
Abstract
Background:
Surgical site infections (SSI) are multifaceted. Pre-operative, intra-operative, and post-operative factors influence the risk of developing an infection. Our objective was to evaluate the effectiveness of an infection risk-stratification checklist, utilizing known SSI risk factors, and a tailored surgical protocol for SSI prevention in women undergoing cesarean delivery.
Patients and Methods:
A prospective project to reduce SSI was conducted for women undergoing cesarean delivery on the resident staff service at a midwestern, urban tertiary care hospital. Patients were categorized according to an SSI risk-stratification checklist as high risk or low risk. The low-risk group received the local standard of care (single prophylactic dose of pre-operative intravenous antibiotics and a standard pressure dressing). In the high-risk group, prophylactic antibiotic agents were given pre-operatively and continued for the first 24 hours post-operatively. Additionally, patients at high risk received an absorbent dressing (Mepilex Ag®; Mölnlycke Health Care AB, Gothenburg, Sweden) that was applied in the operating room and worn for one week.
Results:
The overall rate of SSIs decreased from 6.1% (pre-study rate) to 1.4% after initiation of the protocol, a 77% reduction (p < 0.001). The low- and high-risk groups did not differ in infection rate (0% and 1.4%, respectively; p < 0.59). Both deep incisional and organ/space SSIs decreased after initiation of the protocol (91% and 62% decrease, respectively).
Conclusion:
Stratifying patients into high- and low-risk groups with tailored peri-operative management strategies reduced overall SSIs. The protocol incorporates known risk factors for SSI in a surgical procedure with high rates of SSI. This approach offers a structured method that can be adopted by other hospital systems for SSI prevention in patients undergoing cesarean delivery.
Surgical site infections (SSIs) represent approximately 31% of all hospital-acquired infections [1]. The incidence of SSIs after cesarean delivery is 3%–15% with a maternal mortality rate of up to 3% [2]. Risk factors for SSI are multifaceted and include pre-operative (e.g., medical comorbidities, elevated body mass index [BMI], smoking status), intra-operative (e.g., length of surgery), and post-operative factors (e.g., incision care, medication compliance). Patients often have several discrete risks factors that cumulatively result in an increased risk of SSI, which makes a “one size fits all” prevention plan inadequate.
Cesarean delivery is a primary contributor to SSI rates, with a risk up to 20 times greater than other surgeries [3]. Risk factors for SSI among patients undergoing cesarean delivery include the presence of labor, stage of labor, presence of ruptured membranes, absence of antibiotic prophylaxis, length of surgery (>60 minutes), obesity (BMI >30 kg/m2), tobacco use, hypertension, and diabetes [4–8]. Moulton et al. [9] found that failure to progress in labor, high parity, earlier gestational age, longer operative time, and increasing BMI predicted SSIs with a 71% concordance, demonstrating the influence of multiple factors on the development of SSI.
Prophylactic pre-operative antibiotic agents are an accepted standard for SSI prevention [10–13]. Recently the use of extended spectrum agents and post-operative extended dosing have been shown to reduce SSI in high-risk patients such as those undergoing cesarean during labor or after rupture of membranes and in those who are obese (BMI >30) [14,15]. Other SSI prevention methods include the importance of full-body shower/bath with soap or antiseptic agent the night prior to surgery, maintaining glycemic control and normothermia during surgery, and pre-surgical preparation with povidone iodine or chlorhexidine alcohol [13,16–18].
The effectiveness of different surgical dressings for prevention of SSI has been assessed although definitive recommendations are lacking [19]. Silver-containing dressings have been shown to have instant and sustained antimicrobial activity in both scientific and clinical studies with Mepilex Ag® (Mölnlycke Health Care AB, Gothenburg, Sweden), specifically, providing superior antimicrobial activity compared with other commercially available dressings [20–24]. Silver-containing dressings have been shown to manage bioburden effectively in both acute and chronic wounds that are at increased risk of infection and have been recommended as adjunctive therapy with systemic antibiotic agents for infection prevention [25]. However, some randomized trials examining SSI have not shown a substantial reduction in infection when these dressings are compared with standard cloth dressing or no dressing, leading to their use being determined by provider and patient preference and cost [19]. Our approach to SSI prevention draws from the literature to acknowledge the effects of multiple factors on the development of SSIs and utilizes several methods in the protocol to minimize the influence of these factors. The objective of this study is to evaluate the use of an infection risk-stratification checklist to categorize women into high and low SSI risk groups and to provide a tailored protocol for perioperative care based on the level of risk. We predict that a protocol, tailored to address patients' risk for infection, will decrease SSI rates in women undergoing cesarean delivery.
