
Abstract
Background:
Delayed treatment of seriously infected patients results in increased mortality. However, antimicrobial therapy for the initial 24 to 48 hours is mostly empirically provided, without evidence regarding the causative pathogen. Whether empiric anti-enterococcal therapy should be administered to treat intra-abdominal infection (IAI) before obtaining culture results remains unknown. We performed a meta-analysis to explore the effects of empiric enterococci covered antibiotic therapy in IAI and the risk factors for enterococcal infection in IAI.
Methods:
We searched multiple databases systematically and included 23 randomized controlled trials (RCTs) and 13 observational studies. The quality of included studies was assessed, and the reporting bias was evaluated. Meta-analysis was performed using random effects or fixed effects models according to the heterogeneity. The risk ratio (RR), odds ratio (OR), and 95% confidence interval (CI) were calculated.
Results:
Enterococci-covered antibiotic regimens provided no improvement in treatment success compared with control regimens (RR, 0.99; 95% CI, 0.97–1.00; p = 0.15), with similar mortality and adverse effects in both arms. Basic characteristic analysis revealed that most of the enrolled patients with IAI in RCTs were young, lower risk community-acquired intra-abdominal infection (CA-IAI) patients with a relatively low APACHE II score. Interestingly, risk factor screening revealed that malignancy, corticosteroid use, operation, any antibiotic treatment, admission to intensive care unit (ICU), and indwelling urinary catheter could predispose the patients with IAI to a substantially higher risk of enterococcal infection. “Hospital acquired” itself was a risk factor (OR, 2.81; 95% CI, 2.34–3.39; p < 0.001).
Conclusion:
It is unnecessary to use additional agents empirically to specifically provide anti-enterococcal coverage for the management of CA-IAI in lower risk patients without evidence of causative pathogen, and risk factors can increase the risk of enterococcal infection. Thus, there is a rationale for providing empiric anti-enterococcal coverage for severely ill patients with CA-IAI with high risk factors and patients with hospital-acquired intra-abdominal infection (HA-IAI).
The correct management of intra-abdominal infection (IAI) involves expeditious diagnosis, initial resuscitation of the patient, source control, and antimicrobial therapy [1]. Antimicrobial therapy for the initial 24 to 48 hours is provided mostly empirically, without any evidence regarding the causative pathogen or its susceptibilities. It is substantially different from pathogen-directed therapy, which is based on the result of bacterial culture. Conventional wisdom states that appropriate empiric antibiotic treatment that matches the in vitro susceptibilities of the isolated pathogens increases efficacy and reduces mortality [2]. Physicians thus strive to achieve the appropriate empiric antimicrobial therapy for inpatients with suspected infections; consequently, the duration of antibiotic therapy for patients hospitalized with confirmed or suspected infections often exceeds the recommended lengths of treatment [3,4]. The resulting overuse of antibiotic agents is a key driver for the emergence of antibiotic-resistant bacteria and leads to potentially avoidable adverse drug events [5].
However, inadequate or delayed antimicrobial therapy has been associated with higher deaths in patients with sepsis and septic shock from any source [2,6]. Several studies have also demonstrated an association of inadequate antimicrobial therapy with poorer outcomes in patients with IAI [6–8]. Therefore, antibiotic regimens should be rational and effective.
Enterococci are common opportunistic micro-organisms that are isolated increasingly from patients with IAI, with a high percentage of up to 32.02% being reported [9]. A few observational studies have suggested that the failure to treat seriously ill patients infected with micro-organisms such as Enterococcus spp. results in increased mortality [10–12]. However, Enterococcus is not covered routinely and is resistant to the established principle of antimicrobial therapy for patients with IAI, which involves the administration of agents with activity against gram-negative Enterobacteriaceae, aerobic streptococci, and obligate enteric anaerobes [13,14]; there also comes antibiotic-resistant enterococcus, such as vancomycin-resistant enterococci (VRE) [15]. Furthermore, there are no consistent opinions on whether timely anti-enterococcal therapy improves outcomes in patients infected with enterococci [16–19]. Moreover, the variable basic physical conditions of patients with IAI and infection sources usually result in diverse incidences of enterococcal infection [20]. Therefore, in addition to whether empirically enterococci-covered antibiotic therapy should be administered to patients with IAI even when the pathogen culture result is not available, we also considered when these antibiotic therapies should be administered.
