
Abstract
Background:
The post-operative management of simple (acute) appendicitis differs throughout the United States. Guidelines regarding post-operative antibiotic usage remain unclear, and treatment generally is dictated by surgeon preference. We hypothesize that post-operative antibiotic use for simple appendicitis is not associated with lower post-operative complication rates.
Methods:
In a post-hoc analysis in a large multi-center observational study, only patients with an intra-operative diagnosis of AAST EGS Grade I were included. Subjects were classified into those receiving post-operative antibiotics (POST) and those given pre-operative antibiotics only (NONE). Clinical outcomes examined were length of stay (LOS), 30-day emergency department (ED) visits and hospital re-admissions, secondary interventions, surgical site infection (SSI), and intra-abdominal abscess (IAA).
Results:
A total of 2,191 subjects were included, of whom 612 (28%) received post-operative antibiotics. Compared with the NONE group, POST patients were older (age 37 [range 26–50] versus 33 [26–46] years; p < 0.001), weighed more (82 [70–96] versus 79 [68–93] kg (p = 0.038), and had higher white blood cell counts (13.5 ± 4.2 versus 13.1 ± 4.4/103/mcL (p = 0.046), Alvarado Scores (6 [5–7] versus 6 [5–7]; p < 0.001), and Charlson Comorbidity Indices (median score 0 in both cohorts; p < 0.001). The POST patients had a longer LOS (1 [1-2] versus 1 [1-1] days; p < 0.001). There were no differences in the number who had ED visits within 30 days (9% versus 8%; p = 0.435), hospital re-admission (4% versus 2%; p = 0.165), an index hospitalization SSI (0.2% for both cohorts; p = 0.69), an SSI within 30 days (4% versus 2%; p = 0.165), index hospitalization IAA rate (0.3% versus 0.1%; p = 0.190), 30-day IAA (2% versus 1%; p = 0.71), index hospitalization interventions (0.5% versus 0.1%; p = 0.137) or 30-day secondary interventions (2% versus 1%; p = 0.155).
Conclusions:
Post-operative antibiotic use after appendectomy for simple appendicitis is not associated with better post-operative clinical outcomes at index hospitalization or at 30 days after discharge.
Acute appendicitis is the single most common cause of the acute abdomen and most common impetus for urgent operation performed in the United States, with more than 250,000 appendectomies performed annually [1-4]. Appendicitis can be encountered in multiple forms: Simple, perforated, and gangrenous, with the type affecting the operative and post-operative complications [5].
Multiple studies have shown recently that discharge from the recovery room after laparoscopic appendectomy for simple acute, non-perforated appendicitis is safe and effective [6,7]. However, the routine management of this patient population with respect to the use of post-operative antibiotics is limited and controversial. In 2016, the Surgical Infection Society released Task Force Guidelines stating that “Patients undergoing source control for intra-abdominal contamination without an established infection or for an uncomplicated IAI in which the source control procedure can completely eradicate the infection, the task force concluded that antimicrobial use should be limited to no more than 24 hours.” However, some surgeons continue to discharge patients on antibiotics for various amounts of time, whereas others adhere to the SIS 2016 guidelines and find a single pre-operative dose to be sufficient.
The present study reviewed the experience at multiple institutions to compare complication rates for simple appendicitis after appendectomy with respect to different post-operative antibiotic practices. We hypothesized that post-appendectomy antibiotic administration in simple appendicitis is not associated with reduced complication rates.
Patients and Methods
This multi-center prospective observational study was approved by the Eastern Association for the Surgery of Trauma (EAST) and by the Institutional Review Boards of all participating sites. Prospective enrollment occurred between January 26, 2017 and June 30, 2018. All adult (age ≥18 years) patients with a confirmed, or strong suspicion of, acute, perforated, or gangrenous appendicitis as determined by imaging were enrolled [5]. Our database of 28 sites spanned the entire United States and included both urban and rural institutions, academic and nonacademic centers, and large and small institutions. The current study is a post-hoc subgroup analysis only of the data collected prospectively for acute, simple appendicitis (as diagnosed intra-operatively by the surgeon), excluding the perforated and gangrenous cases. Exclusion criteria for the original database included transfer from another institution and patient encounter outside the emergency department (ED) setting (i.e., inpatient consultation).