Patients and Methods
This project was approved by the University Institutional Review Board. Female patients undergoing cesarean delivery between March 1, 2016 and February 28, 2017 on the obstetric staff service at a midwestern, urban tertiary care hospital were managed using the infection risk-stratification checklist and a tailored protocol.
Patients were evaluated according to the infection risk-stratification checklist developed for this project. This checklist consisted of risk factors associated with SSI identified in the literature [4-9]. Our interdisciplinary team evaluated the risk factors and classified each one as having a major or minor influence for the development of SSI based on team members' professional judgment (Table 1). The low-risk group criteria included absence of major risk factors and presence of zero or one minor risk factors. The high-risk group criteria included presence of one or more major risk factors or presence of two or more minor risk factors.
Major and Minor Risk Factors for Development of SSI
SSI = surgical site infection; BMI = body mass index; GA = gestational age; PROM = pre-mature rupture of membranes.
Care for all patients followed a three-step tailored surgical protocol that included a pre-operative surgical preparation bundle, standardized intra-operative surgical procedures, and the low-risk/high-risk tailored post-operative bundle (Fig. 1). Procedures for steps 1 and 2 were the institution's local standard at the time of this project and had been selected based on their demonstrated effectiveness in the literature [26]. Patients were evaluated using the infection risk-stratification checklist into HR or LR groups after step 2 in order to assign the tailored post-operative bundle for step 3 (Fig. 1).

Three-step protocol.
Cefotetan was chosen based on the recommendation from the Infection Prevention and Control Department (IPCD) for broad-spectrum antibiotic agents that would be effective against the bacteria historically seen in the local population who develop SSI after cesarean delivery. All patients received cefotetan (2 g intravenously) 30 to 60 minutes prior to incision. The high-risk group received an additional dose of cefotetan to provide 24-hour post-operative coverage (i.e., one post-operative dose at 12 hours after surgery). In the event of severe allergy to penicillin, low- and high-risk patients received pre-operative intravenous clindamycin (900 mg) and single-dose gentamicin (5 mg/kg), and high-risk patients received additional doses of clindamycin post-operatively to provide 24-hour coverage (i.e., two post-operative doses, one at eight hours after surgery and the second at 16 hours after surgery). The low-risk patients received standard dressing (Telfa™; Kendall Company, Mansfield, MA) that was removed after 24 hours, whereas the high-risk patients received an absorbent dressing (Mepilex Ag®) that was removed after seven days to maximize antibacterial effect [20,27].
The primary outcome was the development of SSI within 30 days of delivery. Surgical site infection was defined according to the U.S. Centers for Disease Control (CDC) and Infection National Healthcare Safety Network and included superficial incisional, deep incisional, and organ/space infections [28]. Patients were assessed for SSI in the hospital until discharge and in the outpatient clinic at regular post-operative visits. Standardized order-sets and operative and post-operative templates were used to enhance adherence to the protocol and appropriate data recording.
Data were obtained from the hospital electronic medical record and included demographic and health information, indication for cesarean delivery, maternal complications, and development of SSI. In cases in which patients presented to other hospitals for treatment of SSI, the delivering hospital's IPCD received notification of the SSI and provided the data to the investigators. The baseline SSI rate (6.1%) was provided by the IPCD for the obstetric staff service on labor and delivery for 2015–2016. The risk-stratification checklist was validated in a separate chart review study examining obstetric staff service patients who delivered in 2014 (n = 357). That study confirmed that when patients were assigned retrospectively to the low- and high-risk groups using the checklist, they were appropriately classified in that all SSIs occurred in the high-risk group (SSI rate was 6.3% in the high-risk group and 0% in the low-risk group) [29].