As these problems continue to threaten current treatments, it is important to form a reasonable therapeutic strategy; thus, we conducted a systematic review and meta-analysis to investigate whether empiric enterococci-covered antibiotic therapy should be administered to patients with IAI prior to pathogen-directed therapy and to screen the risk factors for enterococcal infection in patients with IAI.
Materials and Methods
Eligibility criteria
This study was approved by the Institutional Review Board of First Affiliated Hospital, Zhejiang University School of Medicine. All randomized controlled trials (RCTs) and observational studies that enrolled patients diagnosed with IAI were considered for inclusion. Trials comparing the treatment success of IAI between patients receiving enterococci-covered antibiotic regimens and those receiving an antibiotic regimen without enterococcal coverage were eligible. Case control and cohort studies with the data comparing the risk factors between positive and negative enterococcal culture in patients with IAI were also eligible.
Search strategy
The search and screening procedures followed the Quality of Reporting of Meta-Analyses Criteria [21]. In brief, two authors independently performed a systematic search of several databases, including the Cochrane Library, MEDLINE, Embase, Central, Web of Science, Chinese National Knowledge Infrastructure (CNKI), WANFANG DATA, VIP Database for Chinese Technical Periodicals, and Sinomed (CBM), from January 1, 1990 to October 31, 2019 without language restrictions. Additionally, the ClinicalTrials.gov website was searched for relevant trials.
Previous systematic reviews and meta-analyses as well as the references associated with these studies were also searched manually. Keywords and medical subject headings used in the search included (but were not limited to): “intra-abdominal infection,” “intra-abdominal sepsis,” “appendicitis,” “diverticulitis,” “peritonitis,” “typhlitis,” “peritonitis tuberculous,” or “subphrenic abscess” for the identification of IAI; “Enterococcus/cci/ccal” for the identification of Enterococcus; and “antibacterial agents,” “antibacterial compounds,” “bactericidal agents,” “bactericides,” “antibiotic,” “anti-infective agents,” or “antimicrobial therapy” for the identification of antibiotics. A complete search strategy, including all keywords, is provided in the supplementary material.
Study selection and data extraction
Two authors independently screened titles and abstracts and subsequently analyzed the full text of all the studies that passed the abstract screening. An arbitrator dealt with any discrepancies that arose. The primary outcome for the meta-analysis of RCTs was treatment success, and secondary outcomes included mortality and adverse effects.
Furthermore, two authors independently extracted data from the included studies pertaining to the participant characteristics, intervention and control antibiotic regimens, treatment success, and other factors using a standardized form. Another author checked the data and resolved any disagreements.
Study quality assessment
We applied the Cochrane risk of bias tool [22] to assess the study quality of RCTs and the Newcastle-Ottawa scale (NOS) [23] for observational studies. Publication bias was assessed using funnel plots.
Data pooling and statistical analysis
In total, 36 studies that included a total of 20,110 patients were analyzed. The pooling of estimates of overall effects was conducted using Review Manager software (RevMan, version 5.3, The Cochrane Collaboration, Denmark). Results were presented as risk ratio (RR) or odds ratio (OR), as appropriate. A random effects model was used if clinical heterogeneity was present and a fixed effects model was used if there was no clinical heterogeneity. Statistical heterogeneity was evaluated using the Q and I2 statistics. A p value >0.05 with I2 <50% indicated no heterogeneity. Data were presented with a 95% confidence interval (CI). Subgroup analyses were mainly based on the antibiotic regimen.
Definitions and abbreviations are as follow: ITT, intention to treat, subjects randomized; mITT, modified intention to treat, subjects who received at least one dose of the study drug; c-mITT, clinical modified intention to treat, subjects in the mITT population who met the minimal disease criteria; CE, clinically evaluable, subjects in the c-mITT population who met all the inclusion/exclusion criteria and had a clinical response of either a cure or failure at the test of cure (TOC) visit, eight to 44 days after the last dose of the study drug.
