
Abstract
Background:
Parapneumonic effusion (PPE) and thoracic empyema (TE) necessitate prompt differential diagnosis regarding their unequal rates of mortality and disparate methods of treatment.
Patients and Methods:
A total of 80 patients with equally divided between the PPE and TE groups were evaluated in terms of age, gender, side of the affected hemithorax, and peripheral blood counts including white blood cell (WBC) count, C-reactive protein (CRP), lymphocyte, monocyte, and lymphocyte-to-monocyte ratio (LMR).
Results:
The difference between the two groups in terms of age, gender, side of the disease, and monocyte count was not statistically significant (p > 0.05) whereas WBC count, lymphocyte, and LMR was significantly higher in the TE group (p < 0.05). Lymphocyte-to-monocyte ratio over 2.45 was a differential diagnostic test of PPE and TE at 85% sensitivity and 87.5% specificity.
Conclusions:
Lymphocyte-to-monocyte ratio is an effective indicator to finalize the differential diagnosis of PPE and TE when combined with high levels of serum WBC, CRP, and lymphocytes in addition to clinical and radiologic findings.
A parapneumonic effusion (PPE) is the accumulation of fluid in the pleural space after pneumonia, lung abscess, bronchiectasis, trauma, or cardiothoracic surgery whereas thoracic empyema (TE) is described as the collection of pus in the thoracic cavity. Patients with pneumonia may develop PPE and TE at rates up to 40% and 15%, respectively [1].
Epidemiologic data concerning the organisms causing pleural infections vary widely among countries. The most isolated bacteria of TE are reported as streptococci, staphylococci, and anaerobes whereas methicillin-resistant Staphylococcus aureus (MRSA) and Mycobacterium tuberculosis constitute more serious cases [2].
Differential diagnosis of PPE and TE is based on physical examination, radiologic findings, and pleural fluid examination. Given that the mortality rate of patients with TE is 15%–20% and even higher in immunocompromised cases, rapid and influential diagnostic and therapeutic approaches are essential [3].
Simple PPEs may resolve with adequate antibiotic therapy without the need for drainage unless the amount of pleural fluid is larger than or equal to half hemithorax. Conversely, diagnosis of TE necessitate rapid drainage of the thoracic cavity and potential demand for intrapleural instillation of fibrinolytics or decortication.
Recent studies support lymphocyte-to-monocyte ratio (LMR) as a good predictor in any inflammatory events such as malignancies. This study aimed to reveal the effect of LMR in the differential diagnosis of PPE and TE.
Patients and Methods
The patients who were treated for TE and PPE between 2000 and 2018 were analyzed retrospectively. Those patients who had a history of chest surgery, thoracic trauma, or any malignancies and also died during the course of treatment were excluded from the study.
A total of 80 patients equally divided between PPE and TE were examined in terms of age, gender, and side of the affected hemithorax. Moreover, serum WBC, C-reactive protein (CRP), lymphocyte, monocyte counts, and LMR measured in the peripheral blood were noted for every patient at the time of diagnosis.
The patients were diagnosed with PPE by identifying a pleural effusion, which is thicker than 10 mm on a lateral decubitus radiographic study and pleural fluid analysis presenting glucose level >40 mg/dL, pH > than 7.2, and lactate dehydrogenase (LDH) <1,000 IU/L.
Presence of TE was confirmed via positive microbial staining or culture, white blood cell (WBC) count higher than 15,000 cells/mm3, protein level higher than 3 g/dL, pH <7.2, and LDH >1,000 IU/L in the pleural fluid.
SPSS (IBM SPSS for Windows, version 24, IBM Corp, Armonk, NY) statistical package program was used for calculations. Descriptive statistics for continuous parameters in the study were expressed as mean, standard deviation, minimum, and maximum whereas categorical parameters were expressed as number (n) and percentage (%). After verifying that the data were normally distributed via Shapiro-Wilk and Skewness-Kurtosis tests, parametric tests were applied. Independent t-test was used to compare average of measurements for patient groups and Pearson correlation parameters were calculated to determine the relation between the measurements. The χ2 test was used to reveal the relation between categorical parameters. Sensitivity, specificity, and cutoff values were calculated via receiver-operating characteristic (ROC) analysis. The statistical significance level (α) was taken as 5%.
