
Abstract
Background:
Vascular infections are rare and challenging conditions with significant deaths and morbidity. Their management necessitates a multi-disciplinary approach and substantial human and financial resources. The management selected may be influenced by the available resources in low- and middle-income countries (LMICs), where such resources may be variable.
Methods:
We reviewed the published literature and reviewed the management options for various vascular infections with a focus on carotid, aortic, infrainguinal, and dialysis access infections.
Results:
Recommendations related to prevention and treatment will be offered from the perspective of LMICs. The general principles for prevention are in compliance with established surgical site infection guidelines and minimize the use of prosthetic material. Early detection and intervention by removing all infected prosthetic material, debridement, drainage, and coverage of the infected field with vascularized tissue are essential steps in the management of the infection. Revascularization using an extra-anatomic or in situ approach is individualized based on the resources and expertise available.
Conclusions:
The prevention and management of vascular infections in LMICs are effective by adhering to time-proven principles even with limited resources.
The care of the vascular patient has changed significantly over the past two decades. Endovascular technology has offered many less invasive alternatives to open vascular surgical procedures with increased utilization of stents, covered stents, and endografts, some placed percutaneously and others using open access or hybrid techniques. Advancement in prosthetic material, supported by various studies suggesting improved performance [1–5], has led to increased acceptance by surgeons for the utilization of prosthetic patches and vascular grafts.
In addition, advancement in renal replacement therapy has resulted in increased utilization of short- and long-term catheters for hemodialysis [6]. Further, despite the approach of “fistula first” in hemodialysis access, many patients with no available or suitable veins are undergoing placement of arteriovenous prosthetic grafts [7]. This increased utilization of a wide variety of patches, grafts, stents, covered stents, and catheters has opened the gate to a wide spectrum of potential vascular infections [8,9].
Vascular infections are rare and challenging conditions that can result in significant deaths and morbidity [10]. Their management can be complex, often requiring multiple stages and interventions and a multi-disciplinary approach including vascular surgeons, interventional radiologists, infectious disease specialists, plastic and general surgeons. The management can also necessitate numerous resources and can be taxing on the patient and institution. In the Western world and even in the best of hands, the outcomes of their management can be vexing and with high morbidity and deaths, resulting in various approaches for management [11,12]. The management can also vary depending on the available resources.
In this article, we will review the variable aspects of vascular infections and the possible variations in care imposed by the resources available in low- and middle-income countries (LMICs) from prevention to management.
Classification of Vascular Infections
Vascular infections can be classified according to location, onset, and extent. Vascular infections occurring in the chest or abdomen are cavitary infections, while those occurring in the neck or extremities are considered extra-cavitary. Early vascular infections are those seen within the first four months after the vascular intervention, while those seen later are considered late vascular infection. Suggestions have been made to also create an additional category of subacute for those infections appearing between one month and four months [8].
Early vascular infections are characterized by redness, pain, and draining wounds while late infections may have a more insidious onset. The extent of the vascular infection is variable. Szilagyi et al. [13] provided the first vascular infection classification based on the extent of the infection: Stage 1, when the infection is limited to the skin, stage 2 when it extends into the soft tissues yet sparing the graft, and stage 3 when it involves the underlying graft. When the graft is involved, it may still be covered by the surrounding tissues or may become exposed (Table 1).
Infection Classification
The infection can be limited to a segment of the graft or can involve the entire graft including the suture lines or anastomoses. Involvement of the suture lines is very dangerous because, depending on the duration and the infecting organism, it may lead to pseudoaneurysm formation, dehiscence, and anastomotic rupture and bleeding [8]. As such, several classifications have been proposed to describe further the extent of the infections, such as the Samson classification [14], developed for vascular groin infections in particular (Table 1).
Graft involvement extent was also categorized as per the Bunt classification [15] into four groups that differentiated between cavitary graft infection (P0), non-cavitary graft infection (P1), extra-cavitary portion infection of a graft whose origin is cavitary (P2), and prosthetic patch angioplasty infection (P3) (Table 1). Vascular infections also may occur without a surgical intervention, secondary to a hematogenous spread causing a mycotic aneurysm [16] or after a penetrating trauma and superimposed infection causing an infected pseudoaneurysm [17].
Clinical Presentation
Patients with early infections typically present with pain; also seen are redness and hotness along with purulent discharge. Left inadequately treated, the condition may progress to sepsis or hemorrhage. Patients with late infections may present with a draining sinus, enlarging pulsating mass if extra-cavitary, or insidious onset of fever, signs of sepsis, septic emboli, or even gastrointestinal bleeding, which may be mild in graft enteric erosions or massive in graft enteric fistulae. In early infections, the entire graft tends to be affected, while in the late infections, the graft may be partially or totally involved [18].
Etiology
The infection can occur because of contamination of the graft from the skin or transected lymphatics, especially in the presence of remote infections. It may also be because of a contamination and break in the sterile techniques in the operating room, or contamination from an iatrogenic bowel injury. The infection may also occur because of direct spread and extension from a surrounding soft or deep tissue infection. The graft may also be seeded from bacteremia related to remote infections such as urinary tract infections, foot infections, or even periodontal infections.
Predisposing factors include patients with diabetes mellitus, patients with decreased immunity, non-adherence to antibiotic prophylaxis guidelines, wound hematomas, complex operations, prolonged operations, re-do procedures, and emergency procedures [19,20]. Procedures that involve groin exposures are also more prone to infection, especially in overweight patients [21].
Other factors include creation of skin flaps, ischemic wound closure techniques, and not abiding by the typical surgical site infection (SSI) prevention recommendations [22]. These include peri-operative antibiotic coverage within one hour of skin incision, hair clipping instead of shaving, peri-operative glycemic control, and avoidance of hypothermia. Prepping using alcohol-based antiseptic solutions with chlorehexidine or iodophores (povidone iodine) is more effective in reducing the risk of SSI compared with aqueous iodophores solutions frequently used in developing countries. Draping techniques—the use of iodinated skin protective barriers (Ioban)—have also been recommended for SSI prevention in vascular procedures [23].
