
Abstract
Background:
Surgical site infection (SSI) is a serious complication after routine lumbar spinal operations, and its effect on global treatment outcome (GTO) is less reported. The aim of the current study was to measure the impact of SSI on outcome, which was evaluated with patient reported outcome measures (PROMs) and patients' subjective judgment (GTO).
Methods:
A total of 910 patients underwent primary a single- or two-level lumbar decompression or instrumented fusion surgical procedure. Patients completed Visual Analogue Scale (VAS), Oswestry Disability Index (ODI), and Core Outcome Measurement Index (COMI) at baseline and at two-year follow-up. The rate of improvement in PROMs was measured for the total cohort and the group of patients with SSI. Patients evaluated GTO on a five-point Likert scale. This study was approved by the Scientific and Research Ethics Committee of the Medical Research Council (number: 29970-3/2015/EKU) and the Institutional Review Board.
Results:
Regardless of the presence of SSI, significant improvement was measured in all PROMs without any difference in the rate of change between the clinical subgroups (non-SSI vs. SSI, dODI: p = 0.370, dCOMI: p = 0.383, dVAS: p = 0.793). In the total cohort, 87.3% of patients reported good outcome (N% = 87.3%). After an SSI, however, more patients (25.7%) reported poor outcome compared with those without the complication (chi-square test: value = 5.66; df = 1; p = 0.017; odds ratio = 2.49).
Conclusions:
Patients with successfully treated SSI can expect as good objective clinical result as patients without SSI while the subjective treatment outcome can be worse. The GTO could also be improved in complicated cases, however, with more extensive peri-operative patient education and information considering the patients' expectations, too.
Surgical treatment of degenerative lumbar disc disease can help for many patients after failed conservative treatment. Spine surgical interventions can lead to some complications just like any other invasive procedures. Surgical site infection [SSI] is a potentially serious complication after lumbar spine operation. Posterior approach open spinal surgical procedures have one of the highest rissk for SSI within orthopedic interventions [1]. The SSI results in prolonged length of hospital stay and higher treatment costs [2–6]; hence, it has a significant impact on morbidity and death [2].
For all these reasons, many articles have been published about the prevention, incidence, and prevalence of SSI [7–12], risk factors [7,10–16], diagnosis [4,5,9,17], and treatment options [8,18]. Very few publications, however, can be found in the literature about the influence of an SSI on the long-term outcome of the surgical treatment.
The success or outcome of a surgical intervention can be judged based on many different criteria, and it can be significantly influenced by a post-operative adverse event [19]. Lack of complications, an illustrious radiologic documentation, or the judgments of the surgeon are inappropriate success criteria in elective operations [20]. Validated functional outcome measures as well as the patient's opinion must be included in the evaluation [21].
Several different measurement tools have been developed to monitor the efficacy of treatment in terms of the patient. Most of these instruments were developed to measure the outcome in the case of a well-defined pathology or a specific condition. These instruments were collected into six different categories by Vavken et al. [22]. The most frequently used measurement tools in spine operations are pain scales (e.g., visual analogue scale, VAS; numeric rating scale, NRS), and questionnaires for disability (e.g., Oswestry Disability Inde [ODI] questionnaire, ODI), psychometric issues (e.g., Modified Somatic Perception Questionnaire), and combined assessment scales (e.g., Scoliosis Research Society22; Short Form [SF]-12; SF-36).
Global treatment outcome can be judged in terms of different criteria. Mannion et al. [23] recommended separating the two concepts of “overall effectiveness of treatment” and “satisfaction with the treatment delivered.” The term “satisfaction” also includes the patient-provider relationship and estimation of the surgeon. The “effectiveness of a treatment,” however, estimates primarily the rate of improvement by treatment and how much the treatment helped the symptoms.
The aim of our study was to analyze the effect of SSI on treatment outcome measured by different patient reported outcome measures (PROMs) and by patients' subjective judgment on the global effectiveness of treatment in a cohort of patients who underwent the most frequently performed, elective lumbar spinal surgical procedures because of degenerative disc disease.
Methods
Study cohort
Adult patients who underwent single- or two-level primary lumbar spinal operation because of degenerative pathology (e.g., disc herniation, secondary canal spinal stenosis, segmental instability, spondylolisthesis) were recruited in our study between May 2009 and December 2012. Patients with previous lumbar spine operation and revision surgical procedures or spine operation because of neurologic emergency conditions were excluded from the study.