Minimal disease criteria at the time of diagnosis included the presence of either fever, defined as temperature ≥38.0°C/100.4°F; hypothermia, defined as temperature <35.5°C/95.9°F; leukocytosis, defined as white blood cell (WBC) count >10,000/mm3; or leukopenia, defined as WBC count <5,000/mm3 or >10% immature (band) forms. In addition, at least two of the following findings were required to be present: localized or diffuse abdominal wall rigidity or involuntary guarding; abdominal tenderness or pain; nausea, vomiting, or ileus; radiographic, scintigraphic, sonographic, computed tomography, or magnetic resonance imaging studies suggesting a perforated viscus; an intra-abdominal abscess; or other focus of IAI.
Results
Study identification
The primary search resulted in 3,091 records, whereas 21 additional records were identified through manual searching of previous systematic reviews and meta-analyses as well as the references associated with these studies (Fig. 1). In total, 2,512 non-duplicated titles and abstracts were retrieved and 128 articles were acquired for full-text screening. Finally, 23 RCTs with a total of 9,681 participants were included in the meta-analysis of empiric anti-enterococcal treatment for patients with IAI and another 13 observational studies with 10,429 participants were included in the meta-analysis of assessment of risk factors for enterococcal infection in patients with IAI.
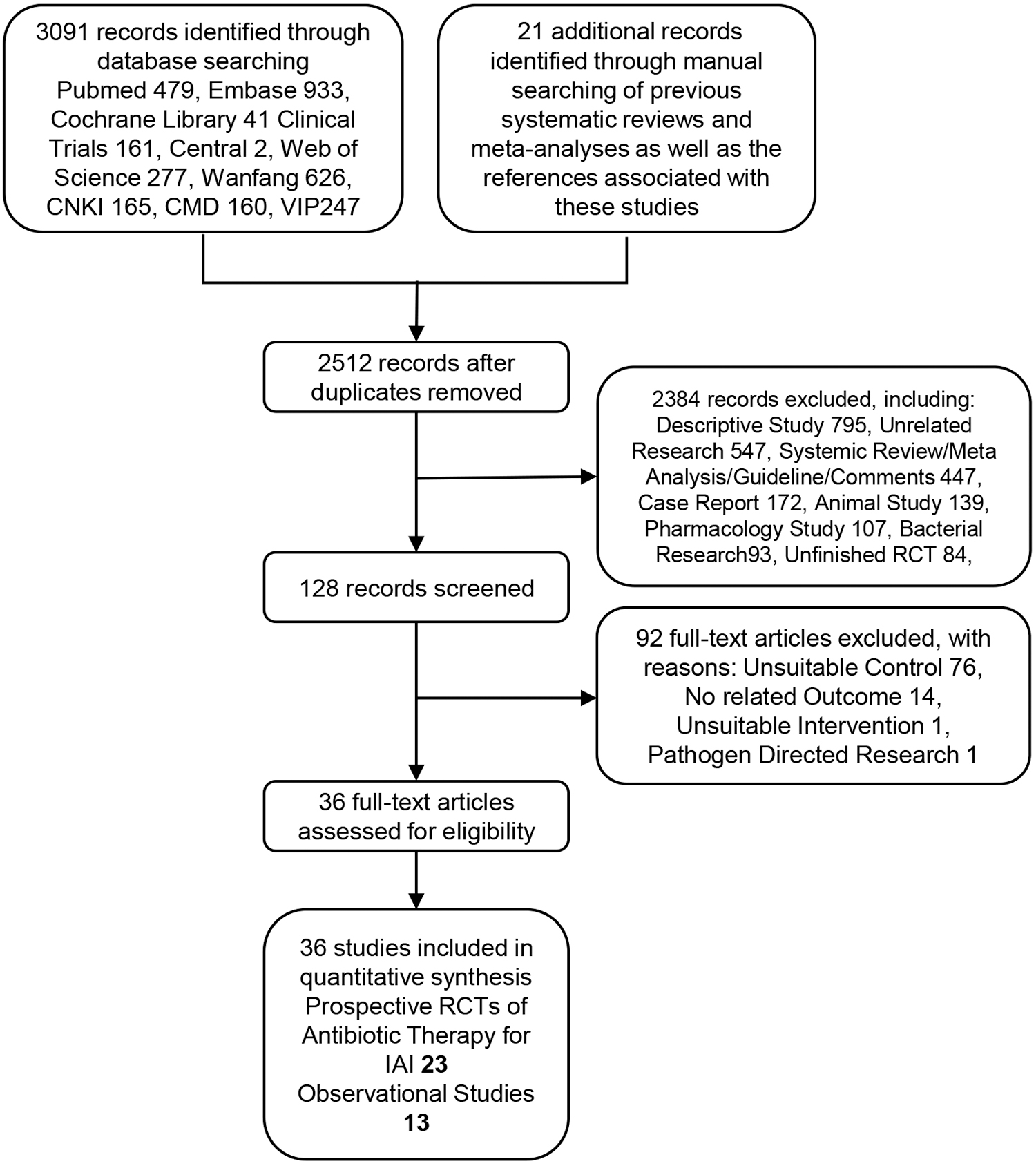
Study flowchart of the literature search.
Characteristics of included studies
The characteristics of all RCTs to assay empiric enterococci-covered antibiotic therapy are documented in Table 1. Data were obtained from trials performed in 48 countries; as the geographic map shows, the participant geographic distribution covers most developed and developing countries from five continents (Supplementary Fig. S1). Most of the included population consisted of adults, but two studies [29,32] recruited children as participants. The agents that were included in the enterococci-covered category were piperacillin-tazobactam in seven studies, meropenem in five, moxifloxacin in three, imipenem/cilastatin in two, eravacycline in two, tigecycline in two, and ampicillin/sulbactam in two. The primary characteristics of the enrolled patients, including ages, APACHE II scores, and baseline percentages of enterococci, are listed in Supplementary Table S1.