Results
Patients (n = 80) included 41 (51.3%) men and 39 (48.7%) women. Mean age was 48.2 ± 11.2 (range = 21–74) years. Right hemithorax affected 44 cases (55%) and left hemithorax affected 36 (45%) cases.
Regarding the two groups, PPE had 20 (50%) and TE had 21 (52.5%) men; mean age was 46.3 for PPE and 50.1 years for the TE group. Right hemithorax was present in 23 (47.5%) for PPE and 21 (52.5%) patients for TE. The difference in terms of age, gender, and side of the disease was not statistically significant (p > 0.05). The findings are summarized in Table 1.
General Features and Group Comparison
χ2 test.
SD = standard deviation; PPE = parapneumonic effusion; TE = thoracic empyema.
With regards to serum markers assessed in two cohorts of diseases, a series of statistical analysis revealed a significant difference in levels of WBC, CRP, lymphocyte, and LMR (p < 0.05). Mean values of WBC was 12,917.3 cells/mm3, CRP 87.1, lymphocyte 1,852.8 cells/mm3, and LMR 2.76 presenting higher levels in patients with TE. On the other hand, mean monocyte count was calculated as 712.5 cells/mm3 for PPE and 676.3 cells/mm3 for TE, which did not comprise a significant difference between these two diseases (p > 0.05). Comparison of serum markers for both groups is provided in Table 2.
Analysis of Tests Applied in Patients with PPE and TE
Independent t-test.
PPE = parapneumonic effusion; TE = thoracic empyema; SD = standard deviation; Min = minimum; Max = maximum; WBC = white blood cell count; CRP = C-reactive protein; LMR = lymphocyte-to-monocyte ratio.
Receiver-operating characteristic analysis discovered cutoff values of 12,335 cells/mm3 for WBC, 57.5 for CRP, 1,524.5 cells/mm3 for lymphocyte, and 2.45 for LMR in the differential diagnosis of PPE and TE. Moreover, sensitivity was calculated as 72.5% for WBC, 77.5% for CRP, 67.5% for lymphocyte, and 85% for LMR whereas specificity was 77.5% for WBC, 80% for CRP, 67.5% for lymphocyte, and 87.5% for LMR (Fig. 1, Table 3).
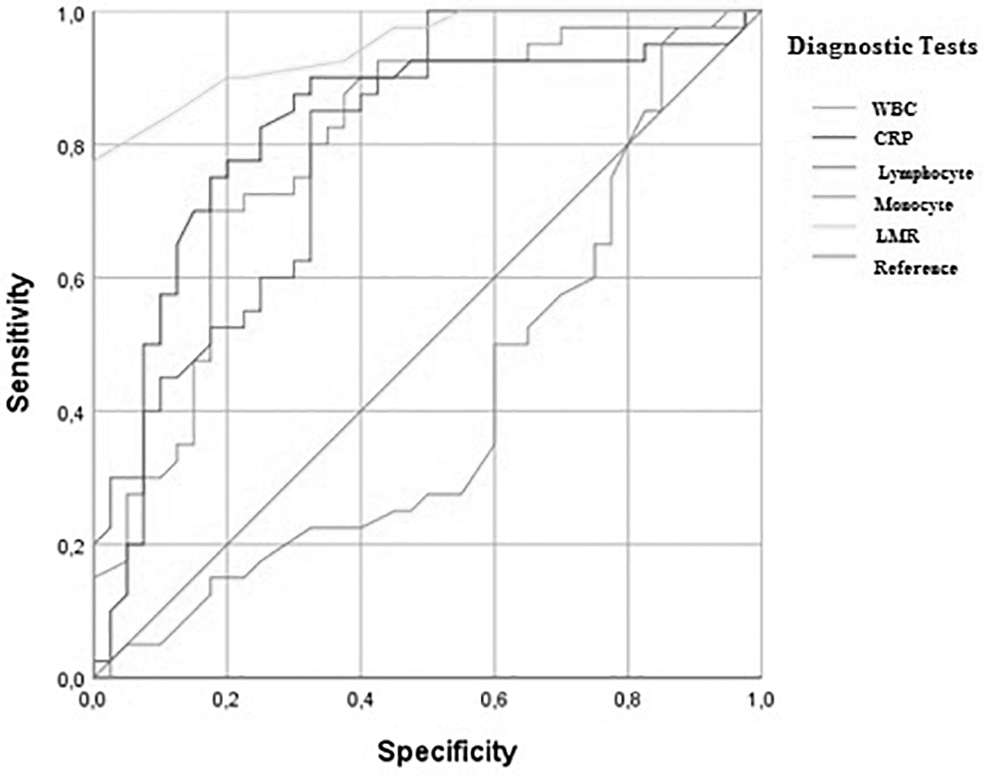
Sensitivity and specificity of diagnostic tests.