Surgical procedures
All study participants underwent microdiscectomy, decompression, or instrumented fusion (transforaminal lumbar inter-body fusion or posterior fusion) operation. All procedures were performed from a standard median-sagittal posterior approach and were performed by orthopedic spine surgeons.
Diagnosis and management of SSIs
The current guideline published by the Centers for Disease Control and Prevention was used to define SSI after spine operation in 2014 [24]. Clinical findings, laboratory tests, microbiologic cultures from the surgical wound or from blood as well as radiologic imaging were the pillars of diagnosis making [17]. Both superficial and deep SSIs were considered. Management of SSI was based on national [25] and international [17] guidelines. Summary, surgical debridement was performed in case of an abscess, inflammatory process under the fascia, or a deteriorating septic condition. Intravenous or oral antibiotic agents were administered depending on patient condition, laboratory findings, and results of microbiologic cultures.
PROMs
Demographic and clinical data about patients were collected during the standard course of medical care. Study participants completed PROMs to assess the level of pain with the use of VAS and to measure disability and functional capacity with the completion of the validated versions of ODI [26] and Core Outcome Measurement Index (COMI) [27] at baseline and at two years after the index spinal operation.
Two years after the index spinal operation, patients were asked to evaluate the global effectiveness of surgical treatment. Global Treatment Outcome (GTO) was measured using the method published by Mannion et al. in 2005 [28]. Patients could evaluatd their GTO on a five-point Likert scale. Two clinical outcome subgroups were developed based on their answers. The “good” clinical outcome subgroup consisted of those who evaluated the overall result of the surgical intervention as “very good” or “good.” Those patients, however, who reported the clinical outcome as “satisfactory,” “bad,” or “worse than before” were categorized into the “poor” clinical outcome subgroup.
Statistical analyses
Prospectively collected data of patients was analyzed. Changes between pre-operative and post-operative status of mean scores were compared with paired t tests. Unpaired t tests were used to analyze the difference in PROMS mean scores in terms of SSI and GTO. The GTO were analyzed in terms of occurrence of SSI applying the chi-square test. Statistical analyses were performed with SPSS 20.0 software package (IBM Co., Armonk, NY), and with MedCalc 12.5 software (MedCalc Software, Ostend, Belgium). Post-hoc power of the study calculations using online tools (https://clincalc.com/stats/Power.aspx) were conducted to determine the statistical power provided by the sample size.
Study approval
This study was approved by the Hungarian Scientific and Research Ethics Committee of the Medical Research Council (number: 29970-3/2015/EKU). The Institutional Review Board of the National Center for Spinal Disorders also approved this protocol. All patients provided written informed consent for study participation.
Results
Study cohort
In the present clinical study, prospectively collected data of 910 patients were analyzed. The final study cohort is shown on Figure 1.