Every effort should be made to prove microbiologic infection when suspecting vascular graft infection [24]. This can be achieved directly through operative sampling and peri-graft fluid sampling assisted by ultrasonography (US) or computed tomography (CT) guidance or indirectly through blood cultures, wound specimens, and draining sinus cultures. The infective organisms include gram-positive cocci and gram-negative rods. Staphylococcus aureus is typically the most common pathogen in device-related infections [25].
There has been a rise in S. epidermidis and gram-negative bacterial infections, such as Pseudomonas, Escherichia coli, Klebsiella, Enterobacter, and Proteus [26]. These organisms tend to produce various toxins such as elastase and alkaline protease that can lead to breakdown of the arterial wall, anastomotic disruption, and bleeding. The S. epidermidis infection is typically a chronic peri-graft infection because of biofilm and slime producing infection, which tends to isolate the graft from antibiotic treatment. As a result, there is poor incorporation of tissue in the graft, and special “US disruption” techniques may be needed to isolate the organism [27].
In early vascular infections, the offending organisms are typically S. aureus and gram-negative bacteria and tend to be more aggressive and virulent. Occasionally, skin flora bacteria, such as streptococci and Propionibacterium acnes, can also be the organisms responsible for vascular infections [28].
General Principles of Management
Post-operative SSI in a patient who underwent a vascular procedure remains a concern to all surgeons. Pre-operative antibiotic coverage according to standards is essential to all, along with discontinuation of antibiotic prophylaxis when not needed. Wound erythema and tenderness or discharge are typically managed with intravenous antibiotic therapy along with investigations to determine the extent of the infectious process (Fig. 1). In extra-cavitary infections, US is very valuable to determine the presence of any fluid collection under the skin and its relationship to the vascular bed and graft [29].

Groin infection with erythema.
The presence of a skin and soft tissue infection that is managed typically by simply opening the wound, draining the infection, and wound care, can result in a disastrous effect in a vascular patient if a graft is exposed or involved. In addition, the management may be variable, depending on whether a prosthetic or autogenous graft or patch is used in that specific patient. In general, an autogenous graft or patch may be more resistant to infection and may be managed by draining any associated fluid collection, wound debridement, and coverage by a healthy vascularized muscle [30].
If the infection has reached a prosthetic graft, the treatment is typically graft excision, especially if the anastomosis is involved. Partial graft excision may be possible if the graft infection is limited to a graft segment and the anastomoses are spared [31]. When the graft is excised, usually there will be a need for another re-vascularization procedure to maintain the circulation that existed before graft removal. Such revascularization may be planned using an extra-anatomic approach through uninfected tissue, preferably before graft explantation to decrease the degree of ischemia.
Occasionally, in situ graft replacement may be performed, which carries the risk of repeated infection. Adequate drainage and debridement of the infected area is performed along with graft removal. Prolonged antibiotic coverage guided by intra-operative wound and graft culture results will be an essential part of the management.
The management of vascular infections in LMICs follows the same principles as wealthier countries but may encounter some constraints related to the available resources and expertise. Diagnostic tools such as US disruption of the specimen for the diagnosis of S. epidermidis infections may not be available readily. Similarly, radiologic imaging such as tagged white cell scanning, positron emission tomography, CT scanning, or other expensive modalities may not be available readily. Special grafts used in the management, such as silver coated grafts, rifampin soaked, cadaveric, or bovine grafts may not be accessible readily.
In the following sections, specific vascular infections will be presented and potential management adaptations imposed by the possible variations in resources available in LMICs will be discussed.
SSI after carotid operation
An SSI after a carotid surgical procedure is a rare event, similar to most cervical operations. It is reported in the literature as less than 1% [32]. Typically, when carotid surgical complications are mentioned, the focus is on the neurologic and cardiac events rather than infection. Nonetheless, the seriousness of this complication is associated in general with carotid patch infection, and the separation of these entities is difficult.
In one of the largest series reported of 4,000 cases performed over a 10-year period, there were 25 patients re-admitted for SSI, and diabetes prevalence was 44% [33]. The most common presentation for patch infection varied between neck swelling with pseudoaneurysm formation or draining sinus and purulent discharge (Fig. 2). The extent of the infection impacts further management and can follow the Szilagyi classification (Table 1).

Draining sinus after carotid endarterectomy because of chronic patch infection.
The world literature counts today 132 cases of reported carotid patch infection [34]. Predisposing factors include early SSI, operative contamination, wound hematomas, diabetes mellitus, and upper respiratory tract infection. As for the timing, there was a bimodal distribution—50% occurring within the first three months, largely related to post-operative wound infection, or contamination with highly virulent organisms [35].
Bacteriology
The microbiologic epidemiology is affected by many factors. These include prophylactic anti-staphylococcal antibiotic agents, developments in surgical techniques, performing operations on patients with several underlying comorbidities, evolution of the flora in hospitals [36]. Of the reported cultures, 91% were gram-positive cocci (S. aureus and S. epidermidis; some strains of methicillin-resistant S. aureus [MRSA]) [31,32,35]; the remaining culture results are divided between Enterobacter, Pseudomonas, Bacteroides, Proteus, coliforms, Enterococcus, Corinebacterium. Of note, 20%–30% of culture results were negative or not reported in the large series.
Management
Prophylactic antibiotic agents for the original operation follow standard hospital protocol for all clean vascular operations, in general covering gram-positive organisms. In the eventual suspicion of SSI, whenever possible and with any discharge or draining sinus, cultures should be taken in addition to blood cultures. Broad-spectrum antibiotic agents are initiated and re-adjusted as per culture results. Treatment varies between conservative with exploration, washout, drainage, and long-term antibiotic agents to a more radical approach with patch excision, artery debridement, and vascular reconstruction [33].