For this post-hoc subgroup analysis, subjects who underwent appendectomy for American Associations for the Surgery of Trauma (AAST) operative Grade I appendicitis were reviewed. The AAST intra-operative grade was assigned on the basis of a review of the operative report or direct contact with the surgeon (if the diagnosis was unclear from the report). This subgroup was divided into two groups: Those who received post-operative antibiotics (POST) and those who received pre-operative antibiotics only (NONE). The data analyzed included demographic information (age, sex, weight, current tobacco use), initial presentation (white blood cell [WBC] count and Alvarado score [8]), clinical outcomes at initial hospitalization (surgical site infection rate, intra-abdominal abscess rate, secondary interventions rate, and length of index hospitalization stay [LOS]), and clinical outcomes at 30 days after discharge (ED visit rate, hospital re-admission rate, surgical site infections (SSI) rate, intra-abdominal abscess [IAA] rate, and secondary interventions). Because of the observational nature of the study, subjects were not contacted after index hospitalization discharge, and therefore clinical outcomes were extracted from the electronic medical record. If the subject was not encountered after discharge, he or she was considered to be lost to follow up.
For this post-hoc analysis, statistical analysis was performed using Stata v 14.2. A p value <0.05 was considered statistically significant. Categorical values were tested for statistical significance using the χ2 test or Fisher exact text if counts were fewer than five subjects in a category. Continuous variables and ordinal variables were reported as medians [interquartile range], and comparisons were performed using the Wilcoxon rank sum test. Clinical outcomes were reported as frequencies and compared using the χ2 test.
Results
After exclusions, this analysis included a total of 2,191 subjects who underwent appendectomy and had operative findings that met the criteria for AAST Operative Grade I. Of these subjects, 612 (28%) received at least one dose of antibiotics post-operatively and comprised the POST subgroup. The remaining 1,579 subjects (72%) did not receive post-operative antibiotics and comprised the NONE subgroup. Table 1 shows the demographic characteristics of the POST and NONE groups. The POST group subjects were older, heavier, more likely to be current smokers, and to have a higher WBC count on admission than the NONE group. Of these differences between groups, age, weight, and admission WBC counts were significant. There were no differences in median Alvarado Score or Charlson Comorbidity Index of the two groups. There was no difference in antibiotic prescribing practices among participating sites.
Characteristics of Patients Receiving Post-Operative versus Pre-Operative Only Antibiotics in Simple Appendicitis
CCI = Charlson Comorbidity Index; NONE = pre-operative antibiotics only; POST = post-operative antibiotics given; WBC = white blood cells.
The only significant difference in index hospitalization outcomes of the two groups was LOS, reported in Table 2. In the POST group, the LOS was longer than in the NONE group (p < 0.001). The rate of SSI during index hospitalization was 0.2% in both groups.
Index Hospitalization Outcomes of Post-Operative versus Pre-Operative Only Antibiotic Administration in Simple Appendicitis
IAA = intra-abdominal abscess; LOS = hospital length of stay; NONE = pre-operative antibiotics only; POST = post-operative antibiotics given; SSI = surgical site infection.
At the 30-day follow-up period, 18.5% of the subjects in the POST group were lost to follow-up compared with 16.1% of the NONE group (p = 0.181). Analysis of these two cohorts showed that they were similar to their respective POST and NONE groups containing subjects not lost to follow-up. The clinical outcomes of the two groups were similar at 30 days as is shown in Table 3.
30-Day Outcomes in Patients Receiving Post-operative versus Pre-operative-Only Antibiotics in Simple Appendicitis
ED = emergency department; IAA = intra-abdominal infection; NONE = pre-operative-only antibiotics; POST = post-operative antibiotics given; SSI = surgical site infection.
The spectrum of post-operative antibiotic use was similar across all institutions. Roughly one-third of patients received post-operative antibiotics, with 386 patients (16.8%) receiving antibiotics for longer than 24 hours. The median duration of post-operative antibiotics was five days [4,8].
Great variability was observed between and within individual sites with respect to antibiotic choice. A total of 16 regimens were identified, with the most commonly prescribed antibiotics being piperacillin/tazobactam and metronidazole (Fig. 1). The prescription and duration of post-operative antibiotics was not limited to any regional trend or type of institution.