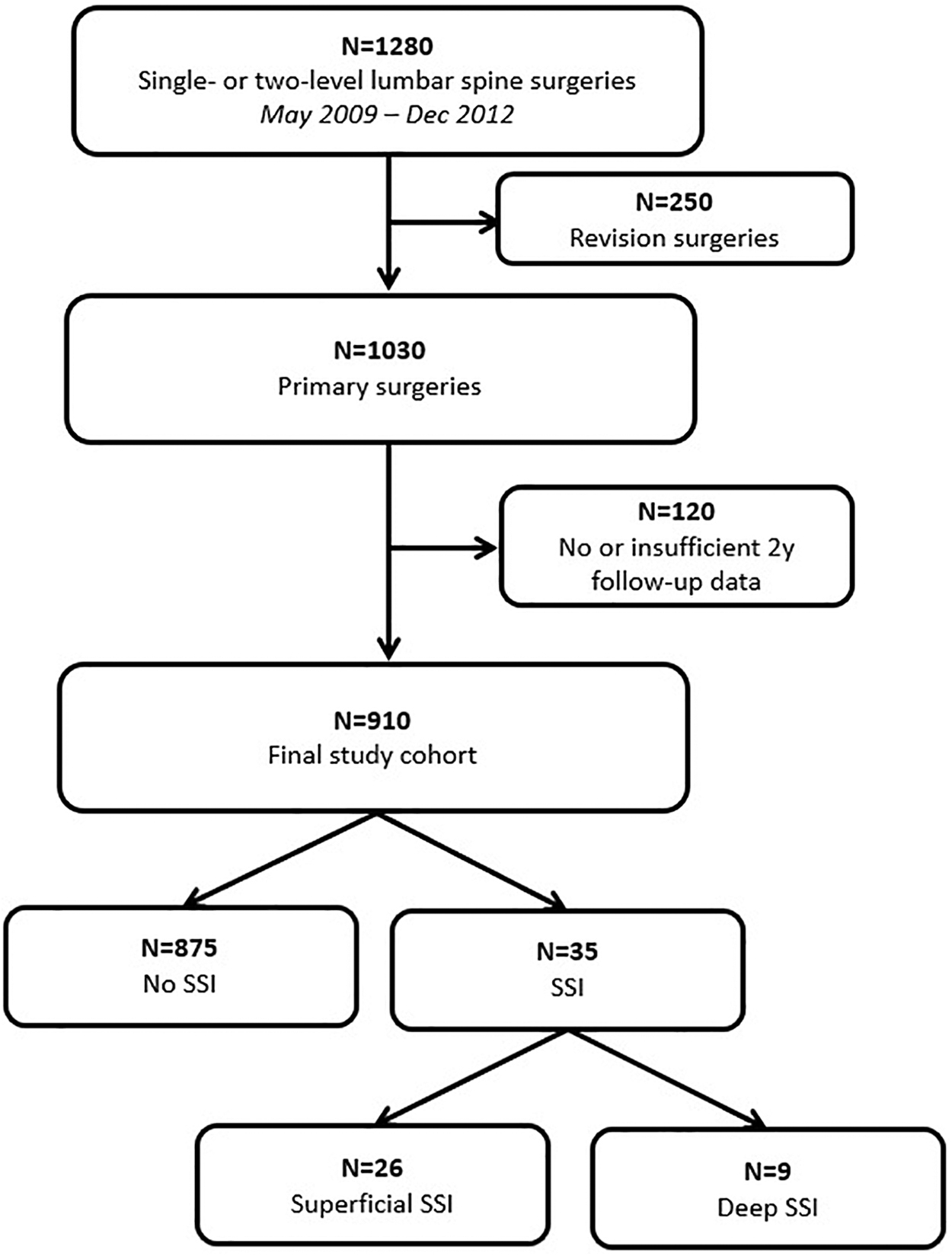
Flowchart of the final study cohort. SSI = surgical site infection.
Demographic and surgical data
Baseline characteristics of the study cohort are listed in Table 1. The prevalence of SSI was 3.8% in the entire cohort (N = 35). Most of the SSIs were superficial (N = 26; 74.3%). Most of SSIs were caused by Staphylococcus aureus (N = 14) or coagulase negative Staphylococcus (N = 7). No significant difference was found in the proportion of gender (p = 0.840) and age (p = 0.081) between SSI and non-SSI subgroups. Current smoking status did not differ between the subgroups (p = 0.987).
Baseline Demographic of Study Cohort
SSI = surgical site infection; SD = standard deviation; BMI = body mass index; PROMs = patient reported outcome measures; ODI = Oswestry Disability Index; COMI = Core Outcome Measurement Index; VAS = Visual Analogue Scale.
Those with an SSI, however, had a significantly higher weight (p = 0.022) and body mass index (p = 0.001). Baseline clinical status in terms of the scores of the PROMs did not show any significant difference in the subgroups. Neither spinal instrumentation nor operated levels were differently distributed in the SSI subgroup (chi-square = 0.745; df = 1; p = 0.246 and chi-square = 0.059; df = 1; p = 0.808, respectively).
Management of SSI
All patients with SSI regardless of its depth received medical treatment. Surgical debridement was performed in 22 (62.9%) patients. In the superficial SSI subgroup, 14 patients underwent a debridement surgical procedure, and all of them were treated with oral antibiotic agents based on their culture results for 14 days. In the case of deep SSI, patients received antibiotic agents for six weeks.
