
Abstract
Background:
Surgical site infections (SSIs) are recognized complications of surgical procedures. Methicillin-resistant Staphylococcus aureus (MRSA) colonization increases the likelihood of developing SSIs. Decolonization of MRSA has been shown to reduce post-operative SSIs, therefore, the aim of this project was to identify and decolonize MRSA carriers and to tailor perioperative antibiotic prophylaxis to protect those at high risk for SSIs better.
Methods:
In September 2013, a quality improvement process initiative was implemented for pre-operative screening of MRSA nasal carriage for patients undergoing elective neurosurgical procedures. Those identified as colonized received a 10-day decolonization protocol that consisted of: oral doxycycline 100 mg twice daily or oral trimethoprim-sulfamethoxazole (TMP-SMX) DS twice daily; oral rifampin 600 mg daily; daily bathing with chlorhexidine; and twice daily use of mupirocin ointment in each nostril and under the fingernails. In addition to cefazolin (weight-based dosing), vancomycin (weight-based dosing) was recommended for perioperative prophylaxis in known MRSA carriers and patients undergoing surgical procedures involving hardware implantation irrespective of colonization status. We compared the results with our previously documented neurosurgical site infection rates (2012 and 2013 were 3.0 and 2.2%, respectively)
Results:
From 2014 to 2015, MRSA screening was done for 1,197 patients, of whom 52 (4.3%) were found to be colonized. Surgical site infections occurred in 14 procedures (1.4%) in 2014 and eight (0.8%) procedures in 2015, respectively. Methicillin-resistant Staphylococcus aureus remained responsible for most of these infections. None of the patients who underwent decolonization developed an infection (MRSA or otherwise).
Conclusions:
The overall rate of neurosurgical site infections can be reduced through a bundled approach of MRSA decolonization and change in perioperative antibiotic prophylaxis to include vancomycin for procedures involving hardware implantation irrespective of MRSA carriage state.
Surgical site infections (SSIs) remain a concern for institutions, physicians, and patients. The risk of SSIs depends on multiple factors including environmental factors, patients' underlying morbidities, state of health at the time of surgery, colonization with bacterial pathogens, and type of surgical procedure performed [1]. Meticulous attention to these modifiable and preventable variables can help healthcare institutions meet the quality measures recommended by various regulatory bodies and ensure quality care and good patient outcomes.
The rate of SSIs varies by the type of surgical procedure. Traditionally, surgical procedures are classified into clean, clean/contaminated, contaminated, and dirty. One study of a large pool of patients (634,426 cases) found that the rates of superficial SSIs were 1.76%, 3.94%, 4.75%, and 5.16%, respectively [2]. Neurosurgical site infection rates have been reported at varying frequency in the literature. In some estimates as high as 4.4% [3], and in others up to 11% [4]. These infections carry substantial morbidity, mortality, and financial burden to the healthcare system. The matter becomes more complex when such procedures involve the implantation of instruments such as stabilization devices (e.g., plates, rods, and screws) and electronic or mechanical devices such as stimulators and shunts.
To manage infections that occur after neurosurgical procedures, incision care and administration of systemic antibiotic agents are the standard of care. The management can be more complex and requires re-admission to the hospital for surgical debridement and intravenous antibiotic agents. In some cases, additional surgical procedures and hardware extraction is needed to resolve the infection. One study estimated the cost incurred as a result of cervical spine fusion infections to be more than $12,000 dollars per episode [5].
The average rate of neurosurgical site infections at our institution was 2.8%, which was within the range reported in the literature [4,6]. Surgical site infections at our institution were caused by a variety of micro-organisms, most SSIs were monomicrobial and in many cases methicillin-resistant Staphylococcus aureus (MRSA) was the culprit microorganism. There was inconsistency in MRSA screening and management of colonized patients between different neurosurgeons. The literature suggests that detection and eradication of MRSA can prevent SSIs and is cost-effective even with low colonization rates [7]. Therefore, we conducted a quality improvement project to decolonize patients with positive for MRSA. The primary goal of the project was to reduce the rate of SSIs in neurosurgical procedures through a bundle approach of MRSA decolonization and adjustment of perioperative antibiotic prophylaxis in higher risk patients. In this review we compare the rates of SSIs in neurosurgical patients before and after the implementation of the screening-decolonization quality improvement protocol.
Patients and Methods
This is a retrospective review to evaluate the quality improvement process conducted at our institution, a regional referral center with 303 staffed beds located in Huntington, West Virginia, between 2012 and 2015. We reviewed the internally reported SSIs by our infection control department for all neurosurgical procedures performed in years before and after the introduction of a bundle of interventions aimed at reducing SSI rates, which was introduced at the end of 2013. Data from 2012 through 2015 were obtained from infection control and from antimicrobial stewardship program.