The radical approach typically is unavoidable in the presence of suture line involvement or dehiscence. Once the patch is removed and the artery debrided, the options will depend on the remaining segment of the debrided artery. The reconstruction may be achieved by placing another patch sutured to healthy debrided artery. The patch used in this setting is preferentially an autogenous vein. If the infection is extensive, an interposition vein graft may be necessary. Muscle flap coverage typically using the sternocleidomastoid muscle is an integral part of the procedure. Reconstruction with prosthetic material has a high rate of complications and should be avoided [34,37–39].
In regions with limited resources, the focus should be first on prevention. When patch material is to be used, we suggest autogenous vein when available in the original carotid procedure, which would both be cost effective and reduce the risk of prosthetic patch infection. Another alternative is to become familiar with the eversion endarterectomy technique, which avoids using a patch altogether. Once infection occurs, every effort should be made to replace all prosthetic material with autogenous reconstruction, which should be possible irrespective of the country's income classification.
Thoracic aortic and thoracoabdominal graft infection
These infections are associated with high morbidity and death. Patients with these infections may present with sepsis, empyema, esophageal bleeding, or bleeding in the thoracic cavity. Extra-anatomic bypass is not an option in these patients, and the surgeon typically is forced to replace the infected graft by another prosthetic graft or cadaveric graft if available [40]. In case of thoracic graft infection from aorto-esophageal fistula, excision of the infected material, esophageal repair, and viable tissue coverage is recommended [41,42].
There is no universal consensus on the appropriate management of thoracic aortic graft infections; however, it is essential to drain all peri-graft fluid collections and excise the graft in its entirety with all infected field surgically debrided back to healthy tissue [43]. It is important to remove all infected graft material because bacteria have an ability to form biofilms refractory to medical management. Occasionally, in the presence of an unstable patient with major bleeding and aorto-esophageal fistula, a thoracic endograft may be used as a temporary measure to stabilize the patient to conduct the definite resection days later when the patient is stable enough [44]. Rerouting is an option in selected cases with ascending to supra-celiac aortic bypass through the right pleural space.
In the case of graft infection, preservation techniques should be limited to patients with excessive operative risk for graft excision and replacement. In LMIC, the availability of cadaveric grafts may be limited. Similarly, the prompt availability of thoracic endografts as temporizing measures in emergency bleeding situations and the financial implications of using such engografts as a bridge to definitive therapy will limit the utilization of such options, especially when not covered by third party payers.
Abdominal aortic graft infection
This condition is the nightmare of every vascular surgeon. The incidence of aortic graft infection varies, depending on the type of procedure, with an increase in rate if involving a femoral anastomosis. The management also varies if the graft is an aortic graft, aorto-bi-iliac, or aorto-bifemoral bypass. The graft management also varies if the infection involves the limb of the graft with sparing of the body of the graft, or if the graft body is involved. In addition, the management varies if the original procedure was placed for occlusive or aneurysmal disease.
One of the main issues in aortic infection is establishing the diagnosis. The presence of an exposed graft in the groin, or the visualization of a graft during upper endoscopy can make the diagnosis certain (Fig. 3). In many patients, however, the presentation is more indolent. A CT scan with an arterial phase is an essential tool for diagnosis. The presence of fluid around the graft is greatly suspicious for a graft infection. Infection becomes even more certain if gas is also seen around the graft or in the peri-graft fluid collection (Fig. 4). Very rarely, needle aspiration under CT guidance may be necessary to establish a diagnosis and identify the infective organism.
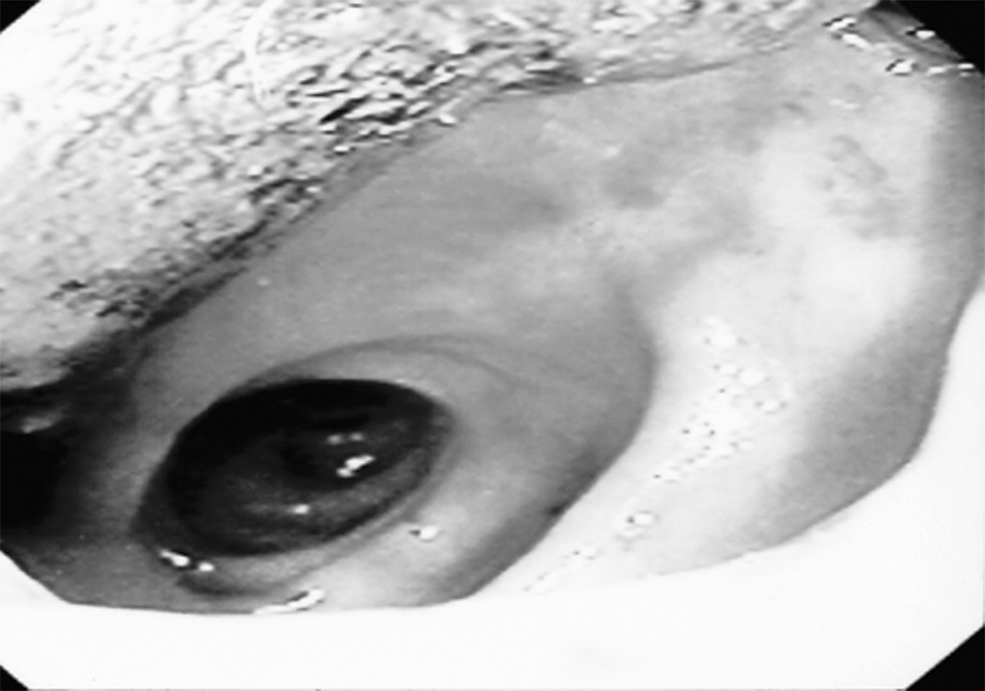
Endoscopy showing abdominal aortic graft erosion into viscous lumen.