A priori sample size estimation indicated that 296 patients would be needed to detect a 50% reduction from the baseline SSI of 6.1%, using power = 80% and α < 0.05 criterion for statistical significance (G*Power, version 3.0.10, Universität Kiel, Germany). Data analysis, including Pearson χ2, Student t-test, and Fisher exact test, was performed using SPSS version 24.0 (IBM Corp, Armonk, NY). Significant associations were determined using p < 0.05.
Results
Three hundred sixty-five (365) patients were classified according to the infection risk-stratification checklist resulting in 75 patients in the low-risk group and 290 patients in the high-risk group. The groups did not differ on demographic characteristics with the exception of BMI, which was a criterion for high-risk group membership (low risk = 27.93 ± 6.59; high risk = 35.12 ± 8.45; p < 0.001). Groups did differ in the presence of major risk factors as expected (Table 2). By definition, those with BMI ≥30, insulin-controlled diabetes, prolonged rupture of membranes, an intra-amniotic infection, or those who labored were classified in the high-risk group. There were no differences in demographic and clinical characteristics, or for major and minor risk factors, among those who did versus those who did not develop SSI (Table 3).
Patient Characteristics and Risk Factors by Risk Group

BMI = body mass index.
Patient Characteristics and Risk Factors by Presence of SSI
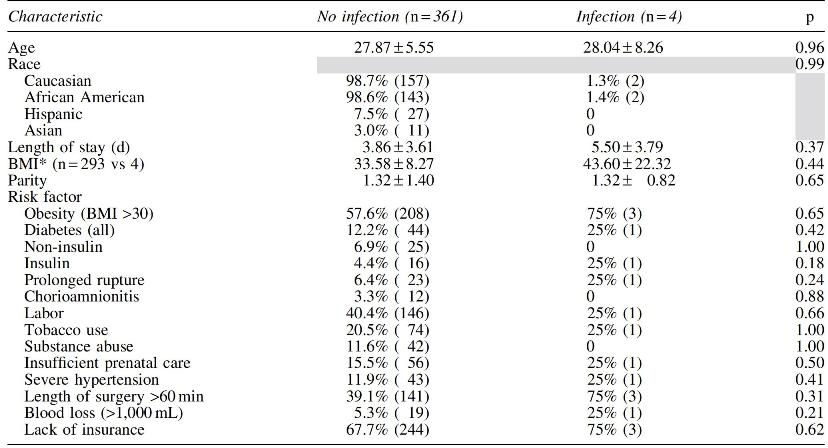
SSI = surgical site infection; BMI = body mass index.
Total percent of SSI decreased from 6.1% from the pre-intervention period to 1.4% after the intervention period (77% reduction; p < 0.001). As expected, all SSIs occurred in the HR group. Superficial incisional SSI occurred in 0.3% of patients (91% decrease from the pre-study rate of 3.5%), and deep incisional and organ/space SSI occurred in 0.3% (62% decrease from pre-study rate of 0.8%).
Discussion
Our goal was to determine the effectiveness of the SSI risk-stratification checklist and the tailored surgical protocol for reducing SSI in women undergoing cesarean delivery. The results of this project show a substantial decrease in SSI for HR patients after executing this approach.
These results suggest that the combination of these demonstrated methods for reducing SSI, i.e., extended antibiotic dosing such as that used by Valent et al. [15] and Tita et al. [14] and standardized surgical preparation and incision closure bundles such as that used by Kawakita et al. [26,30], effectively reduce SSI to a greater degree than reductions reported in the literature for these methods alone (58% in Valent et al. [15]; 64% in Tita et al. [14], and 52% in Kawakita et al. [26,30]) [31].