Almost all those with deep wound SSI (N = 8) underwent debridement. One of the patients with deep SSI has not been re-operated. This patient had a two-level decompression without any spinal instrumentation. The SSI could be controlled with targeted antibiotic agents, and the patient wore a stiff brace for three months. None of the patients with SSI required removal of the previously implanted spinal instrumentations.
Outcome
Treatment outcome was analyzed from different aspects. A significant improvement (p < 0.001) at two-year follow-up was measured by all the PROMs for the total cohort and for the sub-cohorts as well (Fig. 2).

Mean scores of patient reported outcome measures at baseline and two-year follow-up. ODI = Oswestry Disability Index; COMI = Core Outcome Measures Index for low back pain; VAS = Visual Analogue Scale for pain.
No significant changes were found in the rate of improvement in PROM scores between patients with and without SSI (Fig. 3). The ODI improvement was 25.7 ± 22.1 points among patient without SSI and 22.0 ± 28.1 in the group of patients with SSI (p = 0.370). The COMI scores showed similar improvement: 3.9 ± 3.3 points in patients without SSI and 4.0 ± 2.7 in patients with SSI (p = 0.383). Improvement is VAS scores was 4.2 ± 3.8 points in patient without SSI and 3.7 ± 3.3 in SSI patients (p = 0.793).

Changes in mean scores (pre-operative vs. two-year follow-up) in the two subgroups. SSI = surgical site infection; ODI = Oswestry Disability Index; COMI = Core Outcome Measures Index for low back pain; VAS = Visual Analogue Scale for pain.
