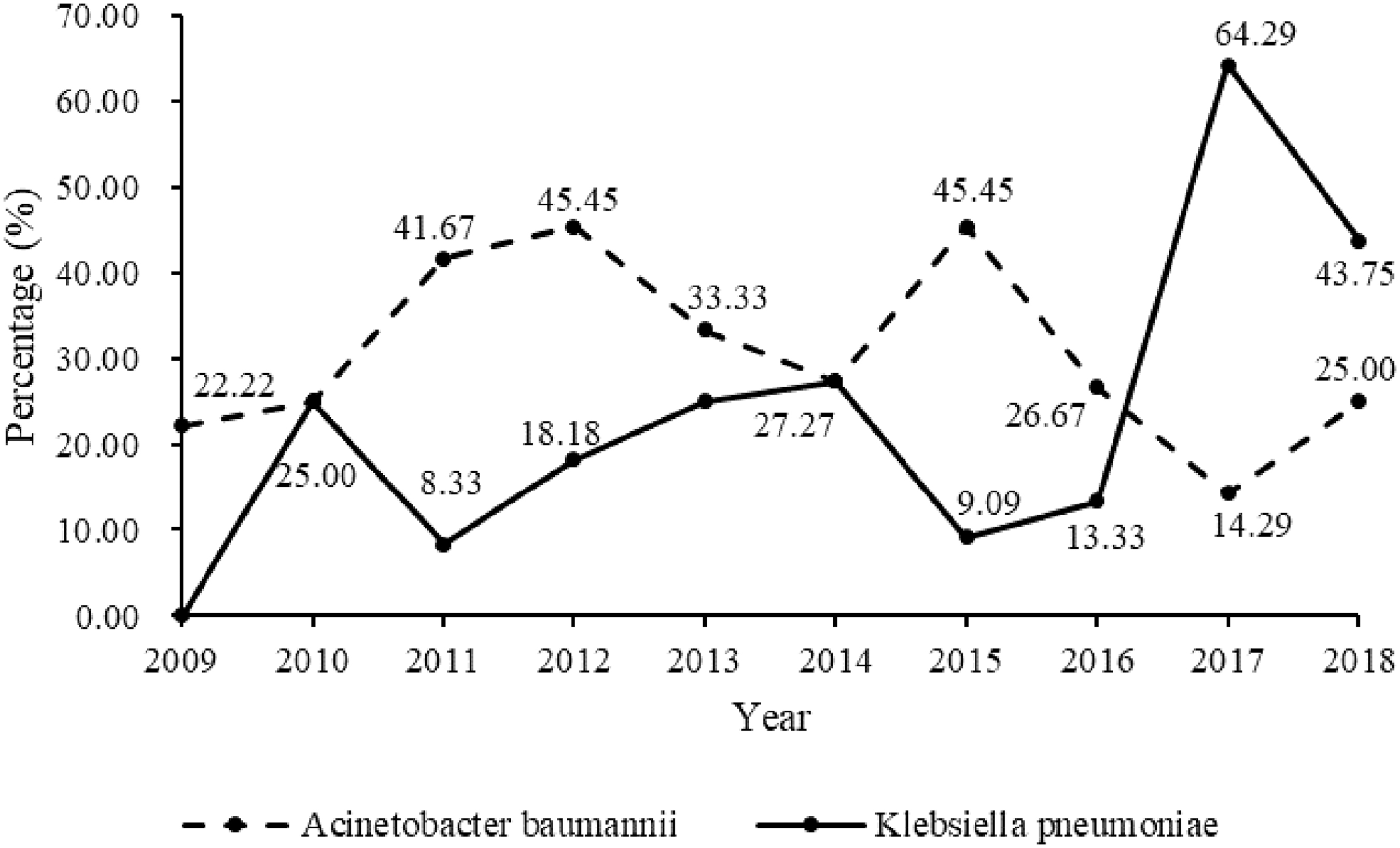
Trends of top two central nervous system infections from 2009 to 2018.
Multi-drug resistant (MDR) and pan-drug resistant (PDR) bacteria
There were 96 strains of GN bacteria. The top three were A. baumannii (44 strains), K. pneumoniae (31 strains), and P. aeruginosa (six strains), among which MDR bacteria accounted for 97.7%, 100%, and 83.3%, respectively. There were 17 strains of PDR bacteria, consisting of 13 strains of Acinetobacter and four strains of K. pneumoniae. Five strains of these PDR bacteria (23.8%) were found in dead patients.
Gram-positive bacteria were isolated 27 times, mainly S. epidermidis (eight times). All of them were sensitive to linezolid, teicoplanin, and vancomycin. The MDR and PDR bacteria are listed in Table 3.