Stratification of patients according to level of risk replaces the “one size fits all” approach to SSI prevention and may represent a more cost-effective approach to SSI reduction. The infection risk-stratification checklist was verified with the 2014 chart review confirming that those who developed SSI met criteria for high-risk group inclusion and that no patient meeting criteria for low-risk group inclusion developed SSI. The tailored protocol was utilized to assign infection prevention methods according to patients' risk. Low-risk patients who are unlikely to develop SSI can be treated with the standard pre-incision antibiotic agents and standard dressing, providing an appropriate and low-cost protocol that fits their level of risk. High-risk patients were identified effectively and when managed with additional preventive measures, e.g., post-operative antibiotic agents and an absorbent dressing, had a substantially lower rate of SSI compared with baseline. Re-admissions for deep incisional and organ/space SSI were substantially lower after execution of this project, resulting in an estimated cost savings of approximately $50,000 for our hospital, based on cost per infection estimates from Olsen et al. [32].
The design of this study takes into account the multiple factors that place patients at higher risk for developing SSI. Key elements, e.g., risk factors, standardized techniques, and infection prevention methods, were selected from the literature and CDC guidelines for SSI prevention. Antibiotic agents were selected after consultation with the hospital IPCD to ensure that the bacteria seen in this population would be targeted appropriately. Additionally, this project was executed over a full year to reduce potential bias associated with known seasonal variability in infection rates [33]. The hospital IPCD worked closely with the research team to ensure that complete SSI data were gathered regardless of patient compliance with post-operative follow-up visits or facility in which their SSI was treated. The design elements used in this project add to the strength of this approach. The SSI risk-stratification checklist and the three-step tailored surgical protocol provide a clear process for SSI prevention that can be applied in other hospital systems and in other surgical specialties.
The objective of this project was to reduce SSI in patients undergoing cesarean delivery. It was our intention to include multiple procedures that are known to reduce infection to achieve the goal of reduced SSI. However, by doing this, the individual effectiveness of the procedures, i.e., antibiotic extended dosing, pre-operative preparation procedures, intra-operative procedures, and dressing type, cannot be determined and is recognized as a limitation of this study. We also acknowledge that the risk-stratification checklist treats the identified risk factors equally in terms of their influence on SSI. We attempted to address this limitation by categorizing risk factors as major or minor according to our professional judgement of their potential impact on SSI. We noted that 79% of our population was classified into the high-risk group. It is possible that patients are being overclassified, i.e., those who are really at low risk are being classified in the high-risk group because the criteria are too liberal. The more liberal use of the high-risk classification and its longer duration of antibiotic use could pose an increased risk for developing antibiotic resistance among the commonly encountered pathogens and Clostridioides difficile infection. Although we did not note any of these events, this is an important reason for continuing to evaluate the factors that place individuals in the high-risk group.
More research is needed to validate the risk factors for the high-risk group to ensure that only those factors that are strong predictors of SSI will be included in the checklist. We noted that none of the patients with chorioamnionitis developed SSI, however, this may be because of the additional treatment they received as a result of this diagnosis (i.e., ampicillin, gentamicin, and clindamycin per American College of Obstetricians and Gynecologists guidelines) instead of the post-operative antibiotics used in the high-risk protocol. It is possible that this risk factor represents a separate group that should be removed from the checklist and treated differently because it represents an existing infection that would not be appropriate to manage with an infection prevention protocol such as ours.
There may also be a benefit for adding the absorbent dressing to current antibiotic protocols as some have suggested [25]. However, there is little information in the literature to determine the additional impact of dressings used this way [34–36]. This project was not designed to determine the separate effectiveness of antibiotic use and dressing type. Further research is needed to investigate the individual and combined effects of these methods.
Conclusions
We have demonstrated that there may be a benefit to stratifying patients into LR and HR groups according to their risk for developing SSI using an infection risk-stratification checklist. We have also shown that a multifaceted tailored peri-operative protocol reduces SSI in women undergoing cesarean delivery who are at high risk for developing infection.
Footnotes
Acknowledgments
This project was presented as a Poster at the American College of Obstetricians and Gynecologist (ACOG) 2018 Annual Clinical and Scientific Meeting, Austin, Texas, April 27–30, 2018.
Author Disclosure Statement
No competing financial interests exist.