The rate of improvement in PROM scores was also analyzed according to the depth of SSI. Patients with superficial SSI had 23.7 ± 28.4 points improvement in ODI, 4.2 ± 3.2 points in COMI, and 4.2 ± 3.8 points in VAS. Patients with deep SSI showed 16.4 ± 28.7 points improvement in ODI, 2.8 ± 3.7 points in COMI, and 3.3 ± 4.1 points in VAS. Depth of SSI did not have a significant effect on the rate of improvement in PROM scores (dODI: p = 0. 561; dCOMI: p = 0.374; dVAS: p = 0.637).
Most of the patients reported a good outcome at two-year follo- up after the index spinal surgical procedure in the total cohort (N = 794, 87.3%). Nevertheless, a greater proportion of patients who underwent surgical treatment without spinal instrumentation reported a better GTO than those who were treated with spinal fusion (90.6% vs. 83.4% good outcome, chi square = 10.553; df = 1; p = 0.01).
The GTO was reported similarly good (87.8% good outcome) among patients without SSI. More patients (25.7%) who had SSI, however, reported poor outcome compared with those without SSI (12.2%) (chi-square test = 5.66; df = 1; p = 0.017). The odds ratio (OR) for having a poor outcome was 2.49 (95% confidence interval [CI]: 1.13–5.45) in the case of post-operative SSI (Fig. 4).
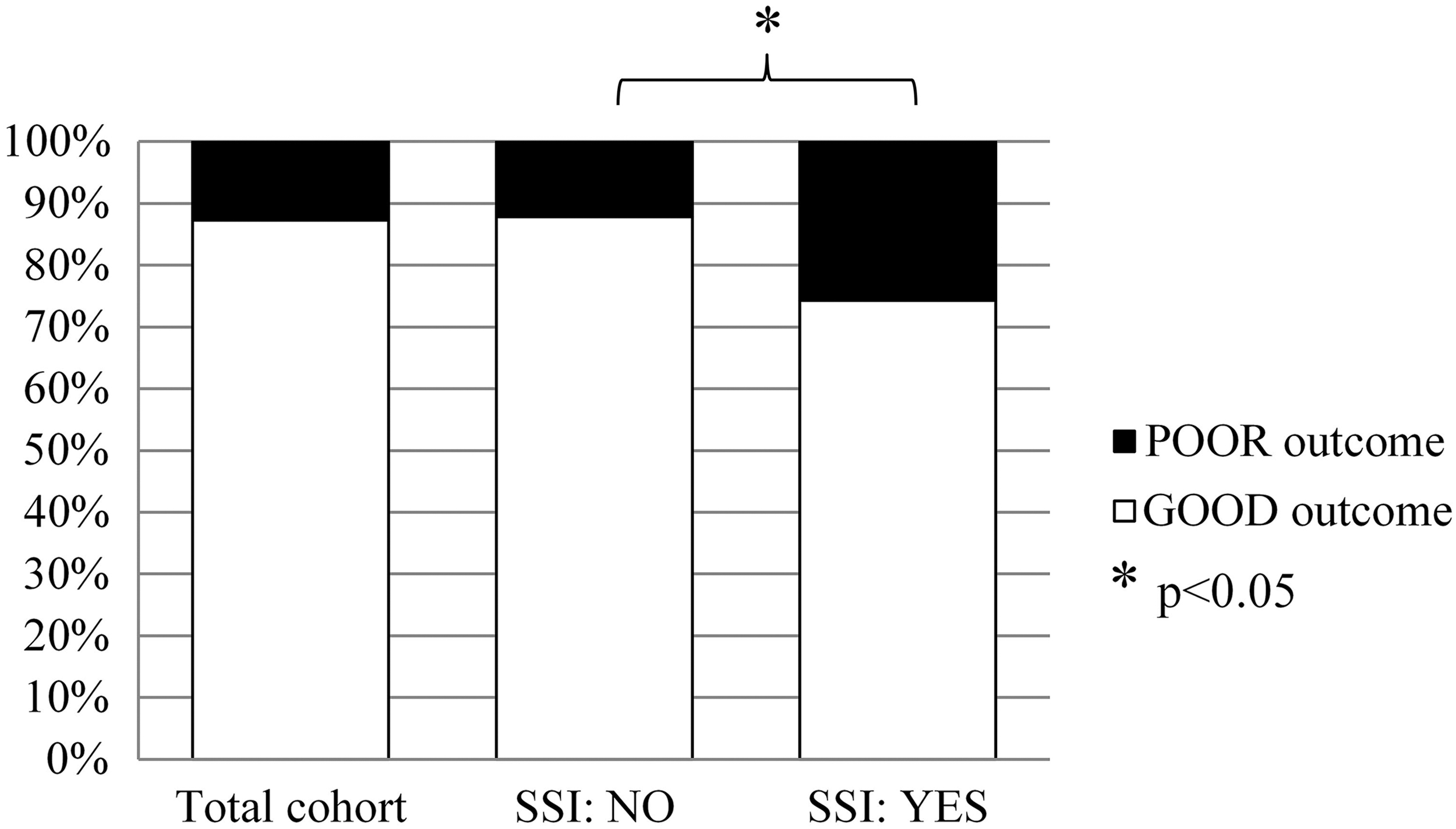
Global treatment outcome two years after the index operation. SSI = surgical site infection; * = significant difference, p < 0.05.
Deeper analysis of the GTO categories showed that 67.5% of the patients without SSI gave the best rate (“very good”) for their overall clinical results. Among patients with SSI, only 42.9% gave the best rate. Further, 1.7% of patients without SSI rated their final clinical results with the worst option (“worse than before”), while 8.6% of patients with SSI chose the worst category (Fig. 5)
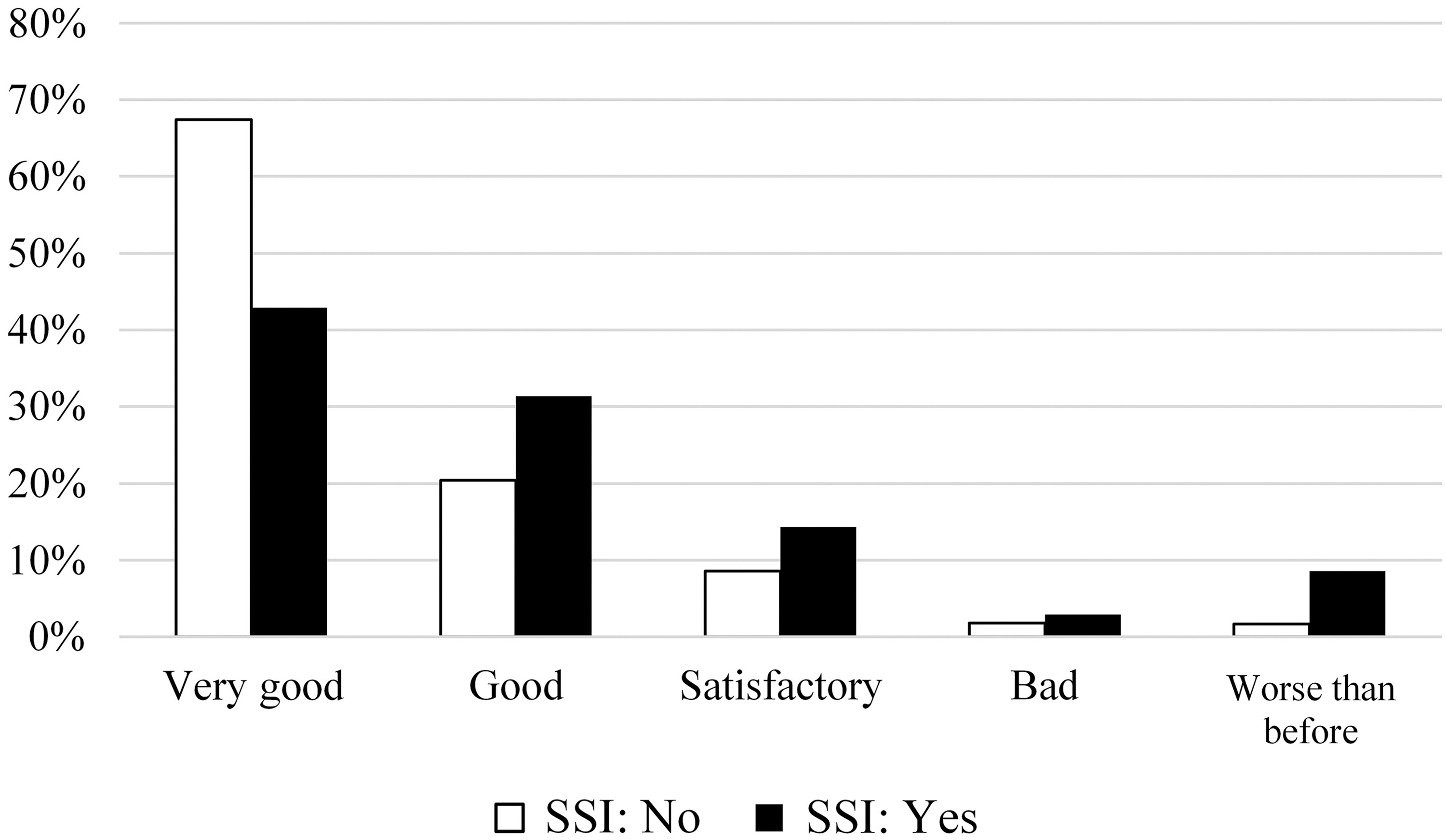