Quality improvement protocol
Our infectious diseases group often used an aggressive decolonization protocol that consisted of topical chlorhexidine, topical mupirocin, and systemic doxycycline or trimethoprim-sulfamethoxazole (TMP-SMX) and rifampin. The program was based on both literature supportive of topical and systemic approach to a more successful eradiation of MRSA colonization [8,9] and the team clinical decision to extend the systemic therapy to 10 days. The choice of antibiotic agents depended on the individual patient's allergies, intolerance, and drug–drug interactions, among other parameters, with preference to doxycycline plus rifampin because doxycycline had better efficacy against MRSA based on our institution's antibiogram.
To streamline the process and ensure a consistent approach, an algorithm was created to screen all neurosurgical candidates at least two weeks prior to the anticipated procedure date, which would allow enough time to test for MRSA colonization and to implement the 10-day decolonization protocol. In addition, perioperative prophylaxis was changed to include vancomycin (in addition to cefazolin) in patients with MRSA colonization and in patients undergoing device implantation, which was shown in some studies to be of benefit [10].
Patients who were evaluated in the outpatient clinic for neurosurgical procedures underwent routine perioperative evaluation. In addition, patients underwent screening for MRSA colonization via nasal swab. The swab was streaked on a CHROMagar MRSA plate (DRG International Inc., Springfield, NJ). The results were read after 24 and 48 hours of incubation at 35°C. The growth of colonies showing any pink or mauve color was presumptive positive for MRSA. Isolates were reported once confirmed MRSA by susceptibility testing as recommended by the manufacturer (Remel, Lenexa, KS).
Patients who were found to be colonized with MRSA were prescribed a 10-day decolonization protocol that consisted of daily bathing with chlorhexidine, twice daily application of mupirocin ointment in the nostrils and under the fingernails, twice daily oral doxycycline 100 mg (or twice daily TMP-SMX 160 mg/800 mg) and rifampin 300 mg (unless contraindicated because of severe allergy history or potential drug–drug interaction). Patients also received chlorhexidine wipes to use on the night before surgery and the day of surgery as part of the routine pre-operative care. Perioperative antibiotic prophylaxis was given in accordance with Surgical Care Improvement Project (SCIP) guidelines [11,12]. However, if patients were known to be colonized with MRSA (even though they might have undergone decolonization) or if they were having a neurosurgical procedure involving implantation of hardware, a single dose of vancomycin 15 mg/kg was given in conjunction with cefazolin 1 g once (if weight <90 kg) and 2 g once (if body weight is ≥90 kg) [11]. Vancomycin alone was given in cases of confirmed severe penicillin or cephalosporin allergy. During the intervention period there were no other changes made to our institutional operative procedures and standards.
The rates of neurosurgical site infections were determined by infection control department. National Healthcare Safety Network definitions were followed in identifying SSIs before and throughout the intervention period. Baseline data from 2012 and 2013 marked the pre-intervention period and subsequent data from 2014 and 2015 marked the post-interventions period.
To determine the safety and tolerability of the decolonization protocol, a telephone survey was conducted in February 2016 attempting to contact all patients who tested positive for MRSA colonization. Those who could be contacted were asked a series of questions pertaining to their MRSA history, decolonization program compliance, and side effects (Table 1).
Questions Used in the Telephone Survey for Patients Who Tested Positive for MRSA from Nasal Swab Specimens
MRSA = methicillin-resistant Staphylococcus aureus.
Results
Since the introduction of the protocol until the end of the intervention phase (September 2013 to October 2015), 1,197 patients underwent screening for MRSA colonization. The number of patients who screened positive were 52 (4.3%). Prior to the introduction of the screening/decolonization/modified prophylaxis bundle the infection rate for neurosurgical procedures at our institution reached 2.8%. In the year after implementation of the protocol, the infection rate declined to 1.8% and to 0.8% the following year (Fig. 1). Infections caused by MRSA per number of procedures were five in 621 (0.8%) in 2012 and four in 773 (0.5%) in 2013 compared with five in 1,022 (0.48%) in 2014 and one in 1,043 (0.09%) in 2015. Out of the total number of infections per year MRSA infections represented five in 14 (36%) in 2012 and four in 22 (18%) in 2013 compared to five in 14 (36%) in 2014 and one in eight (13%) in 2015.
