
Abstract
Background:
Skin preparation with an antiseptic solution aims to reduce surgical site infection rates. Surgical site infections (SSIs) create a high burden on healthcare systems with impacts on morbidity, mortality, and cost. In 2016, The World Health Organization (WHO) conducted an extensive systematic review and meta-analysis of the existing evidence. From this, they recommended the use of “alcohol based antiseptic solutions based on CHG for surgical site skin preparation in patients undergoing surgical procedures.” This study aimed to assess surgeon compliance with this guidance in the United Kingdom and India.
Methods:
A multiple-choice questionnaire was developed to assess surgeon preferences for antiseptic use in their surgical site preparation. The end point of data collection was defined after 50 responses in each region.
Results:
The majority of respondents in each center was general surgeons (n = 24, 48% United Kingdom; n = 21, 45% India), and registrars (n = 22, 44% United Kingdom; n = 23, 49% India). No surgeon preferred the use of any aqueous preparation. Chlorhexidine gluconate (CHG) was the preparation used most commonly in both centers (n = 30, 64% India; n = 24, 48% United Kingdom). In India, this represented a statistically significant difference (p = 0.0008), however, this was not observed in the United Kingdom (p = 0.22). There were no statistically significant differences between surgeon's reasons between the United Kingdom and India, other than “easier to see” (p = 0.016).
Conclusions:
This data show a reduced compliance of U.K. surgeons with WHO guidance for antiseptic use compared with Indian surgeons. Although the WHO has attempted to summarize the existing data to minimize the previous uncertainty surrounding antiseptic choices, the use of CHG continues to not be adopted widely. To draw robust conclusions to provide the foundations of further guidelines, future research should focus on prospective randomized controlled trials with large numbers across multiple surgical specialties.
Skin preparation with antiseptic solutions is a routine part of surgical site preparation in any surgery. The aim is to decrease surgical site infection rates by reducing micro-organisms present on the skin prior to incision. Surgical site infection (SSI) incidence is varied and dependent on the region and type of surgery performed (clean, clean-contaminated, contaminated, dirty). Reported SSI incidence in clean surgery is generally less than 2% whereas with contaminated or dirty surgery, rates can be more than 10% [1].
Because of the high number of surgeries performed globally, the number of SSIs, even in clean surgeries, is high. This creates a burden on healthcare systems around the world with impacts on morbidity, mortality, and cost. The World Health Organization (WHO) estimates 15% of all hospitalized patients suffer from health-care–associated infection (HCAI) [2], of which 8% can be attributable to SSI. In addition, one-third of post-operative deaths can be related to SSI [3–5]. There has been a reported increased hospital stay of approximately 10 days following an SSI [6] with an estimated annual economic impact of between $3.5 billion and $10 billion in the United States [7].
The most widely available and used antiseptic solutions are chlorhexidine gluconate (CHG) and povidone iodine (PVP-I) in alcohol or aqueous solutions. Before 2016, there was no clear guidance regarding the preferred antiseptic solution for surgical site preparation [8,9]. Although multiple guidelines did exist recommending alcohol-based solutions, these were not based on robust analysis such as systematic reviews or meta-analysis and were not clear in distinguishing between CHG and PVP-I [7,10,11].
The WHO conducted an extensive systematic review and meta-analysis of the existing evidence in 2016. This analysis used 17 randomized controlled trials (RCTs) comparing CHG and PVP-I in aqueous and alcohol solutions in an adult population. Sub-analysis of relevant trials drew the following conclusions with respect to reducing the SSI risk [12]: alcohol-based solutions are more effective than aqueous solutions; CHG (alcohol) was more effective than PVP-I (aqueous); and CHG (alcohol) was more effective than PVP-I (alcohol). The WHO global guidance therefore recommends the use of “alcohol based antiseptic solutions based on CHG for surgical site skin preparation in patients undergoing surgical procedures” [12].
Given the burdensome nature of SSIs, it seems prudent for surgeons to take every measure to reduce the risk of SSI. The WHO guidance is clear, simple, and does not discriminate between types of surgery and geographical location. This study therefore aimed to assess surgeon compliance with this guidance in the United Kingdom and determine how this compared with other countries.