Global treatment outcome categories. SSI - surgical site infection.
Poor outcome was reported at a higher rate by patients with deep wound SSI than patients with superficial SSI (55.6% vs. 15.4%; chi-square test = 5.65; df = 1, p = 0.03). There were 22 patients in the SSI group who underwent a second surgical procedure because of SSI, which was not a signifcant predictor of poor outcome (p = 0.282). Patients with a second surgical procedure have as good improvment in PROMs as patients who did not have a second operation (dODI: p = 0.306; dCOMI: p = 0.660; dVAS: p = 0.628).
A detailed power of the study calculation showed that the sample size was high to detect the significant clinical changes in the PROMs in the subgroups (e.g., only a group of eight subjects is enough to detect the decrease of the pre-operative 46.6 ± 18.4 ODI score to the post-operative 20.9 mean score at an alpha level of 0.05 and with 80% power). Our sample size, however, provided a 65.3% power for the chi-square test applied for the analysis of the effect of SSI on GTO (chi-square test = 5.66; df = 1; effect size [Phi] = 0.078).
Discussion
In this study, the treatment outcome of 910 surgically treated patients was measured by three different PROMs targeting pain intensity, disability, and functional capacity. In addition, the patients' subjective judgment of the GTO was investigated on a five-item Likert scale [23]. Two years after the index spinal surgical procedure, a significant improvement in the clinical status measured by PROMs was detected regardless of the occurrence of SSI. Looking at the total cohort, most patients reported a good GTO at two-year follow-up. Similarly, high magnitude of good GTO was reported by the patients without SSI.