Serum Markers in Differential Diagnosis of PPE and TE
p > 0.05.
PPE = parapneumonic effusion; TE = thoracic empyema; WBC = white blood cell count; CRP = C-reactive protein; LMR = lymphocyte-to-monocyte ratio.
After microbial staining and cultures, the most frequently identified micro-organisms were Streptococcus pneumoniae (27.5%, n = 11) and Staphylococcus aureus (22.5%, n = 9) in PPEs, also Streptococcus pneumoniae (35%, n = 14) and Escherichia coli (20%, n = 8) in TEs. Thus, no organisms were identified in 19 (47.5%) patients with PPE whereas one patient with PPE and three patients with TE were diagnosed with Mycobacterium tuberculosis in their pleural effusions. The most frequently recognized etiologic factor was pneumonia for both PPE and TE (35% and 45%, respectively) followed by thoracic surgery (20%) for PPE, abdominal infections, cardiac, and thoracic surgeries at equivalent rates of 15% for TE. Etiology and causative micro-organisms are both provided in Table 4.
Micro-Organisms and Etiology Identified in the Pleural Effusions
PPE = parapneumonic effusion; TE = thoracic empyema.
All of the patients were initially diagnosed with PPE or TE via thoracentesis. The pleural fluid was drained by repetitive thoracentesis in six (15%) and pleural catheters in eight (20%) patients with PPE whereas the rest of the patients were followed up with antibiotic agents. Among the patients with TE, 24 (60%) chest tubes and 16 (40%) pleural catheters were inserted and pleural drainage was adequate for 28 (70%) patients. Thoracotomy was performed later for eight (20%) patients and the remaining four (10%) cases underwent thoracoscopy. Chest wall stoma was placed in two (5%) patients for whom previous surgical interventions failed to achieve treatment.
Discussion
The findings of this study clearly show that WBC, CRP, and lymphocyte contribute to establishing the diagnosis of PPE and TE whereas LMR is a superior differential method of measurement for these diseases presenting with high rates of sensitivity and specificity.
Pneumonia can be complicated by the development of a parapneumonic effusion and empyema, increasing the expected 5% mortality rate up to 20% [3,4]. Without prompt diagnosis and appropriate treatment, this rapidly progressing process occurs at rates as high as 15% [5].
The aggressive nature of intrathoracic infections necessitates inexpensive, easily applicable and accessible diagnostic tests. As in any other inflammatory events, serum markers try to achieve diagnosis and also to follow-up the treatment of pleural PPE and TE.
Recent studies focus mostly on the availability of LMR as a diagnostic and also as a prognostic utility. Lymphocyte-to-monocyte ratio has been considered as an independent prognostic marker and predictor of antituberculous treatment [6,7]. Okba et al. [8] reported that LMR had been an independent indicator of active ulcerative colitis by detecting the degree and extent of involvement. and could also reduce the need for invasive endoscopies. Moreover, low LMR was announced as a negative prognostic marker in patients with stage 3 colon cancer [9] whereas elevated pre-operative LMR was independently associated with poor long-term survival in patients with hepatocellular carcinoma [10]. Lee et al. [11] demonstrated that LMR was useful in providing independent and additional prognostic information in follicular lymphoma.
Unfortunately, the current literature does not include studies that address the utilization of peripheral blood count parameters for the diagnosis of PPE or TE. Limited by its retrospective design and selected population as a single-center research, the study still emphasizes elevated WBC, CRP, and lymphocyte counts as signs for a pleural infection. Moreover, LMR is a supporting verification to finalize the differential diagnosis of PPE and TE at 85% sensitivity and 87.5% specificity.
Conclusions
Pleural infections are diseases of importance with increasing incidences and substantial mortality rates. Elevated levels of WBC, CRP, and lymphocyte counts point out the existence of a severe infection. A LMR over 2.45 provides supporting evidence to confirm the diagnosis when combined with the traditional diagnostic criteria of TE.
Funding Information
No funding was received.
Footnotes
Author Disclosure Statement
No competing financial interests exist.