Methods
A multiple-choice questionnaire was developed to assess surgeon preferences for antiseptic use in their surgical site preparation. We reached out to single centers in various countries (Australia, India, Malaysia, New Zealand, and South Africa) to gain a global picture of preferences, however, we only received responses for analysis from India. Both electronic and hard copies were developed to maximize engagement through different modalities. These were used once and one reminder was sent. Data on surgeon's reasons for their choice of antiseptic were also collected. The survey was designed in a multiple-choice format to receive responses on specialty, grade, antiseptic preferences, and reasoning. Individual surgeons were approached with hard copies of the survey and electronic versions were sent to departmental leads on a one-off basis for circulation to their teams. The end point of data collection was defined after 50 responses were received.
The surgical services offered at the U.K. center were general surgery (colorectal, upper gastrointestinal, and vascular), breast, trauma and orthopedic, urology, head and neck, cardiothoracic, and obstetrics and gynecology. Exclusion criteria were specialties in which chlorohexidine is commonly contraindicated (for example, in obstetrics and gynecology and ophthalmology, in which there is high exposure to mucosal membranes), pediatric surgery, and incomplete or erroneously filled surveys. The center in India (Kochi) offered additional neurosurgery and plastic surgery services, however, these were retrospectively excluded in order to best match the data to draw more valid comparisons.
