
Abstract
Background:
In past decades, surgical site infections (SSIs) were neglected and not given much global attention in low- and middle-income countries (LMICs). The risk and incidence of SSIs in LMICs continue to increase.
Methods:
We reviewed the limited quality data on SSIs and complicated intra-abdominal infections in these settings that have hampered advocacy and infection prevention and control efforts.
Results:
This review identifies the rising profile of global surgery that has resulted in efforts to scale up access to surgical care as well as increase surgical volumes to address unmet needs. The fallout of these efforts would be increasing SSI rates and a rising volume of laparotomies for intra-abdominal infections.
Conclusion:
Surgical infections are an emerging frontier in global health and surgery. There is an urgent need for global advocacy and investments in their prevention and control.
Although geographical disparities exist, infections necessitating surgery are prevalent globally. The rising interest in surgical care has created a unique window of opportunity for advocates to emphasize existing global inequities. Until recently, there has not been much focus on surgical infections in most low- and middle-income countries (LMICs) [1]. A thorough assessment of the burden of surgical infections in these countries is lacking, and the spectrum and profile are poorly defined [2]. Some of the reasons for this neglect are:
Lack of high-quality reliable data makes it difficult to plan any effective prevention and control programs as well as to provide high-quality evidence-based care [2–4]; Poor advocacy: There has not been much high-level global advocacy focused on surgical infections [5]; Limited involvement of surgeons in advocacy as well as prevention and control programs; Little awareness of the devastating impact of surgical infection by policy makers, a direct fallout of the poor advocacy efforts; Assumption that infection is inevitable in LMICs; Complacency by surgical providers regarding surgical site infections (SSIs).
The Changing Global Surgery Terrain
In 2014–2015, the work of the Lancet Commission on Global Surgery (LCoGS) [6] indicated that five billion of the world's seven billion inhabitants did not have access to emergency and essential surgical care when needed. Further, the majority of these persons live in LMICs, and many families are driven into poverty by surgical operations. Follow-up work by the Global Initiative for Children's Surgery (GICS) [7] found that 1.7 billion children worldwide, mostly in LMICs, lacked access to emergency and essential surgical care (Fig. 1).

Lack of access to timely and safe surgical care with financial risk protection.
World Health Assembly Resolution 68:15
Following the work of the LCoGS, publication of the disease control priorities on surgical care (DCP3) [8], as well as advocacy from several countries and global surgery experts and organizations, the World Health Assembly (WHA) passed a resolution in May 2015 mandating that member countries strengthen emergency and essential surgical care and anesthesia as a component of universal health coverage [9]. In response to the resolution, several LMICs have either completed or initiated the creation of national surgical, obstetrics, and anesthesia plans (NSOAP) to expand access to surgical care in their settings. These activities and timing provide a unique window of opportunity to begin to address surgical infections on a global scale.
Global Burden of Surgical Infections
Surgical infections form a significant proportion of the global burden of disease. Complicated intra-abdominal infections, soft tissue infections, and SSIs make up a significant percentage of these infections in LMICs [10]. According to DCP3, appendicitis was the only surgical infection considered in the burden of conditions addressed by essential surgery in LMICs. That report estimated that 26,286 deaths from appendicitis could be prevented if basic surgical care could be provided, translating to about 1.15 million disability-adjusted life-years (DALYs) averted per year. This gives some idea of the burden of surgical infections in these settings and the role and impact of providing appropriate surgical care.
Burden of SSIs in LMICs
Although there are single-institution reports on the burden of SSI in LMICs, more comprehensive and more generalizable reports are lacking, and reports focusing on district (first-level) hospitals where the burden is potentially highest are rare. Hence, the true burden of SSI in these settings remains unknown or underestimated. One recent report focused on SSI after gastrointestinal surgery in 343 hospitals in 66 countries [1]. In that report, the SSI rates in countries with high human development index (HDI), middle HDI, and low HDI were 9.4%, 14.0%, and 23.2%, respectively. Even after adjusting for risk factors, low-HDI countries had the greatest risk of SSI. In another report from developing countries [11], SSI was the leading cause of hospital-associated infections (HAI) at 27% and a cumulative incidence of 5.6 per 100 surgical procedures. Others have reported SSI rates of 4.3%–60.4% in Africa compared with other parts of the world (Table 1) [12–21]. Even among LMICs, sub-Saharan Africa (SSA) appears to bear the greatest burden (Table 2), with rates as high as 21% even for clean surgical procedures (Table 3). Further, SSIs have been reported to prolong hospital stays in SSA [22]. In children, a high SSI rate of 23.6% has been reported, with a significantly higher mortality rate of 10.5% compared with 4.1% in those without SSI (p < 0.05) [23].