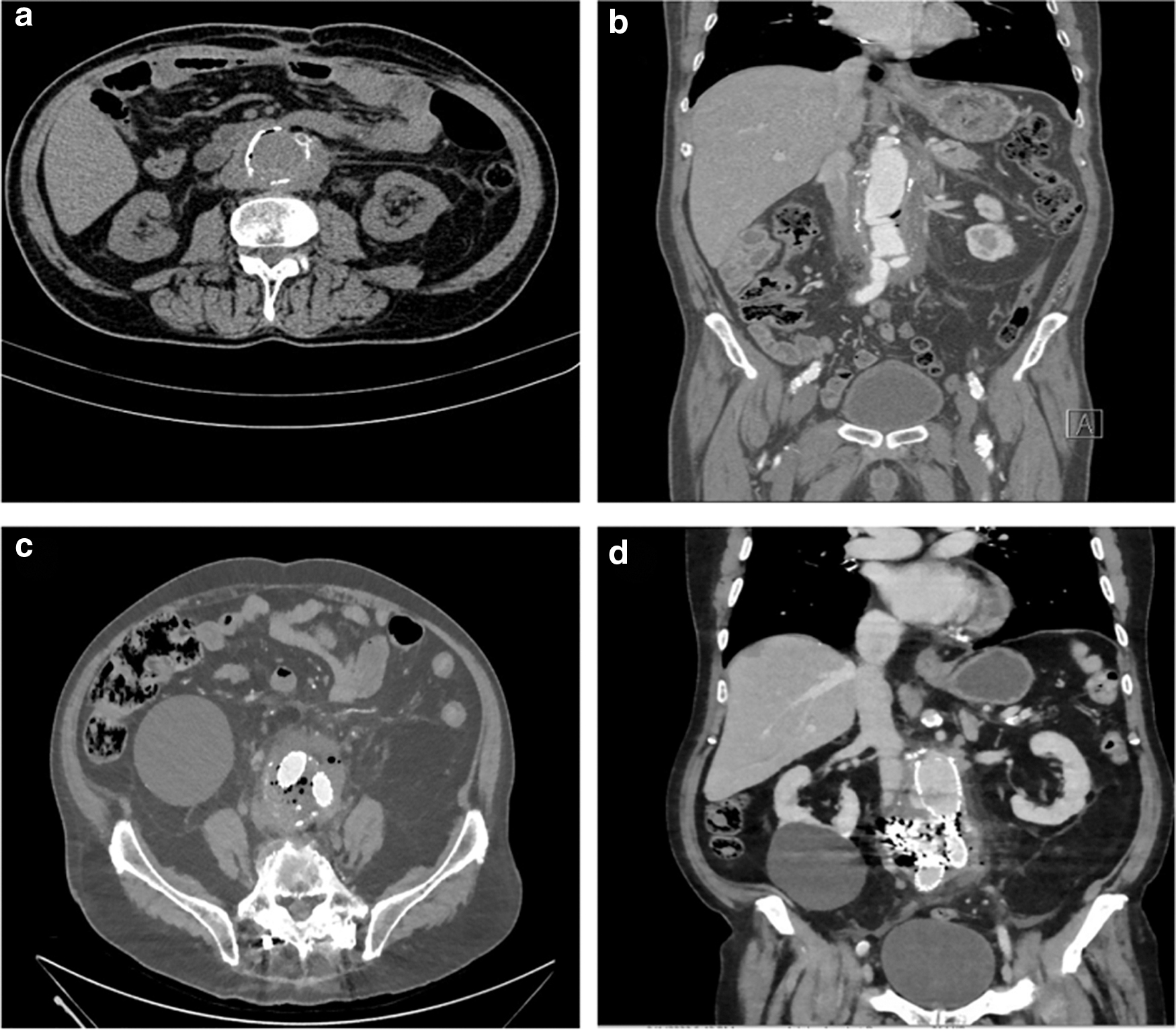
Computed tomography (CT) scan suggestive of aortic graft infection post-open repair in axial
More recently, a PET CT scan has turned into a modality of choice for diagnosing aortic graft infections [45,46]. Such modality may not be available readily in LMICs, and the treating physicians may have to be limited to the CT scan diagnosis. Other technology, such as white cell nuclear scanning, may be available in LMIC and may be diagnostic by showing increased uptake of tagged white cells (Fig. 5) [47]. Occasionally, a fistulogram and injection of dye into a draining sinus may also help in establishing the diagnosis. Very rarely, the diagnosis is only made at exploration, which typically reveals a non-incorporated graft with bile staining when there is an associated enteric fistula or erosion as shown in Figure 6.

White cell scan showing increased uptake in the left iliac region and left groin.