Characteristics of Twenty-Three Included RCT Studies
MC = multicenter; DB = double-blind; RCT = randomized controlled trial; IAI = intra-abdominal infection; c-IAI = complicated intra-abdominal infection; IV = intravenous.
The characteristics of the observational studies are detailed in Table 2. Most research was conducted in Europe, North America, and Asia. Of these studies, 11 were case control or cohort studies, whereas the remaining two were RCTs. Data pertaining to Enterococcus-infected cases, Enterococcus-negative controls, and their exposures were extracted from the embedded descriptions.
Characteristics of Thirteen Included Observational Studies
Case and control data extracted from RCT studies
c-IAI = complicated intra-abdominal infection.
Study quality
Of the 23 RCTs studied, all were declared as randomized controlled, 22 were multi-centered, and 18 were double-blind. However, eight studies failed to mention the sequence generation methods and six studies did not report the allocation concealment methods. The quality assessments of the included studies are shown in Supplementary Table S2 and Supplementary Fig. S2. Generally, it is acceptable that most studies showed a low risk according to the items of selection bias, performance bias, attrition bias, and reporting bias, except for detection bias. A funnel plot was drawn to assess the risk of reporting bias for pooled estimates, and the result of “Treatment Success based on CE Patients” (Supplementary Fig. S3) was symmetrical, suggesting a low risk of reporting bias.
For the 13 observational studies, the mean quality score assessed by NOS was 7.38 (range, 6–8), as detailed in Supplemental Table 3; this indicated the high quality of the observational studies in the meta-analysis. All the assayed risk factors, except for nosocomial infection, showed a good performance in funnel plot analysis (Fig. 3). When we removed the influencing study by Kang et al. [56], the funnel plots became symmetrical, and this omission did not change the role of nosocomial infection as a risk factor for enterococcal infection.
Analysis of Effectiveness, Mortality, and Adverse Effect of Empiric Enterococcus Covered Antibiotic Therapy versus Enterococcus Non-Covered Antibiotic Therapy
ITT = intention to treat; mITT = modified intention to treat; CE = clinically evaluable.