Multi-Drug–Resistant (MDR) and Pan-Drug–Resistant (PDR) Bacteria
Because carbapenem-resistant A. baumannii and P. aeruginosa and carbapenem-resistant and third-generation cephalosporin-resistant Enterobacteriaceae have been ranked as critical-priority bacteria by the World Health Organization (WHO), we further analyzed the resistance of A. baumannii, K. pneumoniae, and P. aeruginosa in our study. Acinetobacter baumannii had the lowest rate of resistance to cefperazone/sulbactam (73.0%) and the highest rate of resistance to ciprofloxacin (97.3%). The resistance rate of K. pneumoniae to amikacin was 64.5%, whereas the resistance rate to ceftazidime was as high as 100%. The resistance rate of A. baumannii to meropenem was 75.7%, but the resistance rate to imipenem was as high as 91.9%. The resistance rates of P. aeruginosa to meropenem and imipenem were 33.3% and 66.7%, respectively. The resistance rates of these three important species are shown in Table 4.
Resistance Rates of Acinetobacter baumannii, Klebsiella pneumoniae, and Pseudomonas aeruginosa Isolated from Cerebrospinal Fluid
TMP/SMX = trimethoprim/sulfamethoxazole.
Relations between pneumonia and CNS infection
Because bacterial pneumonia occurred in most of the patients (82.0%), which increased the risk of CNS infection, we further analyzed the congruence of CSF and sputum cultures in the same patient at the same time. Five kinds of bacteria were present in the same patient's CSF and sputum culture, namely, K. pneumonia, A. baumannii, P. aeruginosa, Serratia marcescens, and Escherichia coli. In the patients with CNS infections with K. pneumoniae, 65.0% had Klebsiella pneumonia. The resistance rate of K. pneumoniae isolated from the CSF ranged from 64.5% to 100%, whereas the resistance rate in those isolated from sputum ranged from 72.3% to 92.3%. The ratios of resistant sputum bacteria to CNS-infecting bacteria are shown in Figure 4. The resistance rates of A. baumannii and K. pneumoniae isolated from sputum are displayed in Table 5.

Ratio of concordant bacteria to central nervous system-infecting bacteria.
Resistance Rates of Acinetobacter baumannii and Klebsiella pneumoniae Isolated from Sputum
TMP/SMX = trimethoprim/sulfamethoxazole.
Discussion
This is the first report on the trends of CNS infection in emergency neurosurgical patients over the last 10 years. We found that GN bacteria were far more common than GP bacteria (78.7% versus 21.3%), specifically that GN bacteria predominated in CNS infections over the last 10 years. Acinetobacter baumannii, K. pneumoniae, and P. aeruginosa were the most common isolates from CSF, and the prevalence of K. pneumoniae increased significantly recently. Moreover, MDR bacteria account for the largest number of organisms.
The rate of intra-cranial bacterial infection ranged from 0.3% to 7.8% [3,11–13]. The large gaps in the rates may be caused by the medical conditions, the level of economic development, and the different inclusion criteria. In our study, the patients suffered from TBI (n = 60) and ICH (n = 34), with a few having other disorders (n = 6). The operations include EVD, ICP implantation, Ommaya implantation, and craniotomy. The incidence of meningitis after moderate or severe head trauma is estimated to be 1.4% and increases to 11% when the injury is combined with open compound cranial fracture [14]. The rate of infection associated with external catheters is approximately 8% [15]. The risk factors for infection include the duration of drainage, changing uninfected catheters, routine sampling of CSF, leakage of CSF at the site, blockage of the drain, and ICH [14]. Although it was thought that the incidence of intra-cranial infections in patients requiring emergency craniotomy may be higher, our data showed the incidence to be 1.4%, which was no higher than for selective craniotomy.
Gram-positive bacteria were said to be the main causes of intra-cranial infection [3,7,8,16]. However, these results came mainly from studies of elective neurosurgical procedures. In our study, there were 123 strains of bacteria cultured from the CSF, and most of them were GN. Indeed, over the 10 years, the number of GN bacterial infections always exceeded that of GP infections. Although Hu et al. reported that the trends of GP and GN bacterial infections were relatively stable in China from 2005 to 2017 [17], we found that the GN bacteria increased to 75.0% over our study. We also found that patients infected with GN bacteria had a higher mortality rate.