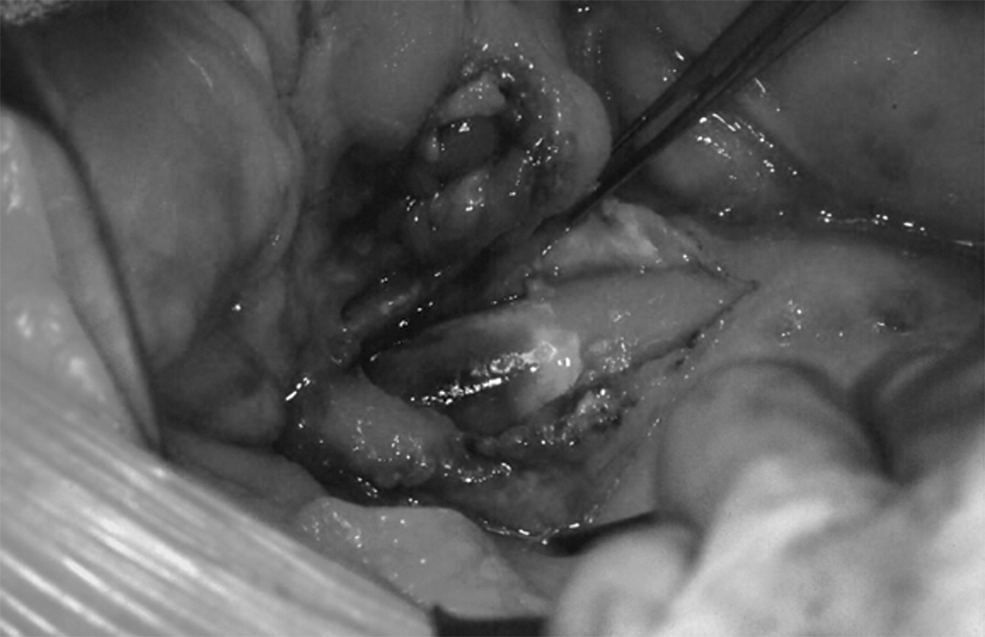
Bile stained graft and a duodenal defect.
Once the diagnosis of graft infection is made, it is very essential to determine the extent of the infection and identify whether the infection is limited to the groin and limb or whether it involves the body of the graft. One of the mainstays of aortic graft infections is removal of the infected aortic graft. Less invasive techniques have been described, such as use of life-long antibiotic agents, incision and drainage of the infected fluid without graft removal with irrigation with antibiotic agents [48]. The definitive treatment, however, involves graft removal. The treatment options are variable and include a single- or two-stage procedure. In the two-stage procedure, two options also exist—revascularization followed by graft removal in the same setting or revascularization followed by graft removal few days later [49].
If the infection is limited to the groin and femoral limb, an extra-anatomic bypass (axillo-femoral bypass) through a lateral approach to the profunda or superficial femoral arteries is conducted first. This is then followed by a retroperitoneal incision in which the graft is identified and transected close to its origin. Presence of incorporated tissue is usually a good indication that the graft infection is limited to the groin. The peritoneum over the proximal part of the limb is then closed, isolating the graft from any infection. The distal limb is pushed down toward the groin, and graft cultures are performed. The retroperitoneal incision and wounds are then closed. The groin incision is then addressed, and the graft is dismantled from the artery. The arterial wall is debrided and then closed, preferably primarily or by an autogenous patch if primary closure is not possible. The graft is then covered by any adjacent vascularized tissue or by a muscle flap.
Another alternative for the femoral infection is to expose the abdomen and identify the limb and transect it and connect to a graft tunneled through the obturator canal away from the infected field to the suprageniculate popliteal artery. Both surgical options can be implemented in LMICs.
If the aortic graft body is involved, then the management becomes more complex. If an aortic graft proximal anastomosis was conducted in an end to side manner, the graft may be dismantled followed by primary aortic closure [50]. Additional revascularization may not be needed. If the proximal anastomosis was conducted in an end to end manner, the excised graft will need to be replaced. The options here include in situ replacement with rifampin-impregnated graft or silver-coated graft, cadaveric graft, bovine graft, or femoral veins.
The main concerns of in situ replacement are sepsis and persistent or recurrent infection that could affect the new graft especially because it will be placed inevitably in the bed of the previous infected aortic graft. Despite all the debridement possible and coverage with healthy omentum, that field is contaminated and so are the instruments used while performing the reconstruction. The use of rifampin-soaked prosthetic grafts or silver-impregnated grafts is thought to decrease the chances of such infection [51]. The use of cadaveric aortic allograft was instigated to decrease this possible infection. Those, however, may not be available in many of the LMICs.
Similarly, the in situ aortic neovascularization (ISAN) with femoral veins was conceived to create an all autogenous aortic bypass. The option of an autogenous graft from harvested femoral veins, a procedure originally described by Clagett et al has gained acceptance [52]. In this procedure, the femoral veins are harvested preserving the great saphenous and the deep femoral veins, which will provide lower extremity drainage. The technique is tedious and time consuming and often necessitates two teams with one working on the vein harvesting and neoartic graft preparation while the other team is working in the abdomen. The lower extremities typically will suffer from post-operative edema that resolves in few months with elastic compression stockings [53]. Occasional patients may need lower extremity fasciotomies because of the associated swelling.
The advantage of in situ replacement is revascularization with an in-line reconstruction and avoiding the concerns of an aortic stump blowout. This dreaded complication may occur in patients in whom the aorta was transected and an extra-anatomic revascularization using an axillo-bifemoral or bilateral axillo-femoral bypasses is chosen for re-establishing flow to the lower extremities. The aortic stump is typically oversewn in two layers and covered with a healthy omental flap [54,55] (Fig. 7). A pedicled latissimus dorsi flap can be used to cover an aortic stump and is reported in the literature. Revascularization of the lower extremities preferably is performed before the aortic graft excision to minimize the degree and duration of ischemia to the lower extremities [56].

Aortic stump coverage:
Experience with ISAN is limited to some centers. A bovine graft is also becoming an option [57]. This option, however, is not available readily in LMICs. The advantage of extra-anatomic bypass is the removal of all infected tissues from the abdomen and not leaving behind any potential source of infection. The Achilles heel of this procedure is the adequacy of the aortic stump. If the aortic procedure originally was performed for a juxtarenal aortic aneurysm, the quality of the aortic tissue remaining available to close the stump in two layers is limited and any persistent infection can lead to stump blowout. There is typically a need for at least 1–2 cm of healthy infrarenal aorta to secure a reliable aortic stump closure.
Debranching of the renal arteries using hepatorenal and splenorenal bypasses has been described to generate a healthy aortic stump; however, this will turn into a formidable operation in typically a high risk critically ill patient, making an in-situ replacement attractive despite the risk of recurrent infection.