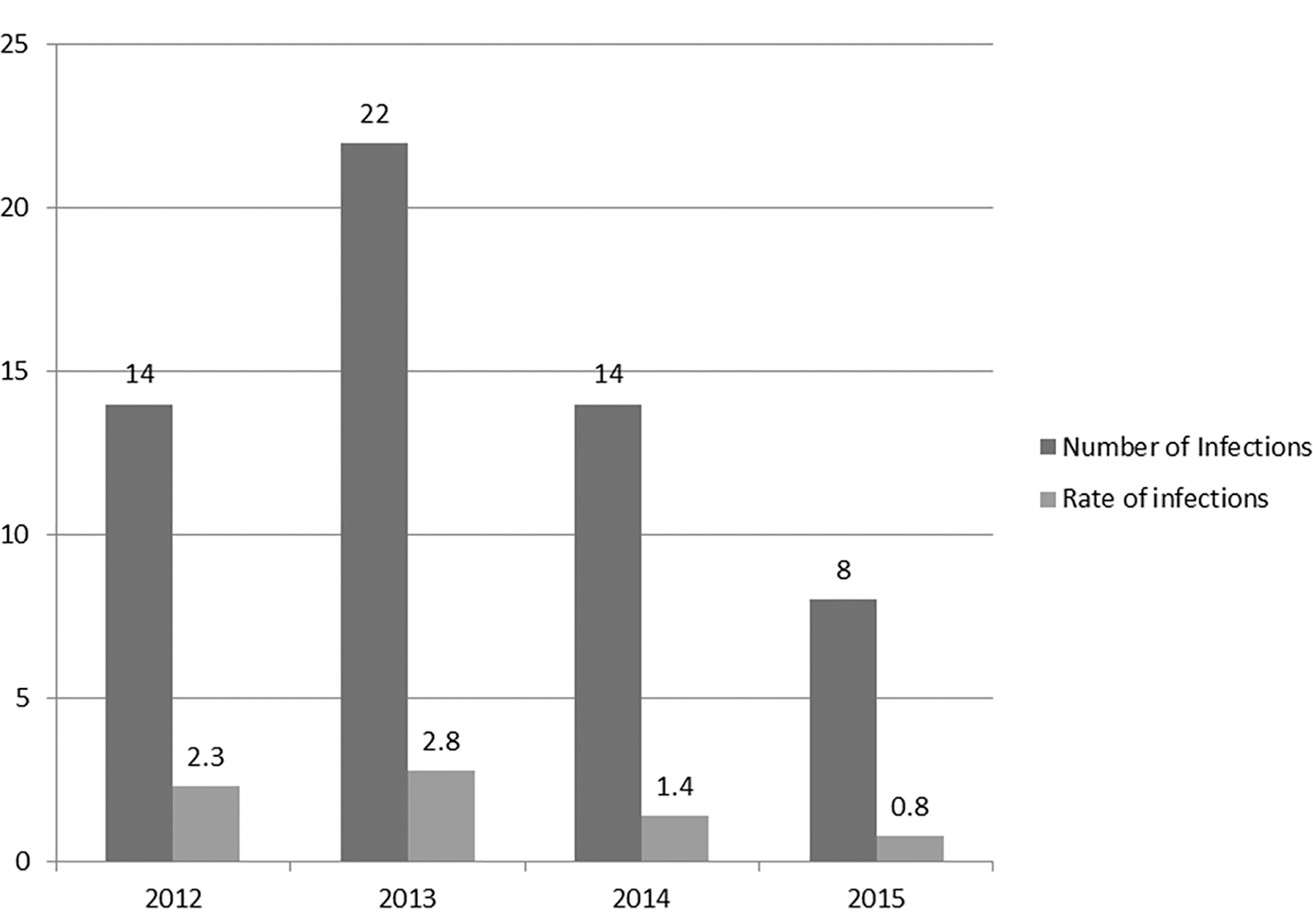
Number of infections and rates for neurosurgical procedures, 2012–2015. Number of procedures were 621, 773, 1,022, and 1,043 for the years 2012, 2013, 2014, and 2015, respectively (not shown in the graph).
The prescription pattern for perioperative prophylaxis changed after implementation of the protocol and, as expected, the use of vancomycin increased but as a combination agent with cefazolin. The use of vancomycin alone did not change, and the use of cefazolin alone declined as more vancomycin was being used concomitantly (Fig. 2).

Percentage of usage of perioperative antibiotic agents for neurosurgical procedures, 2012–2015.
We attempted to contact all the 52 patients who tested positive for MRSA. We were only able to reach 32, however, six of them did not participate in the survey (two declined and four had no recollection of the pre-operative period). Two of them had history of MRSA and nausea was reported by five. None of the patients developed Clostridium difficile infection.
Discussion
The number of surgical procedures performed in U.S. hospitals has increased because of population expansion, increased longevity, and advancement in medical technologies. In 2010 alone, 16 million procedures were performed based on data from the National Hospital Discharge Survey [12]. At our institution, we follow SSI trends for internal monitoring as participants in insurance-sponsored nationwide quality improvement initiatives. However, there are no national mandatory reporting requirements or registries for infectious complications of neurosurgical procedures. The National Healthcare Safety Network only requires reporting infectious complications of hysterectomies and colon procedures [6]. Because of that, we have no benchmarks for what would be considered acceptable rate of neurosurgical SSIs.
Surgical site infections are responsible for substantial morbidity and mortality. They are responsible for almost one-third of health-care–associated infections (HAIs) in acute care hospitals, and hence, the most prevalent HAI [13]. Surgical site infections prolong hospital stay and add substantially to healthcare costs [14]. For these reasons, reducing SSIs through a bundle approach is paramount. It is important to select patients who need surgical interventions carefully and allow enough time for risk modification prior to surgery. Such risks that can be modified include smoking, obesity, hyperglycemia, and colonization with resistant pathogens [7].
Most institutions have standardized procedures to monitor and control selected risk factors. However, screening for MRSA colonization, adopting a decolonization program, and choice of antimicrobial perioperative prophylaxis are far less standardized in neurosurgical procedures.
Neurosurgical site infections can have an early or delayed onset, can be monomicrobial or polymicrobial, and often involving MRSA where MRSA is more prevalent. In one survey from North America, MRSA was the culprit in one-third of infected spinal fusion procedures [15]. Healthcare institutions follow SCIP antibiotic prophylaxis recommendations to meet regulatory requirements. However, the approach to the prevention of SSIs should incorporate local microbiologic and epidemiologic data. Choice of antibiotic prophylaxis should consider resistant organism colonization rates, types of organisms causing SSIs, and antimicrobial resistance patterns.
Guidelines for perioperative antimicrobial prophylaxis are based on data from an era when resistance was substantially less prevalent. The guidelines that were initially issued to address SSIs were published in 1994, and those were not updated until 2013 [11,16]. As a result of wide adoption of the earlier guidelines, SSIs caused by gram-negative bacteria were reduced substantially, however, Staphylococcus aureus remains a major player with MRSA constituting a substantial proportion of those SSIs [17].
Data analysis of patients re-admitted to U.S. hospitals from 2003 to 2007 because of SSIs found that culture-confirmed SSIs caused by MRSA increased substantially from 16.1% to 20.6% [18]. Additionally, mortality rate, hospital stay, and healthcare cost were more when MRSA was the culprit in comparison with other pathogens. Furthermore, Staphylococcus aureus colonization patterns have changed. According to a national survey for nasal colonization with Staphylococcus aureus in the general population between 2001 through 2004, there was a decline in Staphylococcus aureus colonization from 32% to 29% and a substantial increase in MRSA colonization (from 0.8% to 1.5%) [19].
Our comprehensive approach resulted in substantial reduction in SSIs in neurosurgical patients. Prior to the introduction of the screening/decolonization protocol and the change in antibiotic prophylaxis, the infection rate for neurosurgical procedures at our institution was as high as 2.8%. In the year after implementation of the protocol, the infection rate declined to 1.8% and to 0.8% the following year. Our current rates of 0.8% are well below most reported rates. More vancomycin was used in our patient population after implementation of the protocol. This is certainly a concern because of given potential side effects, requirements for dosing and monitoring, and increased cost. Further studies are needed to determine the best MRSA perioperative prophylaxis in surgical populations at increased risk for devastating MRSA infections. An ideal perioperative prophylactic agent should be easy to administer, achieves good tissue concentration at the surgical site for the duration of the procedure without the need to re-dose, requires no monitoring, has a reasonable side effect profile, and is reasonably priced. Hence, vancomycin may not be the ideal agent for practices that do not have the required pharmacokinetic support or practices that serve patient populations at increased risk for vancomycin toxicity.
Similar to most bundle approaches, it is not easy to determine which component(s) of our bundle impacted the outcome the most nor can we extrapolate that a similar impact would be seen at other institutions or other surgical specialties. In addition, given the non-interventional nature of the study, 9% of patients in 2012 and 20% of patients in 2013 received a combination of vancomycin and cefazolin that was based on the neurosurgery team decision on a case by case basis (perception of higher MRSA incidence of colonization), not necessarily guided by history of MRSA infection or colonization.
Another limitation of our study was that we were only able to screen 58% of patients because the screening and decolonization process was only possible for electively scheduled procedures through the outpatient clinic. Transfers from other facilities, urgent and emergent cases, and emergency department admissions were not screened. Hence, further large-scale multicenter studies need to be conducted for such determinations to be made. Despite these limitations, our data show that screening for MRSA colonization and aggressive decolonization protocol in conjunction with perioperative prophylaxis for MRSA in higher risk groups (patients with history of MRSA colonization or infection and patients undergoing procedures involving hardware implantation) reduced all-cause SSIs including MRSA. Additionally, our survey showed that our comprehensive protocol was well tolerated and did not cause major adverse events such as Clostridium difficile infection.
Footnotes
Authors' Contributions
All authors have contributed substantially to all parts of this article and all authors agree with the content of the article.
Author Disclosure Statement
There is no conflict of interest of any type for any of the authors. The content of this paper has not been published or submitted for publication elsewhere.