Meta-analysis
Empiric coverage for enterococci in antibiotic therapy for patients with IAI
Treatment success
The primary analysis of treatment success in CE patients included 17 studies and revealed no difference between enterococci-covered antibiotic therapy and antibiotic therapy without enterococcal coverage (RR, 0.99; 95% CI, 0.97–1.00; p = 0.15) (Fig. 2 and Table 3). When only the adult population was analyzed, a similar insignificant result was obtained (Table 3). In the subgroup analysis, moxifloxacin yielded a positive result (RR, 0.95; 95% CI, 0.92–0.99; p = 0.005), which favored antibiotic therapy without enterococcal coverage; however, the credibility of the evidence was limited because it was based on few studies. Furthermore, other treatment successes based on the indicated population were all nonsignificant.
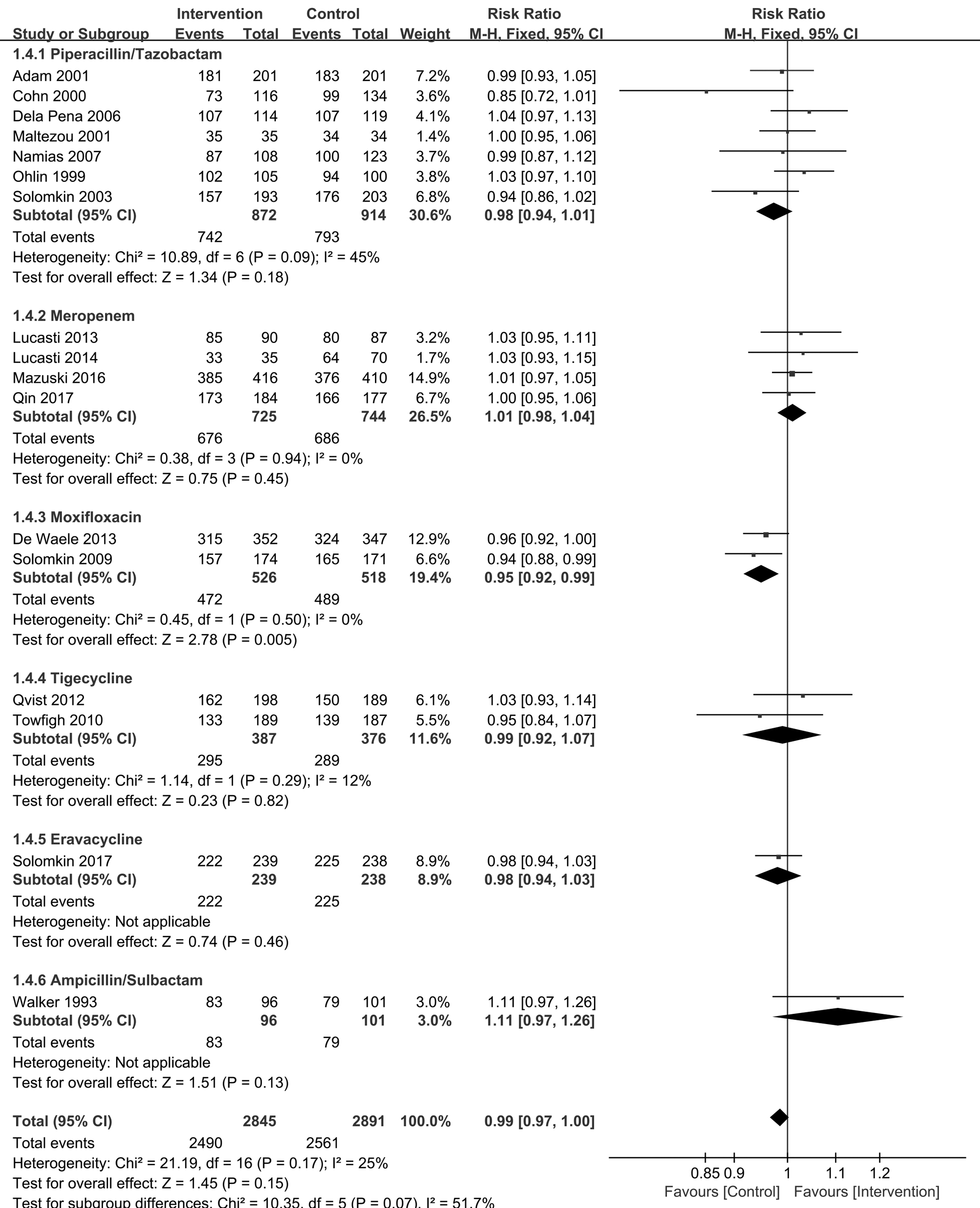
Forest plots showing treatment success based on clinically evaluable patients.