Another concern is the patency of the axillo-femoral bypasses and possible lower limb amputation. The results have been mixed, although excellent results have been reported [58]. The infectious organism also plays a significant role in the outcomes. Gram-negative infections are more prone to develop into recurrent infection, sepsis, or stump blowout [49]. Gram-positive infections with S. epidermidis are more likely to be responsive to in situ graft replacement.
Another integral part to the success of the procedure is proper closure of the enteric fistula where typically the third part of the duodenum is involved. A failed duodenal closure can result in a duodenal leak with persistent sepsis and a poor outcome [8,59]. Primary duodenal closure may be possible, and occasionally excision of a segment of duodenum with re-establishment of bowel continuity will be necessary. Hence, the need of multi-disciplinary teams and an experienced gastrointestinal surgeon to handle the duodenal fistula repair.
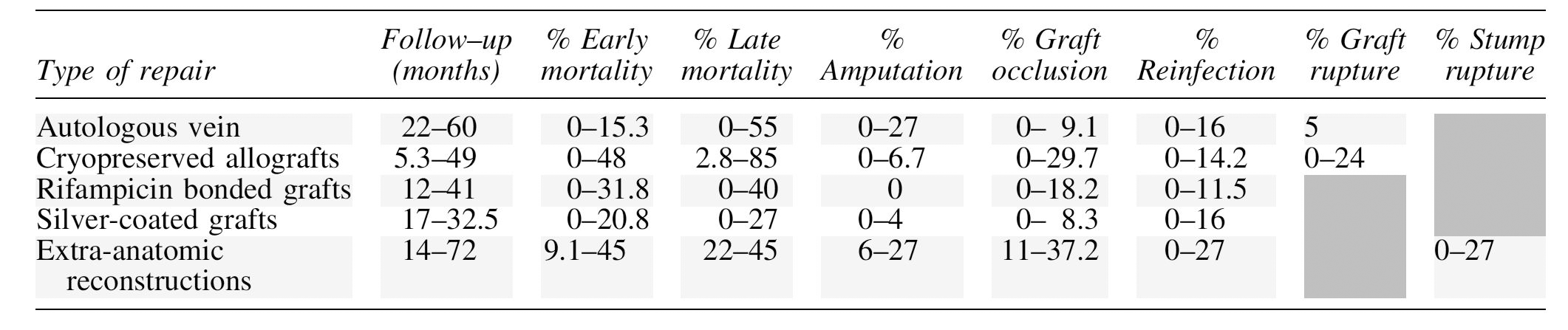
The outcomes of the management of aortic graft infections are viewed typically in relation to death, persistent sepsis, stump or suture line blowout, leg ischemia, and amputation. Table 2 summarizes a range of outcomes with respect to follow-up time, early and late death, amputation rate, graft occlusion, re-infection, graft rupture, and stump rupture. The European Society of Vascular Surgery 2020 proposed an algorithm for the management of aortic vascular graft/endograft infection based on differentiating between acute bleeding and surgical fitness [60]. The resources available will determine its applicability in LMICs.
Range of Outcomes
Endovascular aortic repair (EVAR) infection
The management of aortic endograft infections post-EVAR follows the same principles as open aortic graft infection (Fig. 4). Some may be because of graft contamination while others may occur in combination with an aorto-duodenal fistula. The most definitive management involved graft explanation with reconstruction using in-situ replacement or axillo-femoral bypass with aortic ligation. The choice for graft used for the in-situ reconstruction is similar to that for open aortic graft infections. The graft can be a silver-impregnated, rifampin-soaked, or cadaveric, or using neoconstructed femoral veins [60]. Results of cadaveric grafts and ISANR have been promising.
The situation can become even more complex if a fenestrated or branched graft is infected; typically this will necessitate an even more extensive surgical procedure with renal and visceral bypasses [60]. A less invasive approach with open abdominal exploration and evacuation of the sac with antibiotic irrigation without graft explanation has been described with suboptimal outcomes or mixed results [61]. The management of aortic graft infections in LMICs will be guided by the available resources. Cadaveric aortic grafts are readily available in some countries with advanced transplantation and organ donor programs. The expertise needed to conduct an ISANR may not be available in some LMICs.
Femoral mycotic pseudoaneurysm
Infected mycotic pseudoaneurysms may occur after intravenous drug abuse to the groin. They can also occur as a secondary infection of a pseudoaneurysm that develops from an interventional procedure after a groin puncture for a cardiac catheterization or lower extremity angiography or intervention. The management typically involves evacuation of the pseudoaneurysm and associated thrombus and debridement of the involved artery and restoration of arterial flow.
If the defect in the artery is small, it may be amenable to primary repair. If large, a vein patch repair after good arterial wall debridement may be necessarily followed by coverage of the repair with healthy tissue or a local sartorius muscle flap. If the defect in the artery is extensive, then excision of an arterial segment with reconstruction may be necessary. An autogenous vein graft is then used for a bypass.
Occasionally, if the infection involves the common femoral artery with preservation of the common femoral bifurcation, a segment of the common femoral artery is excised. The proximal end is oversewn in two layers. The distal end is also oversewn while preserving the profunda femoris artery. Retrograde flow from the femoris artery into the superficial femoral artery may provide adequate flow to the lower extremity, and an additional bypass may not be necessary [62].
A femoral pseudoaneurysm in the presence of a graft typically is an infected pseudoaneurysm until proven otherwise. The pseudoaneurysm may be the distal femoral anastomosis of an aorto-bifemoral bypass, and its management was covered in the previous section. The pseudoaneurysm in the proximal anastomosis of an infrainguinal bypass will be discussed in the section below on infrainguinal graft infections.