In contrast, a significantly higher proportion of patients with SSI reported poor long-term GTO despite the successful management of the complication and the fact that the clinical improvement measured by PROMs did not differ from the non-SSI group. Expressed in numbers, SSI was associated with an increased risk of poor long-term outcome by 2.5-fold.
Similar good clinical results after spinal operation with and without SSI have been published in a few studies, but mostly with a low number of participants. Glassman et al. [29] found significant improvement in PROMs using combined assessment scales (short form [SF]-12, Scoliosis Research Society [SRS]-22), a questionnaire for disability (ODI), and also the numeric rating scale for pain both in patients with and without SSI one year after adult spinal deformity operation (number of SSI cases: N = 46).
Mok et al. [4] reported good clinical results measured with SF-36 in patients with SSI (N = 16) compared with patients without SSI (N = 16 ) two years after instrumented thoracolumbar spinal fusion operation. Petilon et al. [30] measured significant improvement at one-year follow-up after instrumented spinal fusion operation with deep wound infection (N = 30) using ODI, SF-36, and NRS for back and leg pain. Rhin et al. [31] reported significant improvement among patients with an infection after surgical treatment of adolescent idiopathic scoliosis using SRS-24 (N = 7 infection cases). Patients with SSI were more unsatisfied with the treatment outcome, however, and knowing the results, they would not choose the surgical treatment again.
The importance of patient opinion was highlighted by Lattig et al. [19] who found that patients and surgeons agreed only about 50% on global treatment outcome three months after surgical treatment. A significant correlation was found among the incidence of patient-rated complications, global treatment outcome, and patient satisfaction one year after cervical and lumbar spinal operations by Grob et al [32]. Falavigna et al. [33] found no significant difference in the improvement of pain, ODI, and SF-36 between patients having deep wound infection (N = 13) and a matched control group after instrumented lumbar spinal fusion; however, a higher proportion of patients with SSI was not satisfied with the treatment procedure at the final evaluation (53.8 % vs. 15.4%).
The difference between the results of PROMs and patient-reported GTO in the group of patients with SSI is a thought-provoking question. Possible explanations addressing these findings can be found in the scientific literature. Insufficient pre-operative patient education and information may play an important role in this discrepancy. The importance of patient education was confirmed by Sitzia et al. [34] who found a strong correlation between patient education and good treatment outcome. Mannion et al. [35,36] recommended clarifying before the operation possible patient expectations about the surgical treatment and the potential complications; thus, patients would have a realistic conception during the entire medical treatment process when a complication occurs.
Psychological factors may also have an important effect on treatment outcome. Havakeshian et al.[37] found a positive correlation between higher level of fear avoidance beliefs about physical activity and poor treatment outcome one year after non-instrumented lumbar decompression operation. Unfavorable GTO in patients with SSI also can be associated with the complicated life period immediately after the surgical procedure characterized by inconveniences and threats such as prolonged hospitalization, additional medications, and side effects, stress, and frustration.
This study has some possible limitations. Despite the fact that the investigation period was nearly three and a half years, there was a relatively small number of cases in the SSI group, especially in the deep SSI subgroup. A further weakness can be that the seriousness of an SSI event could not be measurable objectively, which may have an uncertain effect on GTO. Measuring the seriousness of SSI also can be complicated for many reasons.
There are several factors that individually can affect the severity of infection (e.g., intensive treatment unit support required, need for prolonged antibiotic therapy, cumulative effect with patient-specific comorbidities, multi-resistant organism). Aggravating effects of these factors are difficult to determine separately. A prospective, multi-center study with higher number of SSI cases would be required to clarify the deep associations between SSI and poor treatment outcome.
Conclusions
Patients with SSI after an elective lumbar spinal operation have as hopeful an expectation for objectively measured good clinical status as patients without SSI. Objectively measured improvement in pain and disability is as great as in those who did not have this complication. Surprisingly, these patients rate their global treatment outcome poorer, which can be associated with the psychosocial consequences of a severe post-operative complication. Better management and psychological support can improve the GTO even in this endangered patient group.
Footnotes
Funding Information
No funding was received for this work.
Author Disclosure Statement
No competing financial interests exist.