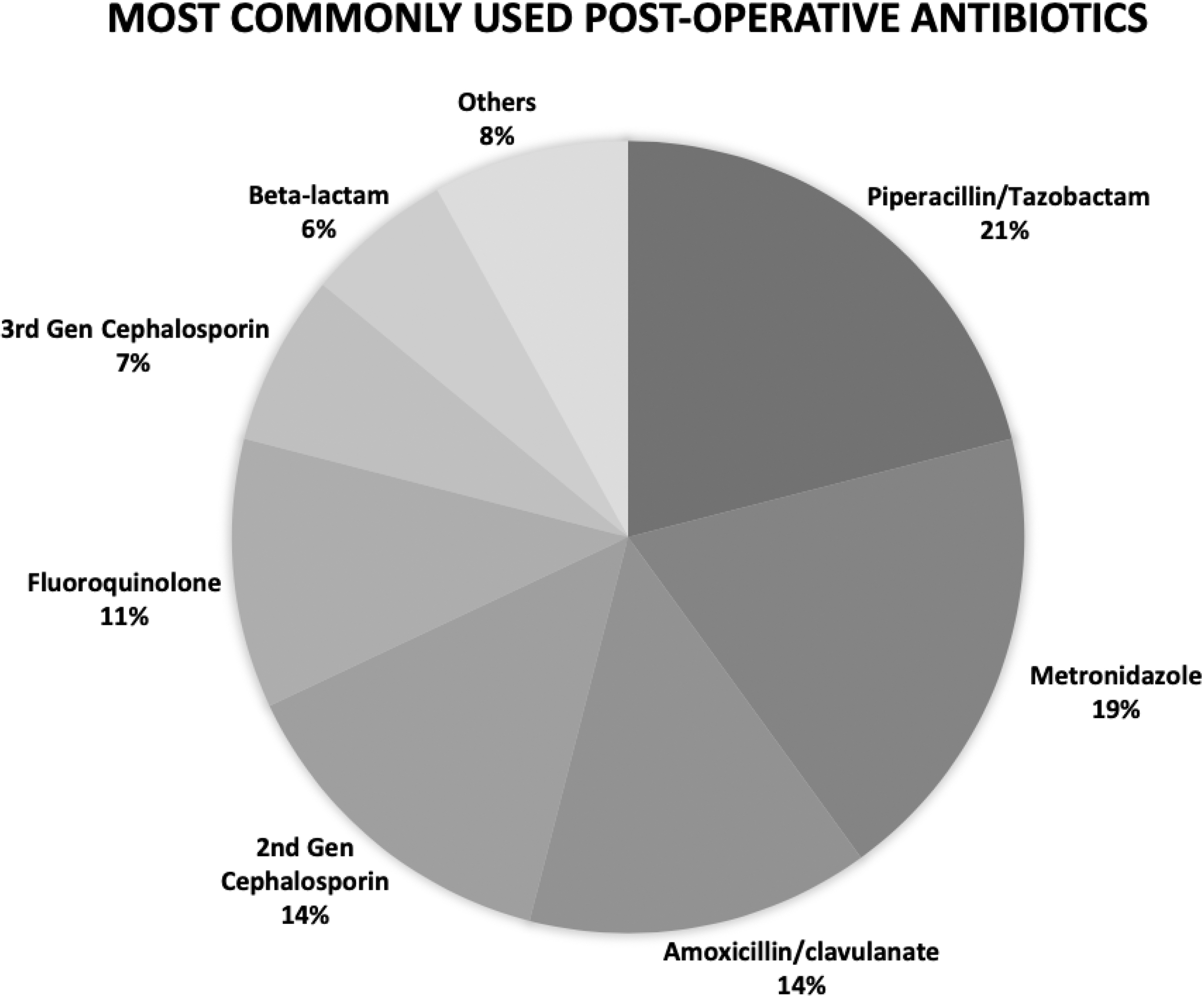
Antibiotics most commonly prescribed post-operatively in simple appendicitis.
Discussion
The management of acute simple appendicitis, AAST Grade I, continues to be largely operative in the United States. Multiple studies have identified the necessity of pre-operative antibiotic administration for appendicitis, regardless of presentation [9,10]. Intra-operative findings are good predictors of the need for post-operative antibiotic administration for perforated and gangrenous appendicitis. However, many surgeons continue to prescribe antibiotics of various classifications and durations post-operatively for AAST operative Grade I appendicitis, as shown in this multi-center observational study. Previous published case series, randomized controlled trials, and systematic reviews have advocated only pre-operative administration of antibiotics for non-perforated appendicitis [1,13-16]. Through this prospective observational study, we have shown that nearly one-third of patients with simple appendicitis continue to receive post-operative antibiotics, despite previous evidence and SIS Task Force Guidelines recommending otherwise. This observational study showed no difference in the rates of surgical site infections and intra-abdominal abscess formation during initial hospitalization and at 30-day evaluation in patients treated with and without post-operative antibiotics. We have demonstrated that the patients who receive these post-operative antibiotics tend to be older and of higher weight and to have a higher admission WBC count; this represents a potential selection bias. Unnecessary administration of antibiotics leads to more antibiotic-resistant infections and a greater risk of adverse events secondary to antibiotic use [17]. Furthermore, prolonged duration of antibiotics is an unnecessary burden to our patients and costly to our healthcare system. This snapshot of current practice highlights the need for surgical services to scrutinize their practices and improve compliance with society guidelines and evidence-based treatment. We advocate for improved adherence to such guidelines and encourage all surgical centers to review their own practices in evaluating room for improvement.