Global Surgical Site Infection (SSI) Rates a
Methods differ, and it is difficult to compare rates.
Surgical Site Infection (SSI) Rates in Africa*
Methods differ, and it is difficult to compare rates.
Reported Surgical Site Infection (SSI) Rates in Nigeria Compared with Expected Standard
High SSI rate for clean surgical wounds may be indication of serious limitations in infection prevention and control activities.
Although the risk factors for SSI in high-income countries (HICs) exist in SSA, additional factors that make SSI more likely in the setting have been identified [24-34] (Table 4). A particularly worrisome problem is gaps in the provision of basic operating room (OR) supplies, which could differ even on the same day in the OR and from one scheduled operation to another (Fig. 2). To compound the challenge of high SSI rates in SSA, infection prevention and control (IPC) programs do not exist in many hospitals, particularly at district/first-level hospitals, where the burden of SSI is highest.

Operating room (OR) supply limitations contributing to surgical site infections in low- and middle-income countries.
Additional Factors Contributing to Risk of Surgical Site Infections in Low- and Medium-Income Countries
Burden of Complicated Intra-Abdominal Infections (IAIs) in LMICs
Reports on complicated IAIs in LMICs are mostly on individual pathologies, and the quality of the reports often is low, making it difficult to appreciate the full picture and true burden of the infection in this setting. In some reports [34,35], IAI was the indication for laparotomy in 19% and 34% of patients, respectively, at district and referral-level hospitals in the Republic of Benin and Nigeria. It is now well known that typhoid intestinal perforation (TIP) is a common cause of severe IAI in SSA. In one report [36], the incidence of complicated typhoid fever, as well as the mortality rate, was highest in SSA. Even in surviving patients, the morbidity from the condition is high and distressing (Fig. 3).

Severe malnutrition from complicated intra-abdominal infection caused by typhoid intestinal perforation.
Several guidelines on the management of complicated IAIs have been developed for HICs, but their applicability in LMICs remains uncertain. For instance, antibiotics commonly recommended by these guidelines (e.g., carbapenems, piperacillin-tazobactam) either are not readily available or are too expensive and unaffordable for many patients, who must pay for their care out of pocket (OOP).
Disparities in Surgical Infections: HICs Versus LMICs
Much disparity exists between HICs and LMICs in the profile of surgical infections [37].The prevalence and incidence of SSI in LMICs is alarmingly high with very little effort being made to address it (see Tables 1 and 2). Despite the low rates in HICs, these countries continue to make efforts to control the problem through well-planned IPC programs [15,16,38], whereas the scope and quality of available data and information, including implementation of guidelines and care bundles, are limited in LMICs. Further, largely preventable risk factors such as malnutrition, limited access to surgery and antibiotics, delayed presentation with advanced disease, and other co-morbidities that are uncommon in HICS are prevalent in LMICs [10].
Similarly, the quality and scope of reports on IAIs from LMICs are limited, and context-specific guidelines do not exist. Despite the highest concentrations of complicated typhoid fever being in LMICs [36], with an overall case fatality rate as high as 15.4% [39], data are sparse, with no active surveillance data from these high-burden countries [36]. Although most patients with complicated IAIs in these settings are severely ill and require critical care, the infrastructure, equipment, and human resources needed to provide such care are limited, and this contributes to the high morbidity and mortality rate [10].
Some of these disparities have contributed to the neglect of surgical infections in LMICs over the years. Much needs to be done to control these infections and bring these countries onto the global surgery and health platform and agenda.
Economic Implications
The economic impact of SSI has been outlined in HICs [40,41], but the impact in LMICs is uncertain. This has hindered progress at a global level. To advocate successfully for a global focus on surgical infections from an economic perspective would require:
Knowledge and understanding of the impact of SSI on healthcare costs, especially in low-resource settings;
Modelling of the potential economic losses caused by surgical infections;
Modelling of the economic benefits and gains of investing in the prevention and control of surgical infections.