Collected data were categorical and analyzed using MS Excel® version 16.31 (Microsoft, Redmond, WA). Chi-squared tests were used for comparisons. Graphs were produced using MS Excel version 16.31. The level of statistical significance was defined as p < 0.05.
Results
The survey received 50 responses from the United Kingdom and India. After exclusion, there were 50 analyzed responses from the United Kingdom and 47 from India (one gynecology, one ophthalmology, and one pediatric surgeon response excluded). The majority of respondents from both centers were from general surgery (n = 25, 50% United Kingdom and n = 22 47% India). A summary of the range of responses across specialties is shown in Figure 1. Because of the lack of consistency between the training pathways in the United Kingdom and India, we categorized data from “years post-qualification” and translated this into the U.K. system of foundation doctor, core trainee, registrar, and consultant. Foundation doctors represent doctors in the first two years post-graduation and core trainees are post-foundation doctors who have started their surgical training. Registrars are surgeons in training in a specific field (typically 5–12 years post-graduation) and consultants are the most senior doctors who have completed surgical training. Registrars comprise the majority of respondents from the United Kingdom (n = 22; 44%) compared with consultants in India (n = 23; 49%). The spread across grades is shown in Figure 2.
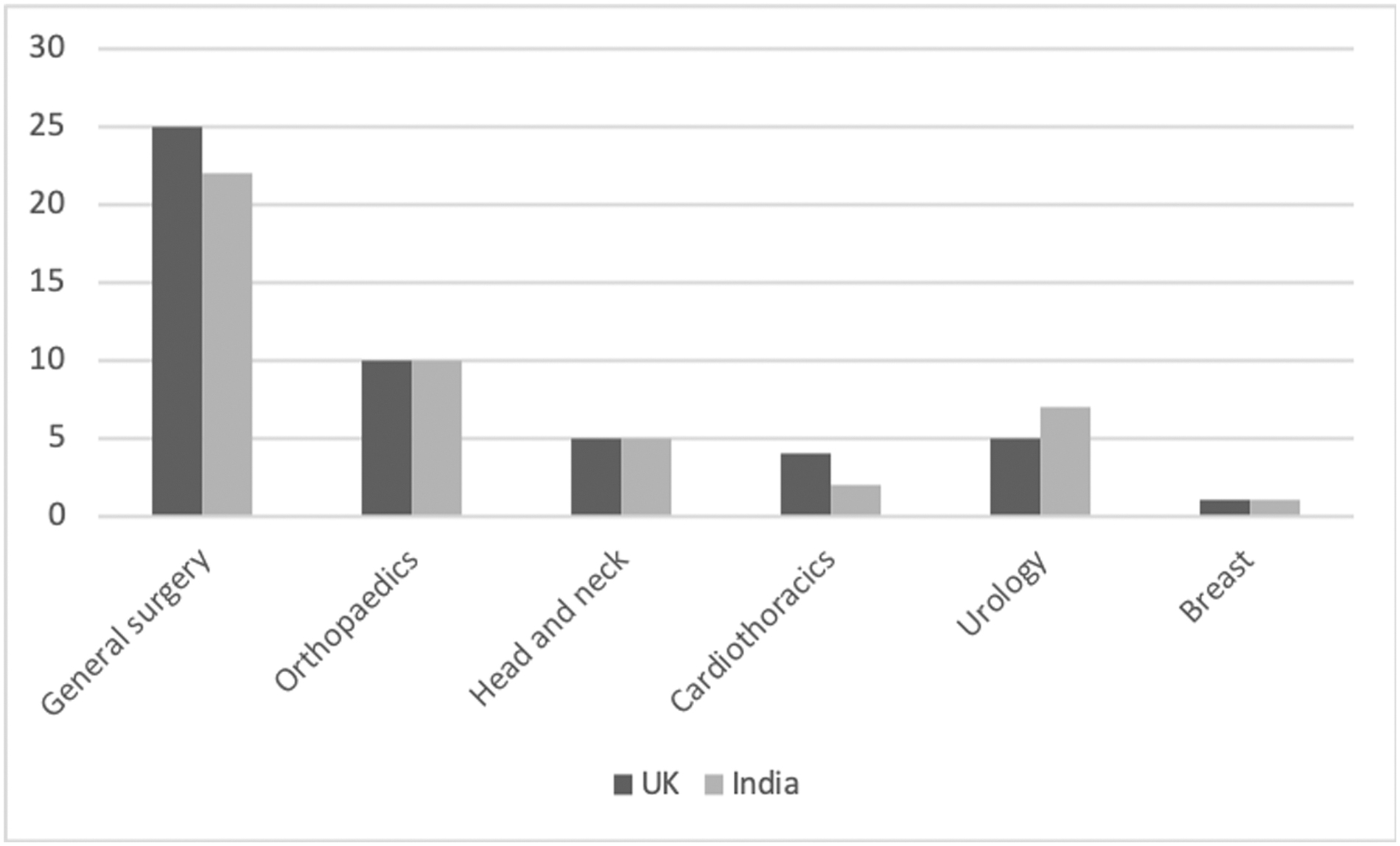
Range of responses across surgical specialties in the United Kingdom and India. There was no substantial difference observed between centers (p = 0.954).

Range of responses in terms of grades after adjustment of the grading system in India to the U.K. grading system of doctors. There was no substantial difference observed between centers (p = 0.330).