We also attempted to separate patients according to APACHE II scores to test whether our results were generalizable to all or relevant to only one and whether enterococci-covered antibiotic therapy could result in improved treatment success in higher risk patients; however, the outcomes were negative (Table 3).
Mortality and adverse effects
The mortalities based on mITT in the enterococci-covered antibiotic therapy group and the uncovered group were 2.66% and 2.47%, respectively, and there was no substantial difference (Table 3). The incidences of adverse effects were also the same between these two groups, accounting for 45.65% and 44.70%, respectively, in each group, based on the mITT population. However, we did not analyze the detailed adverse effects, which were restricted by the limited data available.
Risk factors for enterococcal infection in IAI
Considering that the meta-analysis of RCTs did not result in a positive outcome, we attempted to investigate the risk factors for enterococcal infection in patients with IAI. On the basis of the included studies, we selected 12 community-acquired factors and 10 hospital- or health-care–acquired factors for screening. These factors were not thoroughly distinguished from each other, because community-acquired factors could certainly be acquired in the hospital. Interestingly, we found that malignancy (Fig. 3A), corticosteroid use (Fig. 3A), operation (Fig. 3B), nosocomial infection (Fig. 3B), any antibiotic treatment (Fig. 3B), admission to ICU (Fig. 3B), and indwelling urinary catheter (Fig. 3B) could significantly increase the risk of enterococcal infection in patients with IAI (Table 4).
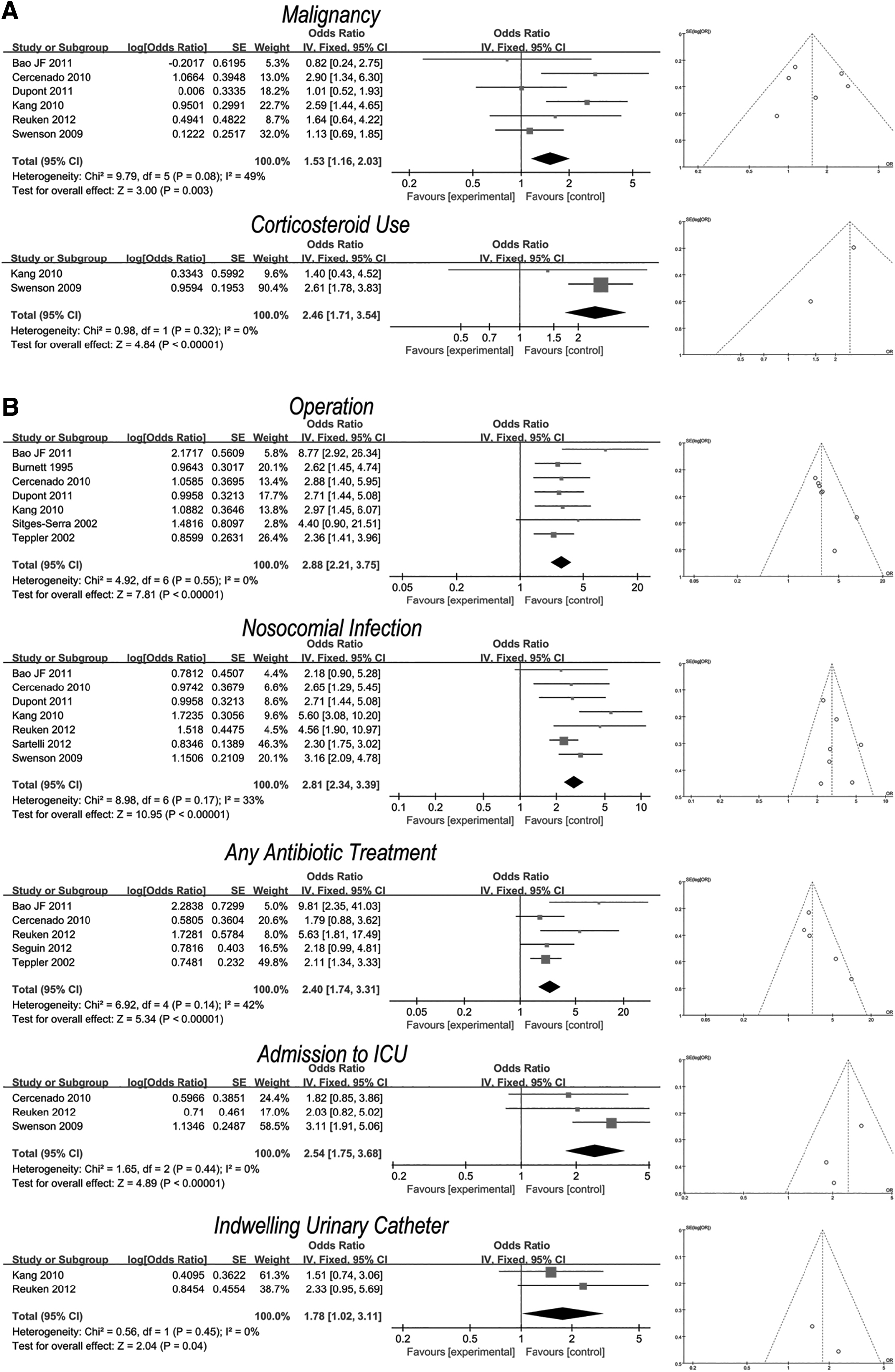
Forest plots and funnel plots of observational studies for assessing
Risk Factor Analysis for Enterococcal Infection in IAI
Discussion
The objective of this study was to evaluate broadly the available evidence regarding whether empiric anti-enterococcal therapy should be timely administered to patients with IAI before acquiring any evidence regarding the causative pathogen, building on previous nonsystematic overviews and systematic reviews of selected applications. The principal findings of this review were that for the included patients with IAI, enterococci-covered antibiotic regimens did not provide any better treatment success than antibiotic regimens without enterococcal coverage, with