Healthcare spending by governments in LMICs is low, and OOP expenditure and development assistance account for as much as 60% of the entire outlay [42]. Given that these are the countries with the largest burden of surgical infections, families are at high risk of being driven into poverty by catastrophic health expenditure (CHE) for the treatment of a surgical infection. In one report on peritonitis [43] from Rwanda, with a population of 12 million, 14% of patients were at risk of CHE from OOP payments if only medical cost is considered, increasing to 28% if non-medical costs are included, despite 98% of the patients having health insurance. In Nigeria (unpublished data) with a population of 199 million, a gross domestic product per capita of US$2,028.18 [41] and about 5% health insurance coverage, 32 children undergoing laparotomy for peritonitis caused by TIP were reviewed; the medical cost was US$236–US$1,700 (median US$325), putting 100% of the families at risk of CHE from OOP payment. These initial findings on the cost of treatment of peritonitis in SSA provide a powerful tool for messaging for advocacy on a global focus on surgical infections, but more data are needed to put the economic impact of surgical infection in a more convincing perspective.
Scaling Up Access to Surgical Care
After the passage of WHA resolution 68:15 [9], several countries in SSA and other LMICs have produced NSOAPs or are planning to do so [44]. These plans are directed at scaling up access to surgical care, particularly at district/first-level healthcare facilities.
A key goal of the NSOAPs is to increase surgical volume to the recommended rate of 5,000 per 100,000 population by 2030. Four countries in SSA that have completed a NSOAP plan to increase surgical volumes by 204%–933% in the next few years (Table 5) [44]. The basic target of surgical scale up is to increase access to Bellwether procedures (caesarean section, laparotomy, open fracture repair) at district/first-level facilities. A recent review revealed a post-caesarean SSI rate in SSA of 4.4%–48.2% [45]. Given this high rate, there is the potential for blowout of SSI rates if no IPC programs are implemented along with the scaling up of surgical volume and access to care. This would have serious economic as well as outcome implications [40]. Another implication is that more laparotomies would be done for IAIs in these settings in the coming years. To prepare for this scale up, provision of infrastructure, equipment, human resources for health [10], and globally implementable IAI guidelines are needed urgently, including training modules and manuals on surgical techniques in the treatment of IAIs. Importantly, source control guidelines that can be taught and implemented at lower hospital levels are crucial. The Surgical Infection Society of North America (SIS-NA) and other infection-focused societies and stakeholders would need to come together to work on these guidelines.
Increase in Surgical Volumes Targeted By National Surgical, Obstetrics, and Anesthesia Plans [44]
Antibiotic Resistance
Antibiotic resistance is growing at an increasing rate and threatens advances in surgery worldwide [46]. The impact of these mutations on SSIs and surgical infections in LMICs could be massive [47]. In quantifying the burden of SSI, it is important to consider the larger impact of SSI caused by resistant bacteria [48]. One recent report on SSI after gastrointestinal surgery [1] showed an overall antibiotic resistance rate of 21.6% for bacteria cultured from incision swabs. The highest rate was 35.9% in low-HDI countries compared with 16.6% and 19.8% in high-HDI and middle-HDI countries, respectively. In a tertiary health facility in Nigeria (unpublished data), over a six-month period in 2018, the antibiotic resistance rate was high for bacteria cultured from surgical infections (Fig. 4); resistance to antibiotics not commonly used in the setting was high, at 17.2% and 20.5% for imipenem and meropenem, respectively, and 39.6% for piperacillin-tazobactam. Despite the high antibiotic resistance rates, most countries in the WHO Africa region have no national antimicrobial resistance plans; and information does not exist for many of the countries [49].