Figure 3 shows the surgical site preparations used in both centers. No surveyed surgeons in either center preferred the use of any aqueous preparation. The majority of surgeons in both centers used single preparation (n = 43, 86% United Kingdom; n = 38, 81% India) compared with dual preparation. Compared with other preparations, CHG was used most commonly in both centers (n = 30, 64% India; n = 24, 48% United Kingdom). In India, this represented a statistically significant difference (p = 0.0008), however, in the United Kingdom this was not observed (p = 0.22). For dual preparations, PVP-I followed by CHG was the most common dual preparation in both centers (n = 5, 10% United Kingdom; n = 9, 19% India).
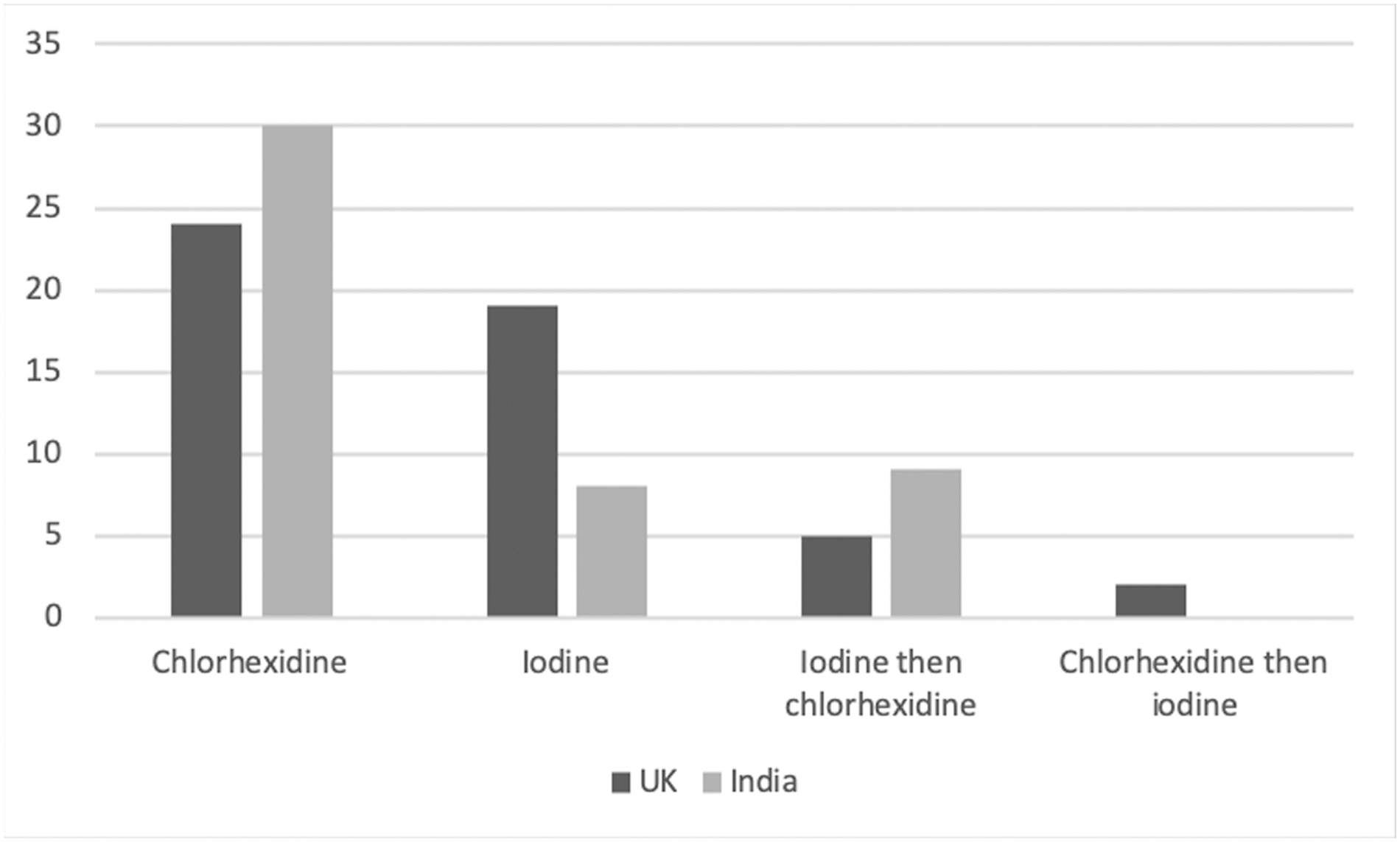
Surgical site preparation preferences in the United Kingdom and India. All preparations are alcohol because no surgeon preferred the use of any aqueous preparation.
Surgeons in the United Kingdom cited “awareness of evidence” (n = 20; 40%) and preparations being “easier to see” (n = 17; 34%) as their main reasons for choosing a particular preparation. Although surgeons in India agreed with “awareness of evidence” (n = 21; 45%) in their reasoning, they described preparations being “readily available” (n = 22; 47%) as their main reason. This was in contrast with the United Kingdom in which only 28% (n = 14) of surgeons said they chose their preparation based on its availability (Fig. 4). Despite this, were no statistically significant differences between surgeon's reasons between the United Kingdom and India for all surveyed responses (awareness of evidence, longer lasting, faster acting, readily available, advised by senior) other than “easier to see” (p = 0.016).