similar adverse events and mortality; this result was consistent across all the subgroups. For enterococcal infection in patients with IAI, malignancy and corticosteroid use were the associated community-acquired risks, while nosocomial infection, operation, any antibiotic treatment, indwelling urinary catheter, and admission to ICU were the associated hospital-acquired risks; the community-acquired risks were also the risks for inpatients.
Interestingly, we noted similar success between enterococci-covered antibiotic regimens and antibiotic regimens without enterococcal coverage in patients with IAI. As the results show, it indeed favors strongly studies in which the treatment failed and the results for which anti-enterococcal therapy was unnecessary. There are several possible explanations for the finding that all the study results were genuinely negative. The included patients with IAI were probably at a relatively lower risk of enterococcal infection (Supplementary Table S1). After analyzing the baseline pathogens sampled before antibiotic administration further, we found that the percentage of enterococcal infection ranged from 2.82% to 32.02%, with most below 20.0%. Most of the isolated pathogenic bacteria were gram negative. Thus, even though the intervention antibiotic regimen exerted positive functional effects on enterococcal eradication, it might not result in a striking clinically successful cure because enterococci were not predominant. Moreover, most of the included patients were young and were in good health, with mean ages ranging from 35.7 to 55.4 years after excluding children, and mean APACHE II scores ranging from 3.8 to 9.6. The percentage of patients with APACHE II scores <10 ranged from 70.44% to 97.4%. These factors predisposed most of the enrolled patients with IAI into a lower risk condition [1]. Furthermore, most of the enrolled patients were identified as community-acquired IAI (CA-IAI). It seems likely that there were higher risk patients in this heterogeneous population who might be more susceptible to enterococcal infections. As shown in Supplemental Table S1, the four RCTs [30,43,45] with the highest rates of enterococcal infection also harbored the highest APACHE II scores or the oldest age. In addition, we believe that positive results are more readily published. Thus, studies with negative results should be given credence.