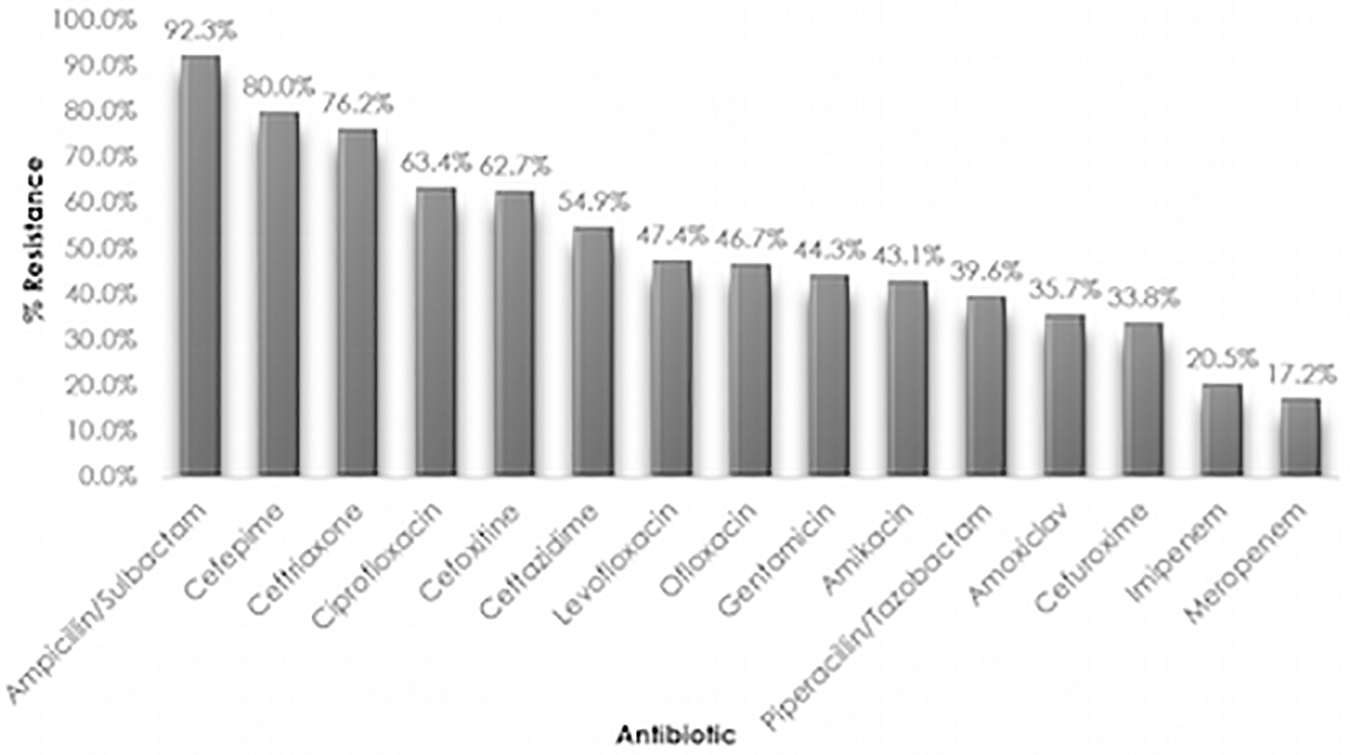
Antibiotic resistance of bacteria cultured from 234 surgical incisions over six months at a tertiary hospital in Nigeria, 2018.
Surgical Infection as Emerging Frontier in Global Health: Time for a Global Focus
Despite the increasing profile of surgery on the global health agenda [6], surgical infections have not received the desired international attention. There now are compelling reasons that surgical infections should not continue to be neglected.
In 2015, the World Bank, through the publication of the Disease Control Priorities Third Edition (DCP3) on essential surgery, made a case for investing in surgical care as well as expanding access to surgical care [8]. That report provided information on DALYs for surgical conditions to make the case for investment. However, there was little or no information on surgical infections. Further, in 2017, another volume of DCP3 focused on infectious diseases and made a case for investing in eradication of neglected tropical diseases, but these were mostly parasitic infestations; and again, surgical infection was left out [50].
There has been some global activity on SSIs in recent times with WHO's publication in 2016 on global guidelines for their prevention [16]. However, awareness and uptake of these guidelines in LMICs has been low, especially by surgeons. The WHO has followed up with the creation of an implementation roadmap, but efforts at implementation at country levels is limited. This document is at risk of being added to the bookshelf and forgotten if efforts are not made by the global surgeon community to raise the profile of surgical infections. A coalition is urgently needed to advocate for surgical infection control and elevate it to the global platform (Table 6).
Needed Action to Elevate Surgical Infections to Global Platform
To realize the health-related targets of sustainable development goals [51] and achieve universal health coverage [52], it is crucial that access to emergency and essential surgical care be scaled up. This is already being done, but corresponding attention needs to be given to surgical infections. These infections should no longer be ignored, and they are now the next frontier for action, advocacy, and investment in global health and surgery.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose