
Abstract
Object:
To analyze the factors influencing surgical site infection (SSI) after pancreaticoduodenectomy and to establish a scoring system for predicting such infections.
Methods:
Patients who underwent pancreaticoduodenectomy in the Department of Hepatobiliary Surgery of the Second Affiliated Hospital of Chongqing Medical University from January 2015 to March 2019 were divided randomly into a model group and a test group in a proportion of 3:1. According to whether an SSI occurred after operation, the model group was divided into an incision-infection group and a non-infection group. Univariable analysis and multivariable regression analysis were used to analyze factors related to post-operative incision infection and to establish a clinical predictive scoring system. The scoring system was evaluated for the test group.
Results:
A total of 236 patients, 177 in the model group and 59 in the test group, were included. In the model group, univariable and logistic regression analysis showed that tumor nature (benign versus malignant), post-operative albumin concentration, pancreatic fistula formation, post-operative cough, and peri-operative blood transfusion were the independent risk factors for incision infection. Then we established a clinical predictive scoring system. In the test group, the area under the receiver operator characteristic curve of the system was 0.768 (p < 0.001, with sensitivity = 59.1% and specificity = 94.6%).
Conclusion:
The scoring system had good clinical prediction ability and high specificity, so it was worth using in the clinic.
Pancreaticoduodenectomy (PD) is one of the most difficult operations in hepatobiliary surgery. It is the main treatment for pancreatic head cancer, peri-ampullary carcinoma, duodenal tumor, and lower bile duct tumors. Because of the complicated operative steps, there are many post-operative complications, including surgical site infection (SSI), gastrointestinal bleeding, bile leakage, pancreatic fistula formation, abdominal infection, delayed gastric emptying, and pulmonary infection [1]. With improvement of surgical techniques and standardized management in the peri-operative period, the mortality rate has been reduced significantly [2]. However, the incidence of post-operative complications is still high, and one of the most common is SSI [3,4].
Surgical site infection is one of the main factors that prolongs the hospital stay and increases the economic burden. Therefore, measures should be taken to protect patients having a high risk for SSI and avoid serious consequences. The purpose of this study was to explore risk factors for SSI and establish a scoring system to predict such infections.
Patients and Methods
Patients
By searching the database of our hospital, all patients who underwent pancreaticoduodenectomy from January 2015 to March 2019 were selected. Then we collected and sorted the medical records and laboratory and imaging results of these patients. The whole process of this study conformed to the STROCSS criteria [5], and the ethics committee of our hospital had reviewed and unanimously approved the study.
The inclusion criteria were: (1) PD in our department from January 2015 to March 2019; (2) no absolute surgical contraindications such as important organ dysfunction; (3) complete clinical data available. Patients with severe heart, brain, lung, or other organ dysfunction and with serious post-operative complications such as abdominal hemorrhage, death, or other results that might significantly affect the outcome of the study were excluded. In addition, those cases of laparoscopic pancreaticoduodenectomy and laparoscopic conversion to laparotomy were excluded.
Surgical technique
Surgeons with extensive experience in pancreatic surgery used the normative Whipple procedure to remove the pancreatic tissue according to the nature and depth of the lesion. They cut the common hepatic duct 0.5–1.0 cm above the junction of the cystic duct and the common bile duct; removed the gallbladder, the lower part of the common bile duct, the distal stomach (30%–60%), and all of the duodenum and jejunum 10–15 cm below Treitz's ligament; and cleared the lymph nodes if the disease was malignant. The specific scope of lymph node removal was determined according to the type of disease. Traditional methods of digestive tract reconstruction were carried out in all patients. According to the diameter of the pancreatic duct and the texture of the residual pancreas, surgeons chose a particular method of pancreaticojejunostomy and performed internal or external pancreatic duct drainage. Placement of a T-tube was determined by the individual experience of the surgeon. Peripancreatic drainage tubes were placed in all patients.
All patients received a prophylactic antibiotic (cefazolin 2 g intravenously) 30 min before the skin incision. After operation, all patients were fasted and had indwelling gastric tubes until intestinal function recovered. The incision was dressed every other day, and this was changed to daily dressing if the site was infected. All patients were given acid-inhibiting drugs, protection of the stomach, inhibition of pancreatic juice secretion, and supplemental nutrition.
The patients were followed up for at least 30 days. An SSI was diagnosed according to the definitions in the guidelines issued by the National Nosocomial Infections Surveillance system [6]. The diagnostic criterion for SSI was infection that occurred within 30 days after the operation involving the skin, subcutaneous tissue, or deep soft tissue (e.g., fascia and muscle layers) at the incision site and at least one of the following: (1) Drainage or puncture of pus (except drainage after infectious surgery); (2) purulent secretions from the incision or accompanied by fever, swelling, local pain, and tenderness; (3) relevant evidence of infection found by re-operation, imaging, or histopathology examination; 4) infection of the skin, subcutaneous tissue, or deep soft tissue diagnosed by clinicians.
All patients were divided randomly into a model group and a test group in a proportion of 3:1. The model group was divided into an incision-infection group and non-infection group according to the occurrence of SSI.
Outcomes
On the basis of clinical experience and related literature, the data were used to analyze the factors potentially related to SSI, which were as follows: (1) Pre-operative clinical data (gender, age, body mass index [BMI], smoking history, diabetes, tumor nature, season of the operation); (2) clinical data during the operation: Operative time, ascites, operative blood loss, peri-operative blood transfusion; and (3) post-operative clinical data: Albumin concentration the first day after the operation, pancreatic fistula formation, bile leakage, post-operative cough, and incision infection.
The diagnostic criteria were bile leakage: Bile-like fluid draining from the abdominal tube with a bilirubin concentration more than three times that of serum bilirubin monitored at the same time, which was confirmed by B-ultrasound or CT examination [7]. Pancreatic fistula was diagnosed according to the definition of the 2016 International Pancreatic Fistula Research Group [8] in which the amylase content of any drainage fluid on the third day after the operation was more than three times the upper limit of normal. Grade A pancreatic fistula, also known as biochemical pancreatic fistula, has no effect on the patient's treatment and hospital stay, whereas grades B and C fistulas are considered to be clinically significant and were used as the observation indicator of this study. Post-operative cough was diagnosed by checking the nursing records to detect paroxysmal coughing for any reason within one week after the operation, lasting more than three days, averaging more than two hours per day (except in those who had a cough and pulmonary infectious diseases before the operation).
Statistical analysis
Data analysis was performed using the SPSS (IBM version 23) program. The measurement data of normal or approximately normal distribution were expressed as the mean±standard deviation, and the comparison between groups was performed by the t-test. The measurement of skewness was expressed by median (range of values) and compared with the Mann-Whitney U test. The counting data were expressed by rate or constituent ratio, and the χ2 test was used for the comparison of the two groups. Variables selected by univariable analyses (p < 0.05) were entered in a multivariable regression analysis model to estimate the association. Receiver operating characteristic (ROC) analysis was used to evaluate the established clinical predictive scoring system. Bilateral p < 0.05 was considered a statistically significant value.
Results
Univariable analysis
A total of 236 patients were divided randomly into two groups in a ratio of 3:1, 177 patients in the model group and 59 in the test group. The model group then was divided into an incision-infection group (n = 87) and non-incision infection group (n = 90). The overall incidence of incision infection was 49.2% (87/177), of which local swelling or fever accounted for 20.3% (n = 36), pain or tenderness 12.4% (n = 22), spontaneously dehiscence 4.5% (n = 8), suppurative exudation 10.7% (n = 19), and formation of local abscess 1.1% (n = 2). There was no statistical difference in age, Body Mass Index, smoking history, diabetes, operation season, operating time, intra-operative blood loss, or post-operative bile leakage between the incision and non-infection groups. However, there were significant differences in gender, tumor nature, post-operative albumin concentration, ascites, pancreatic fistula, post-operative cough, and peri-operative blood transfusion (Table 1).
Results of Univariable Analysis of Peri-Operative Factors Associated with Surgical Site Infection (SSI)
Multivariable analysis
Gender, tumor nature, post-operative albumin concentration, ascites, pancreatic fistula, post-operative cough, and peri-operative blood transfusion were analyzed by multivariable regression. Combined with clinical experience and the univariable analysis results, post-operative albumin concentration, malignant tumor, post-operative pancreatic fistula, post-operative cough, and peri-operative blood transfusion were statistically significant (Table 2).
Multivariable Regression Analysis of Predictors of Surgical Site Infection
Values in boldface type are significant, with a p value <0.05.
Establishment of clinical predictive scoring system
According to the results of multivariable regression analysis, the regression coefficients of each factor were rounded to establish a clinical predictive scoring system for SSI. The full score of the system was 8 (Table 3).
Clinical Predictive Scoring System for Surgical Site Infection
The full score is 8, and the score of 0–4 indicates a low risk of surgical site infection, whereas a score of 5–8 indicates a high risk.
Analysis of the scoring system and the data of the model group showed that the area under the ROC curve was 0.946 (p < 0.001), and the result was statistically different. At the same time, the critical value was 4.5, that is, when the cut-off point was 4.5, the sensitivity and specificity of the scoring system were the best (sensitivity = 86.2%; specificity = 97.8%). Therefore, we set the range of the scoring system to 0–8 points. When the score was <5 points, the risk of SSI was low, whereas when the score was ≥5 points, the risk of SSI was high (Fig. 1).
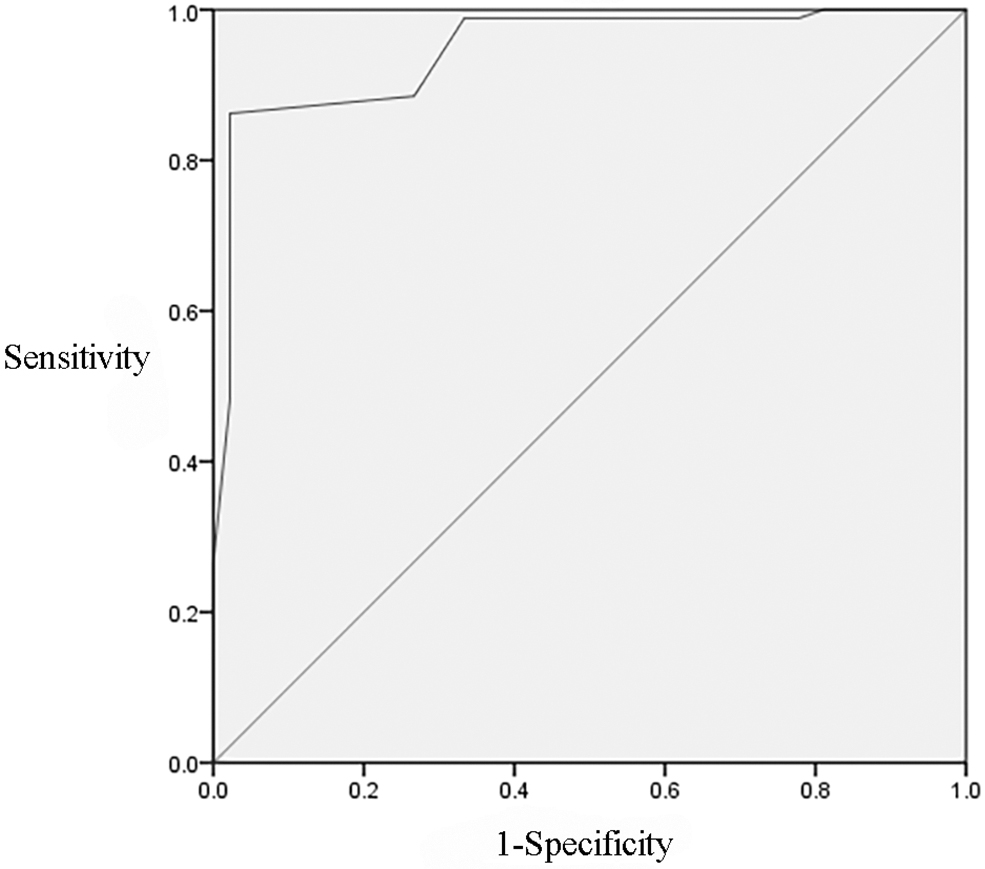
Receiver operating characteristic analysis for tumor nature, post-operative albumin concentration, pancreatic fistula, post-operative cough, and peri-operative blood transfusion of model group. The area under the curve was 0.946 (p < 0.001), with a sensitivity of 86.2% and a specificity of 97.8%.
The data of the test group was then used to examine the system. The area under the ROC curve was 0.768 (p = 0.001), which was statistically significant (sensitivity = 59.1%; specificity = 94.6%) (Fig. 2).
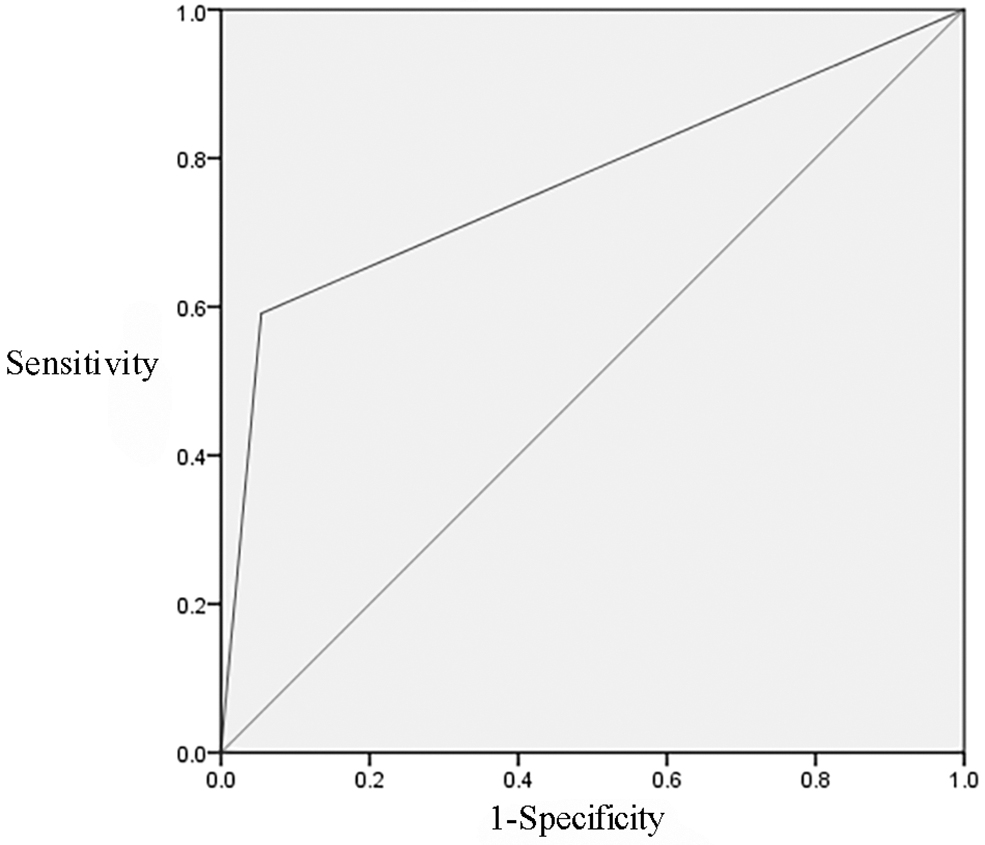
Receiver operating characteristic analysis for tumor nature, post-operative albumin concentration, pancreatic fistula, post-operative cough, and peri-operative blood transfusion of test group. Area under the curve was 0.768 (p = 0.001), with a sensitivity of 59.1% and a specificity of 94.6%.
Discussion
Pancreaticoduodenectomy is a complex operation with a high incidence of complications [9]. Although the morbidity and mortality rates have been decreased through the improvement of surgical techniques and intensive care management in recent years, the incidence of post-operative complications still is high [10,11]. Among these problems, SSI as one of the most common, sometimes significantly increasing the cost of hospitalization, prolonging the stay [12], and leading to an increase in infection-related deaths. Therefore, it is of great significance to evaluate the peri-operative risk factors for the prevention and treatment of post-operative SSI. However, so far, few studies have identified the factors associated with the development of SSI after PD. Consequently, this study collected and collated the clinical data of all patients who underwent PD in our hospital in recent years to explore the risk factors for SSI.
The incidence of SSI in the model group of this study was 49.2%. We considered the reasons as the following. First, this study was retrospective; we could obtain data only through the recorded clinical information. In order to avoid data loss, some patients with slight swelling or fat liquefaction who did not need special treatment were included. Second, there were 236 patients in total, 104 of whom suffered SSI (87 in the model group and 17 in the test group). The total incidence of SSI was 44.1%, but the incidence was higher in the model group. This may be related to sampling error caused by random assignment. If we continue to expand the sample, we may decrease this error and reduce the incidence of infection in the model group.
Univariable analysis showed that there were significant differences in gender, tumor nature, post-operative albumin concentration, ascites, post-operative pancreatic fistula occurrence, post-operative cough, and peri-operative blood transfusion between the case and the control groups. Women had a higher incidence of SSI, which suggests that estrogen has an effect on incision healing, but the specific mechanism needs to be confirmed by further study. Malignant tumor may affect the immune microenvironment and interfere with normal immune function, which leads to an increase in the risk of SSI. In addition, the post-operative albumin concentration in the case group was significantly lower than that in the control group, suggesting that this leads to a decrease in tissue repair ability and immune function, thus affecting incision healing, consistent with the results reported by Relles et al. [13] that hypoproteinemia is an independent predictor of complications after PD. Because we considered that surgery may lead to the loss of albumin, which would affect the results of the study, it was more appropriate to choose the albumin concentration on the first day after surgery as the study object.
The incidence of ascites was higher in the case group. We considered that it was related to hypoproteinemia, and ascites may be complicated by infection, which increased the risk of SSI. Pancreatic fistula formation is one of the common complications after PD; even with the improvement of anastomosis technique and the individualized choice of pancreaticoenterostomy, the incidence of pancreatic fistula is as high as 14.3%–49.9% [14,15]. In the case group, the incidence of pancreatic fistula was higher, which may be related to the accumulation and activation of trypsin in response to pancreatic fistula, with poor site healing caused by digestion of the tissue surrounding the surgical incision. The study also showed that peri-operative blood transfusion and post-operative cough were related to SSI. We speculated that the anastomosis and surgical incision were more prone to ischemia after massive hemorrhage, and post-operative cough caused increased intra-peritoneal pressure and repeated relaxation of the incision, resulting in poor incision healing and a higher risk of infection.
Multivariable regression analysis showed that malignant tumor, post-operative albumin concentration <30 g/L, pancreatic fistula, post-operative cough, and peri-operative blood transfusion were independent risk factors for SSI. Based on the results of multivariable regression, the clinical predictive scoring system of SSI was established, which was named CAPCT(Cancer, Albumin, Pancreatic fistula, Cough, Transfusion). The full score of the system was 8, including 2 each of tumor nature, post-operative albumin, and pancreatic fistula and 1 for post-operative cough and peri-operative blood transfusion. We used the data of the model group to analyze the scoring system, and the area under the ROC curve was 0.946 (p < 0.001), which was statistically significant, suggesting that the model was ideal. At the same time, the critical value was 4.5, when the scoring system was the best (sensitivity = 86.2%; specificity = 97.8%). Therefore, we stipulated that when the score was <5 points, the risk of SSI was low; otherwise, the risk of SSI was high.
In order to verify the scoring system, the test group was examined, and the area under the ROC curve was 0.768 (p = 0.001; sensitivity = 59.1%; specificity = 94.6%), which indicated that the model was ideal and the predictive effect was good. Meanwhile, we found the scoring system had high specificity, meaning that the model can better predict negative results.
This study had certain limitations. First of all, it was a retrospective analysis, and the objects of the study came from a single research center. Therefore, the quality of the study was not as good as that of a prospective multi-center study, and the results might be controversial. Second, in clinical work, our performance of the surgery for such patients is still cautious, so the sample was small, which may affect the accuracy of the results. Although we were able to validate this scoring system in a separate cohort of patients, the study was conducted using retrospective data, which may limit its application in the wider population. In order to avoid underestimating the real incidence of SSI after PD, additional validation with prospective data is needed.
Conclusion
The present study showed malignant tumor, post-operative albumin concentration <30 g/L, pancreatic fistula, post-operative cough, and peri-operative blood transfusion to be independent risk factors for SSI after PD. The clinical scoring system had good predictive power and high specificity, so it is worthy of clinical promotion.
Footnotes
Author Disclosure Statement
This study was not funded, and none of the authors has any conflicts of interests to disclose.