Infrainguinal graft infection
Despite the wide adoption of an endovascular approach first to manage lower extremity occlusive disease, infrainguinal revascularization with bypass procedures is still widely and commonly performed, especially in average risk patients with a good available great saphenous vein or in patients with failed repeated endovascular interventions.
Advances in polytetrafluoroethylene (PTFE) manufacturing with heparin-bonded technology and encouraging results of such grafts to the above knee and even below knee location with results comparable to vein bypasses on the short term have been presented [63]. Many of these patients tend to have diabetes mellitus with a large panniculus and are prone to wound complications.
Wound complications in the presence of an infrainguinal bypass can be managed according to the location and degree of infection. Important considerations are the type of bypass, whether prosthetic or autogenous, and the tunneling techniques for the bypass. In-situ bypasses are notorious for having a higher rate of wound complications [64]. Lower extremity US can add valuable information about the infectious process, the presence of fluid collection around the graft, and also can provide guidance for any needle aspiration of fluid to determine and identify an infective organism.
It is very important to determine whether the graft is involved with the infection or whether the infection is limited to the soft tissues. If the infection extends to the graft, it is important to clarify whether the infection involves the body of the graft or whether it included or involved the anastomotic suture line. If this is an early post-operative infection, an attempt at evacuating any fluid collection, placing drains or draining catheters, intravenous antibiotic agents, coverage with muscle flaps, and avoiding any dead space can be tried initially.
Irrigation in adjunct to negative pressure wound therapy is also considered in such cases and in patients unfit for major procedures [65]. This can be a successful measure if the bypass is an autogenous vein. If the bypass is a prosthetic graft, drainage and antibiotic therapy can be tried but will unlikely be successful. Graft excision is more likely to be required to provide a definitive treatment.
If the infection is limited to the body of the graft, exploration of the graft in uninvolved areas proximal and distal to the infection or exposed graft is performed through separate incisions. An interposition graft is then created and passed through a new tunnel away from the previous graft. After wound closure, the infected area is opened, and the infected segment is pulled from that incision. The incision is kept open for healing with secondary intention or with the help of a negative pressure dressing. Antibiotic therapy is provided guided by intra-operative culture results.
If the infection involves the suture line of the proximal or distal anastomosis, the entire graft will need to be removed. Most often, a new bypass will be needed with autologous vein using an inflow proximal to the currently used one and outflow vessel distal to the distal anastomosis. The bypass typically is tunneled through a non-involved area. In cases of infection with MRSA, Pseudomonas, or multi-drug resistant bacteria, extra-anatomic routing becomes particularly suggested as recommend by the European Society for Vascular Surgery 2020 clinical practice guidelines on the management of vascular graft and endograft infection [60].
A lateral approach to expose the inflow and outflow vessels can be very valuable and limb saving and will allow tunneling through a non-infected field [66]. The defect in the arteries at the level of the previous anastomoses is typically repaired primarily or occasionally with a vein patch. Very essential to the management is coverage of the anastomoses or suture lines by vascularized tissue or muscle flaps. Antibiotic coverage guided by the intra-operative culture results is mandatory.
In the absence of saphenous veins, a composite arm vein may be constructed. If an all autogenous graft is not possible, a cadaveric vein may be used. The results of infrainguinal cryopreserved cadaveric veins are comparable to those of prosthetic grafts with respect to patency rates, but they can present a very good bailout option in the presence of a bad infection, especially when autogenous vein is not available. Again, in LMICs, such cadaveric grafts may not be available readily. All other treatment options are likely to be available in LMICs.
Hemodialysis access
The Kidney Disease Outcomes Quality Initiative guidelines have stressed the importance of a fistula first as an access site for patients needing hemodialysis [7]. Nevertheless, when an arm vein is not available and all options for a suitable autogenous arteriovenous fistula have been exhausted, a prosthetic arteriovenous graft is inevitable. One of the main drawbacks of prosthetic arteriovenous grafts is the high rate of infection in comparison with an autogenous arteriovenous fistula. The infection can be insidious with signs of sepsis or can be obvious with clear signs of infection and redness, tenderness, and fever. A duplex scan is essential to the management and can show clear fluid collection around the graft.
Arteriovenous grafts can be lifelines, and every effort usually is made to prolong their lives and utilization. Once infected, however, the chances of preserving them dwindle [66–70]. Attempts at partial graft excision have been performed and may be successful at preserving the graft as long as the anastomoses are not involved. If an anastomosis is involved, total graft excision will be necessary. At the level of the arterial anastomosis, the options include leaving a rim of graft on the arterial anastomosis to simplify the closure versus dismantling the entire anastomosis and closing the arterial defect most often using a vein patch. Hemodialysis will be maintained using a temporary indwelling catheter. The venous anastomotic area is easier to handle because typically it lends itself to complete dismantling of the anastomosis and primary repair or closure of the vein defect.
The management of infected grafts in LMICs should not be different, with putting every effort for early site selection and autogenous access creation before the veins are exhausted during multiple admissions.
Tunneled hemodialysis catheter infection
Despite giant efforts over the past 15 years to limit the use of dialysis catheters in favor of fistulas, in the United States, catheters are still used for hemodialysis access in 80% of incidental end-stage kidney disease (ESKD) and 20% of prevalent ESKD [71]. Catheter-related blood stream infection (CRBSI) remains the most serious complication for those patients. Incidence of infection increases with duration of catheter use. Compared with arteriovenous fistulas, tunneled central venous catheters (CVCs) are associated with a 15-fold greater risk for bacteremia [72]. One study reports it to be 35%, 54%, and 79% at three, six, and 12 months, respectively. Overall, for tunneled-cuffed catheters, infection rates of about 0.5–5.5 events per 1,000 catheter days have been reported [73].
As per KDOQI, it is preferable to proceed with arteriovenous access in all patients initiated on hemodialysis and to reserve the CVC as a final destination for a few exceptional situations; in addition, if clinical and anatomic circumstances are amenable to good fistula maturation, an arteriovenous fistula would be favored over an arteriovenous graft [7].
The definition of CVC-related infection includes infection in a symptomatic patient with positive blood culture results and similar organisms cultured from a catheter segment (tip or hub). Presenting symptoms are fever and rigor, particularly during a hemodialysis session; symptoms of hemodynamic instability such as hypotension may develop during a dialysis session. Like any blood stream infection, if not treated promptly, this can lead to serious complication; sepsis, endocarditis, and septic embolization and osteomyelitis with spine infection are among the most reported.
Risk factors associated with increased risk of catheter-related infections include MRSA in a patient, history of catheter-related infections, in addition to bacteremia or urinary tract infections within the three months preceding insertion [73]. A study on emergency only dialysis patients, which may happen in a low socioeconomic status or non-insured population, using tunneled catheters showed a higher incidence than in patients with regular schedules; CRBSI was associated with prolonged hospitalization (mean, 15 days), a composite complication rate of 8%, and a 4% mortality rate. In addition, studies reported a consistently higher incidence of CRBSI in patients with associated liver disease [71,74]. About one third of patients with CRBSI will require admission (a slightly larger number with S. aureus infection). After confirmation of the CRBSI, initiating broad antibiotic agents is recommended, provided that treatment is shifted back to culture-specific agents when those are available.
Options in dealing with the catheter are several, including catheter salvage, replacement over wire, removal and placement of a new catheter, lock with antibiotic agents will depend largely on the virulence of the organism and the complicated nature of the presentation. Experts recommend catheter removal in the setting of hemodynamic instability, candidemia, resistant micro-organisms, or metastatic infections (5%–10% of patients) [71]. Because the majority (40%–80%) of organisms are gram positive, initial empiric treatment with vancomycin and ceftazidime is recommended until a more culture-specific antibiotic therapy can be initiated. If salvage of the catheter is attempted, adding antibiotic lock may help in clearing the infection [71]. In general, between two and four weeks of antibiotic agents is recommended with four weeks for S. aureus.
Recommendations regarding catheter care in relation to reduction of entry site and catheter infection are many; however, the following seems to be reasonable as per KDOQI and can be summarized as follows: Cleansing the site with chlorhexidine unless not available, use of an antiseptic barrier at the exit site at least until full healing, and avoiding exposure to wet or dirty environment, especially before full healing. The cost incurred by the healthcare system from CRBSI is elevated and can be as high as $40,000 in the United States; in a study performed in Italy through the Diagnosis Related Group system, dialysis with CVCt had +114% higher infection-related admission than those for arteriovenous fistula; with an average cost of Euro 5,575 (4,080–14,800), which was only one third of the same cost incurred in the United States [75].
In view of the high risk of complications and cost, tunneled catheters should not be considered a final destination in LMICs except in a few specific circumstances. Arteriovenous access is advised for long-term dialysis—and preferably fistula, when feasible. A strict protocol for early referral and protection of a potential extremity would help minimize catheter utilizations and their potential healthcare draining complications, especially in LMICs.
Peripheral venous catheters (PVCs)
More than 80% of hospitalized patients in the United States have one or more intravenous catheters placed during their hospital stay [76]. The PVCs are associated with increased risk of bacteremia in approximately 0.18% of inpatients, which increases with increased length of hospital stay, leading to increased healthcare costs [77,78]. The most common cause for PVC-related blood stream infections in a hospital setting is S. aureus, and most of these infections are underdiagnosed [79]. The PVCs placed in the antecubital area are 12 times more prone to cause infection than in all other placement locations. In addition, PVC duration of ≥4 days increases the risk by four times.
Placement of a PVC in the emergency department has an increased risk of 2.6 times compared with placement in inpatient units or the operating room, with males being more prone (2.3 times) to have PVC infection develop than females [80]. Infections of PVCs may lead to septic phlebitis that may necessitate incision and drainage and possible excision of the infected peripheral vein. In view of the increased numbers of PVC complications and costs, prevention of these complications is paramount [80].
Most complications associated with the use of PVCs are preventable [81]. Based on factors that contribute directly to PVC infections, various preventive strategies have been developed. Some traditional preventive measures are training and education of healthcare practitioners and patients, performance feedback, specialized intravenous treatment teams, hand hygiene, skin preparation, cutaneous antisepsis, use of sterile semi-permeable dressings, and documentation with peripheral cannula care plans [82–84].
Those in LMICs should try to minimize PVC placement in the antecubital area and line duration to reduce PVC infections and adhere to a strict policy of daily examination, with early removal when signs of infections become apparent, and ordering catheter segment cultures to detect the infected organism. The management should be coupled with the use of the appropriate antimicrobial therapy for the optimum duration of treatment according to the culture results [83].
Conclusion
Vascular surgical infections are notorious universally for their complexity and elevated morbidity and death worldwide. Those in LMICs are no exception. The cost burden in LMICs, however, weighs heavier on the already struggling healthcare system. As a general guidance, all efforts should be made toward prevention by using autogenous material when at all possible, in particular for infrainguinal bypasses, dialysis access, and patch procedures both for cost effectiveness and avoidance of infectious complications. Dialysis catheter usage should be limited to strict necessary, and an arteriovenous fistula should be constructed promptly if not performed preemptively; in aortic grafts, a low threshold for liberal use of omental flaps to provide good vascularized coverage of prosthetic material is needed.
Last but not least, prevention remains of the essence, in addition to early detection and intervention to prevent a small problem from becoming a major life- threatening condition. Once present, the infection is most effectively managed by explanting the infected prosthetic material and covering the infection with vascularized tissue. Revascularization using an in-situ or extra-anatomic approach will need to be individualized based on the resources and expertise available in the specific LMIC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.