In this regard, we further performed subgroup analysis separated by APACHE II scores with the limited explored data. Unfortunately, the results were not significant and limited by few studies that reported separated data according to APACHE II scores. Additionally, a score of 10 was not necessarily the optimal cutoff, as it was reported that an APACHE II score >12 (p = 0.04) was identified as an independent factor for post-operative enterococcal infection in patients with complicated intra-abdominal sepsis [24]. Thus, a significant number of studies with more available parameters to divide enrolled patients into subgroups is needed urgently to confirm the effects of enterococci-covered antibiotic therapy further on higher risk patients with IAI who are supposedly more likely to be infected with enterococci.
In IAI, enterococci accounted for up to 32.02% of the isolated bacteria [9]. Unfortunately, no threshold exists regarding how many risk factors constitute a sufficiently high prevalence rate to justify the use of empiric anti-enterococcal therapy. Thus, the identification of patients at risk for enterococcal infection is crucial to the early adaptation of antibiotic treatment. Operation and nosocomial infection were confirmed as risk factors for enterococcal infection in our study; this finding is consistent with the finding of Zhang et al. [12] and Jannasch et al. [11] research as well as the actual clinical situation. The proportion of enterococcal isolation was two- to fivefold higher in the hospital-acquired IAI (HA-IAI) group than in the CA-IAI group [24–26]. As we know, operation-induced trauma can injure the intestinal barrier and disturb the gut flora and long-term broad-spectrum antimicrobial therapy in hospitals can kill the commensal microbiota, both of which can lead to the overgrowth of opportunistic pathogens such as enterococci. Anastomotic injury is reported to induce substantial changes in the anastomotic tissue-associated microbiota, with the most striking difference reported to be a 500-fold increase in the relative enterococcal abundance [27]. Other identified risk factors have also established a positive relation between exposures and enterococcal infections, further providing insight into how the biologic mechanisms of enterococcal infections are affected by risk factors that predispose patients with compromised immunologic functions, disturbed gut flora, weakened barrier leakage, or even systemic failure. In agreement with the aforementioned results, hospitals seemed to have more risk factors. Considering community-acquired risk factors could also be acquired in the hospital, HA-IAI was more dangerous than the counterpart, as confirmed by the OR of 2.81 for nosocomial infection to increase enterococcal infection. Unfortunately, we did not examine the roles of age or APACHE II scores in the meta-analysis of observational studies because we had no access to the detailed dichotomous data of these two parameters.
Our study had a large population and wide geographic variation, ensuring great precision and high statistical power of the results. Moreover, detailed subgroup analyses and publication bias analyses were conducted to evaluate the robustness of the pooled risk estimates, which reinforced the stability and reliability of the findings.
Potential limitations of our study should be noted. Different regimens had different antibacterial spectra, especially against gram-negative Enterobacteriaceae, which comprised the majority of causative organisms [28], and we were even unable to balance the difference in the infectious bacteria between these two groups.
Conclusions
In summary, our review found sufficient evidence to conclude that the use of additional agents to provide anti-enterococcal coverage specifically in the management of CA-IAI in lower risk patients is unnecessary. Moreover, risk factors including community-acquired and hospital-acquired ones can increase the risk of enterococcal infection. Thus, there exists a sound rationale for providing empiric anti-enterococcal coverage in seriously ill patients with CA-IAI and HA-IAI, and a detailed regimen should be considered according to the local epidemiology, adverse effects, drug coverage, and other factors. This generalized conclusion likely obscures heterogeneity in effectiveness among patients and antibiotics or blended formulations. Future studies should assess these factors much more explicitly to refine our understanding of empiric anti-enterococcal therapy for patients with IAI.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.