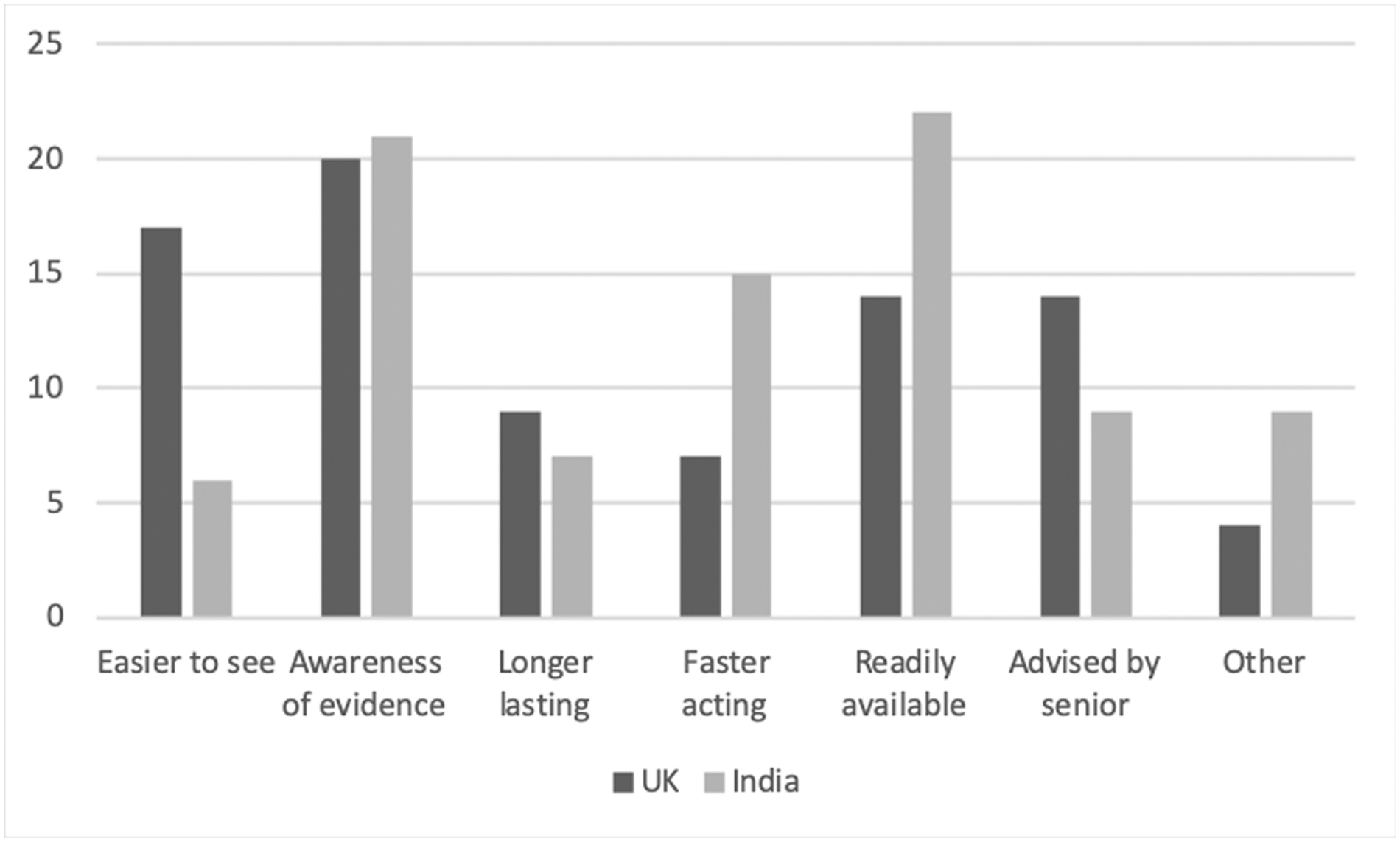
Surgeon's reason for their antiseptic choices in the United Kingdom and India. Surgeons were asked to indicate all reasons that applied to their choices.
Sub-analysis comparing antiseptic use in terms of specialty revealed general surgeons in India preferred the use of CHG over other preparations (p = 0.008), an effect not observed in the United Kingdom (p = 0.69). Head and neck surgeons in India preferred the use of PVP-I over CHG (p = 0.041). There were no statistically significant differences observed for other specialties, in either the United Kingdom or India, exhibiting preference for one preparation over another.
Discussion
Our study reveals that in India, CHG was preferred compared with other surgical site preparations. In the United Kingdom, this outcome was not observed. Adherence to WHO guidance was therefore more likely to be followed in India compared with the United Kingdom, with the exception of head and neck surgeons in India who preferred the use of PVP-I over CHG. This could potentially be because of the reported ototoxic effects of CHG [13]. This study concluded CHG toxicity to be related to intra-operative contact time with the round window, however, 10 of the 12 included studies were animal models. A more robust systematic review found “some” evidence suggesting an ototoxic effect of CHG, however, deemed this to be weak. Furthermore, the study also reported an ototoxic effect with PVP-I [14].
The reason for surgeon's choices was found to be inconsistent and therefore is unlikely to represent a true knowledge of the individual qualities of each preparation. For example, it has been reported that CHG has a more rapid onset of action, persistent activity, and residual effect compared with PVP-I [15]. Despite surgeons in India showing a preference for CHG over other preparations and surgeons in the UK not exhibiting this, the lack of statistical difference between surgeon reasoning suggests that surgeons are unaware of the qualities of each preparation they are using. This reinforces the concept that surgeons should adhere to guidance with respect to antiseptic choice, because their current reasoning seems misinformed to an extent.
Another important attribute of preparations is their cost. It is unlikely that this would be a major contributory factor in surgeon decision-making but may influence the availability of preparations in hospitals (although this effect was not observed in this study). Whereas CHG is more expensive than PVP-I, cost analysis has shown it to be more cost effective overall because of its greater reduction in SSI rates [16]. The data from India was collected from a quaternary hospital in Kochi, Kerala. This institute is privately funded and well-resourced and may stock more CHG to push for its use over other preparations because of its reported cost-effectiveness. This effect may not have been observed in a government hospital in India. Despite this, there was no substantial difference in surgeons in India or the United Kingdom choosing “readily available” as their reason for preparation choices (p = 0.232).
It is therefore unclear why surgeons in India were more likely to adhere to CHG usage compared with surgeons in the United Kingdom in this cohort. The difference is unlikely to be attributable to variance between surveyed surgical specialties or grades because these baseline characteristics were well matched between centers. It is possible that U.K. surgeons prefer other preparations compared with CHG because they were “easier to see” (p = 0.016). Povidone iodine is generally a dark substance compared with CHG, which is light pink. This is assuming, however, that surgeons find this dark color easier to see, which was not specifically surveyed.
Further analysis of the WHO guidance [17] reveals the use of six trials comparing CHG (alcohol) to PVP-I (alcohol), which showed a significance in terms of CHG. However, one trial compared CHG with PVP-I that had a lower concentration of known effective microbicidal (23% isopropanol compared with the established 50%–90%) [18]. In addition, there were two trials that used preparations with unknown alcohol concentrations [19,20]. Nevertheless, post hoc analysis adding more recent trials to the WHO meta-analysis showed a continued superiority of CHG over PVP-I (odds ratio [OR] 0.73, 95% CI. 0.55–0.97) [21].
Despite the questions raised regarding the evidence incorporated in WHO guidance, we believe that CHG should be implemented, where possible, over other surgical site preparations. Changing surgeon's mindsets is difficult. Practice is influenced by many factors including preference, routine, and personal clinical outcomes [22,23]. If surgeons perceive their SSI rates to be low, they may not recognize a need to change their practice.
Although our survey incorporated a wide variety of surgical disciplines and grade, the results are likely limited by low numbers of responses. To gain a better global perspective of surgeon preferences, more centers from different countries would have to be examined. This would improve the power of statistical analysis and validity of conclusions drawn. Furthermore, limitations posed by survey-based research applies to this dataset such as selection bias and duplicate respondents. We have tried to minimize these effects where possible by approaching the majority of surgeons in both centers [24].
Conclusions
This study compares the preferences of surgeons across multiple disciplines and grades in different countries. In general, it shows a reduced compliance of U.K. surgeons with WHO guidance for antiseptic use surgical site preparation compared with surgeons in India. The reasons for this are varied but are unlikely to be related to the properties of the available preparations. We know it is challenging to change surgeon-specific preferences and practice, but we believe the simple change of CHG use as primary antiseptic should be implemented where possible to minimize the global SSI burden.
Although the WHO has attempted to summarize the existing data to minimize the previous uncertainty surrounding antiseptic choices, it is clear that CHG is still not being adopted widely. To draw robust conclusions to provide the foundations of further guidelines, future research should focus on prospective RCTs with large numbers across multiple surgical specialties. This will provide high-quality data for surgeons around the world to make informed decisions regarding their surgical site preparation choices.
Footnotes
Acknowledgments
We would like to acknowledge the centers from which our data were collected: Royal Wolverhampton NHS Trust, New Cross Hospital (United Kingdom) and Amrita Institute of Medical Sciences, Kochi, Kerala (India).
Author Contributions
K.K.G. was responsible for the initial idea, writing, and submission process of the manuscript. D.V. and M.M. were involved in the writing and submission process of the manuscript. V.X. and J.M. were involved in data collection and manuscript editing.
Funding Information
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No commercial associations, competing financial interests, or conflict of interest to disclose from all authors.