Acinetobacter and K. pneumoniae accounted for most of the GN organisms isolated in our study. Other studies had results consistent with ours [18–20]. We analyzed the tendency of A. baumannii and K. pneumoniae from the years 2009 to 2018. The incidence of A. baumannii was relatively stable compared with K. pneumoniae. Acinetobacter accounted for 16 isolates (17.8%) and Klebsiella for 5 (5.6%) from January 2010 to December 2015 [11]. However, we found that Klebsiella infections have surpassed Acinetobacter in the last five years. Specifically, 19 (15.5%) and 18 (14.6%) strains of Acinetobacter were cultured in the first five years and the last five years, respectively, whereas the figures for Klebsiella were 9 (7.3%) and 22 (17.9%). Hu et al. reported that E. coli, K. pneumoniae, A. baumannii, and P. aeruginosa were the top four GN bacteria, of which K. pneumoniae showed an uptrend, whereas A. baumannii showed a downtrend [17]. According to CHINET, the positive rate of K. pneumoniae was 14.7% in 2017, and the positive rate of Acinetobacter was 10.1% [17]. Our study found that Acinetobacter and Klebsiella were the top two GN bacteria. In 2018, the ratio of K. pneumoniae in CSF was 43.8%, whereas the positive rate of Acinetobacter was 25.0%.
We further analyzed the resistance of the top two bacteria in intra-cranial infection as follows. Acinetobacter and Klebsiella accounted for 61.0% of all strains, and most of them were MDR. We also analyzed the resistance rates of Acinetobacter and Klebsiella (see Table 4). Our results showed that Acinetobacter had the lowest resistance to cefperazone/sulbactam (72.97%). Another study found that the resistance to cefperazone/sulbactam of Acinetobacter increased to 46.0% from 2005 to 2017 [17]. In our study, the resistance rate of K. pneumoniae to amikacin was 64.52%, whereas the resistance rate to ceftazidime was as high as 100%. Another study showed that the resistance to amikacin dropped to 14.9% and the resistance to ceftazidime was stable [17]. This difference may be caused by the bacterial sources. The results may provide help for antibiotic selection to clinicians in treating patients with intra-cranial infection early.
Emergency neurosurgical illness itself is an independent risk factor for hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP), which is a leading cause of infection in the neurosurgical intensive care unit. We analyzed the relations between bacterial pneumonia and intra-cranial infection in the same patients. There were 123 strains cultured from CSF of which 52 were consistent with sputum cultures, specifically 24 strains of K. pneumoniae, 23 strains of A. baumannii, three strains of P. aeruginosa, and one strain each of S. marcescens and E. coli. The rates of correlation to the corresponding strains in CSF cultures were 77.0%, 62.0%, 50.0%, 100%, and 100%, respectively. This is consistent with the data of sputum cultures in the emergency neurosurgical center from 2009 to 2018. The top three bacteria causing lung infection were K. pneumoniae (28.8%), A. baumannii (23.0%), and P. aeruginosa (19.5%). This suggests that CNS infections are caused by bacteria translocated from the lung. Measures to mitigate HAP or VAP, such as preventing aspiration, maintaining the head of bed elevated >30∘, continuous subglottic suctioning, oral decontamination, selective digestive decontamination, early tracheostomy, and gastric volume monitoring, may be of benefit in preventing intra-cranial infection. However, further investigation is needed to clarify the value of these measures for this purpose.
Our study had several limitations. First, it was a single-center study, and the results may not be generalizable to other institutions. As our study showed, the prevalence of MDR A. baumannii and carbapenem-resistant K. pneumoniae in this study was higher than in two representative national surveillance network reports on bacterial resistance, the China Antimicrobial Resistance Surveillance System (CARSS) and the China Antimicrobial Surveillance Network (CHINET). Second, as a retrospective study, it is reasonable to assume that some patients were lost before completion. Therefore, the incidence of intra-cranial infection might have been underestimated. Third, the retrospective collection of data resulted in limitations regarding the availability of information. In particular, several potential risk factors for outcome could not be included in our analyses. Despite these limitations, our 10-year study may provide useful reference data for the management of infection and treatment for emergency neurosurgical patients.
Conclusion
Intra-cranial bacterial infection is a serious complication with a potential a high mortality rate. The treatment of patients admitted to emergency neurosurgical centers who suffer intra-cranial bacterial infection is a great clinical challenge with few effective antimicrobial agents remaining. Although the GP bacteria were the most common infection in the CNS after craniotomy, our results showed that GN bacteria govern the intra-cranial infection of emergency neurosurgical patients. Acinetobacter baumannii and Klebsiella pneumoniae were the most common species, of which the trend of A. baumannii incidence was relatively stable, whereas K. pneumoniae showed an upward trend. The results of our study may provide early help for clinicians treating patients with intra-cranial infection.
Footnotes
Acknowledgment
We thank Bei Wang (Huashan Hospital, Shanghai Medical College, Fudan University) for his assistance in collecting data.
Funding Information
This study was supported by the National Natural Science Foundation of China (NSFC Grants 81701206, 81671200, 81471241, 81870968).
Author Disclosure Statement
The authors have no conflicts of interest to disclose. The work is original research that has not been published previously and is not under consideration for publication elsewhere, in whole or in part. The data are available from the corresponding author on request.