There are several limitations to this study that must be acknowledged. First, a selection bias exists for those patients who received post-operative antibiotics. The demographics are different leading to the choice for antibiotic administration. This also was a purely observational study with a waiver of informed consent at most of the institutions; therefore, we were unable to contact subjects after enrollment and relied on the electronic medical record for follow-up data. This resulted in approximately a 15% overall lost-to-follow-up rate, raising the possibility of selection bias in comparing outcomes in the two groups. However, this risk is mitigated by the fact that the rates of loss to follow-up were not significantly different in the two groups. Second, it is possible that patients were missed for enrollment at times when research staff were unavailable because of resource limitations at some sites. The strengths of our study include the large sample size and multi-center data collection. This post-hoc analysis highlights the current practice of U.S. physicians administering post-operative antibiotics to roughly one in three patients with simple appendicitis and was unable to detect clinically meaningful differences in complication rates. However, it should be kept in mind that the complication rate after appendectomy for simple appendicitis is so low that this epidemiologic study is not intended to be powered to detect a statistically significant difference in the rates. Large epidemiologic studies such as this provide snapshots of current practice trends and identify room for improvement in adherence to national guidelines.
Conclusions
In the United States, post-operative management of simple appendicitis is not uniform. We have shown that almost one- third of patients with simple appendicitis receive post-operative antibiotics, without evidence of, or association with, better clinical outcomes. Surgeons treating these patients should review their practices to improve adherence to recommended guidelines and refrain from overprescribing antibiotics for this cohort of patients.
EAST Appendicitis Study Group
Stacie L. Allmond, DO, Carilion Clinic; Reginald Alouidor, MD, FACS, Baystate Medical Center; Nadine Barth, MD, Cooper University Hospital; Brandon Behrens, MD, Oregon Health Sciences University; Matthew Bradley, MD, Walter Reed National Military Medical Center; Richard D. Catalano, MD, Loma Linda University; Morgan Collom, DO, Medical City Plano; Alexis L. Cralley, MD, Denver Health; Marie Crandall, MD, MPH, FACS, University of Florida, Jacksonville; Daniel C. Cullinane, MD, Marshfield Clinic; Chris Dodgion, MD, Medical College of Wisconsin; Savo Bou Zein Eddine, MD, Medical College of Wisconsin; Ahmed I. Eid, MD, Massachusetts General Hospital; Ahmed Elsayed Mohammed Elsharkawy, North Shore Medical Center; David C. Evans, MD, FACS, Ohio State University Wexner Medical Center; Steven Eyer, MD, FACS, Essentia Health; Rondi Gelbard, MD, Emory University; Ali Fuat Kann Gok, MD, University of Southern California; Kailyn Kwong Hing, MD, Baystate Medical Center; Lewis Jacobson, MD, St. Vincent Hospital Indianapolis; Bellal Joseph, MD, University of Arizona, Tuscon; Laura Juarez, PA-C, Intermountain Medical Center; Haytham M.A. Kaafarani MD, MPH, Massachusetts General Hospital; Tala Kana'an, MBBS, Mayo Clinic; George Kasotakis, MD, MPH, Boston Medical Center; Ryan A. Lawless, MD FACS, Denver Health; Elena Lita, BS, Inova Fairfax; Bruce Long, MD, Carilion Clinic; David Morris, MD, Intermountain Medical Center; Jennifer Mull, MSN, RN, CCRC, University of Florida, Jacksonville; Jeffry Nahmias, MD, MHPE, University of California, Irvine; Lindsay O'Meara, University of Maryland; Jason D. Pasley, DO, FACS, University of Maryland; Sean Perez, BS, Boston Medical Center; Victor Portillo, MD, Medical City Plano; Kaitlyn Proulx, PA, Essentia Health; Mohamed Ray-Zack, MD, Mayo Clinic; Jennifer C. Roberts, MD, Marshfield Clinic; Carlos Rodriguez, DO, Walter Reed National Military Medical Center; Janika San Roman, MPH, Cooper University Hospital; Jonathan Saxe, MD, St. Vincent Hospital Indianapolis; Martin Schreiber, MD, Oregon Health Sciences University; Thomas Serena, DO, Beaumont Hospital; Victoria Sharp, DO, Beaumont Hospital; Beatrice Sun, BS, University of California, Irvine; Crystal Szczepanski, MSN, NP-C, ACNP-BC, Emory University; Maryam B. Tabrizi, MD, North Shore Medical Center; Erik J. Teicher, MD, FACS, Inova Fairfax; Jocelyn To, BS, University of Southern California; David Turay, MD, PhD, Loma Linda University; Daniel E. Vazquez, MD, FACS, Ohio State University Wexner Medical Center; Jeffrey Wild, MD, FACS, Geisinger Medical Center; D. Dante Yeh, MD, Ryder Trauma Center; Katelyn A. Young, BS, Geisinger Medical Center; Muhammad Zeeshan, MD, University of Arizona, Tucson
Author Disclosure Statement
No competing financial interests exist.