
Abstract
Background:
Retroperitoneal infection is a persistent and widespread infectious disease that is difficult to treat. It is usually caused by secondary complications such as inflammation, damage, or perforation of adjacent organs in the retroperitoneal space. Pathogenic bacteria invade the retroperitoneal space through retroperitoneal and interstitial organs, peripheral tissue, and the blood. As a result, infections mostly arise from severe acute pancreatitis, acute colonic diverticulitis, inflammatory bowel disease, kidney abscess, and biliary tract injury. Initially manifested by the presence of lumbago, this disease spreads easily, is persistent, and is often misdiagnosed.
Methods:
Review and synthesis of pertinent literature and guidelines pertaining to abdominal infection and retroperitoneal infection.
Results:
Recent data indicate that mortality rates associated with retroperitoneal infection have been increasing annually. Early diagnosis and treatment have been shown to improve the prognosis. In the early stage, infection is insidious and lacks typical symptoms, and is primarily diagnosed with computed tomography (CT). Strategies that control the source of infection, rational use of antibiotic agents, and nutritional interventions are the primary approaches to treat the infections. Emergence of minimally invasive drainage technologies, including the ultrasound/CT-guided puncture and drainage, percutaneous nephroscope puncture and drainage, and drainage using a catheter through an abdominal puncture device (trocar) have shortened the treatment cycle and disease burden. However, current diagnosis and treatment for retroperitoneal infection are not sufficiently effective because some patients do not show typical clinical manifestations. Moreover, sensitivity and specificity of available auxiliary examination methods are not supported by sufficient evidence-based medical research. Additionally, there are no uniform standards on the timing of surgical intervention and treatment options. Therefore, we summarized the progresses on current diagnosis and treatment approaches for retroperitoneal infection.
Retroperitoneal infection is a secondary infection caused by inflammation, injury, or perforation of organs adjacent to the retroperitoneum. It spreads easily, is persistent, and is often misdiagnosed. Early diagnosis and active treatment considerably improve its prognosis. Because of the loose space and poor blood flow in the retroperitoneal tissues, an infection often spreads easily in the space to form abscesses early on [1]. Because of a lack of typical physical signs, misdiagnosis is common. Evidence indicates that mortality rates associated with retroperitoneal infections remain high despite appropriate interventions. The primary causes of death include multiple organ failure, gastrointestinal bleeding, and abdominal bleeding [2,3]. Recent innovations have improved the diagnosis and treatment of retroperitoneal infection. Notably, the emergence of minimally invasive drainage technology has provided new avenues of treating patients with these infections [4–6]. In this article, we review the diagnosis and treatment of retroperitoneal infection to provide recommendations for effective clinical treatment.
Epidemiology
Epidemiologic data are limited because of the low incidence of retroperitoneal infections. Generally, retroperitoneal infection caused by acute pancreatitis is common, and the mortality rate of severe necrotizing pancreatitis coinfection ranges between 30% and 39%. In contrast, retroperitoneal infections caused by appendicitis and bacteremia are relatively rare [7]. Multiple risk factors of the retroperitoneal infection are shown in Table 1. Among them, diabetes is the most common. The incidence of retroperitoneal infections has been increasing in the past two decades. This may be attributed to the advancements in diagnostic methods, the growing aging population, unhealthy diet and lifestyle, high incidence of diabetes, and the abuse of immunosuppressants and hormones.
Risk Factors for Retroperitoneal Infection
HIV = human immunodeficiency virus.
Before the discovery of antibiotic agents, gram-positive cocci accounted for approximately 80% of retroperitoneal infections [3]. Curently, with the widespread use of antibiotic agents, the pathogen of infection varies in different situations. Apart from Escherichia coli being the primary cause, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Proteus mirabilis, Clostridium perfringens, and Streptococcus are common causal pathogens of retroperitoneal infections. Anaerobic pathogens, including Mycobacterium tuberculosis, Brucella, actinomycetes, and Entamoeba histolytica also cause retroperitoneal infections.
Etiology
The presentations of bacterial infection in the extraperitoneal space are mild and infections easily spread along the space, often causing limitations to the disease diagnosis. It is therefore important to explore the etiology of retroperitoneal infection. Multiple diseases can cause infections, such as digestive and urinary system-related diseases, spinal osteomyelitis, necrotizing soft tissue infection, surgery, and trauma (Fig. 1).
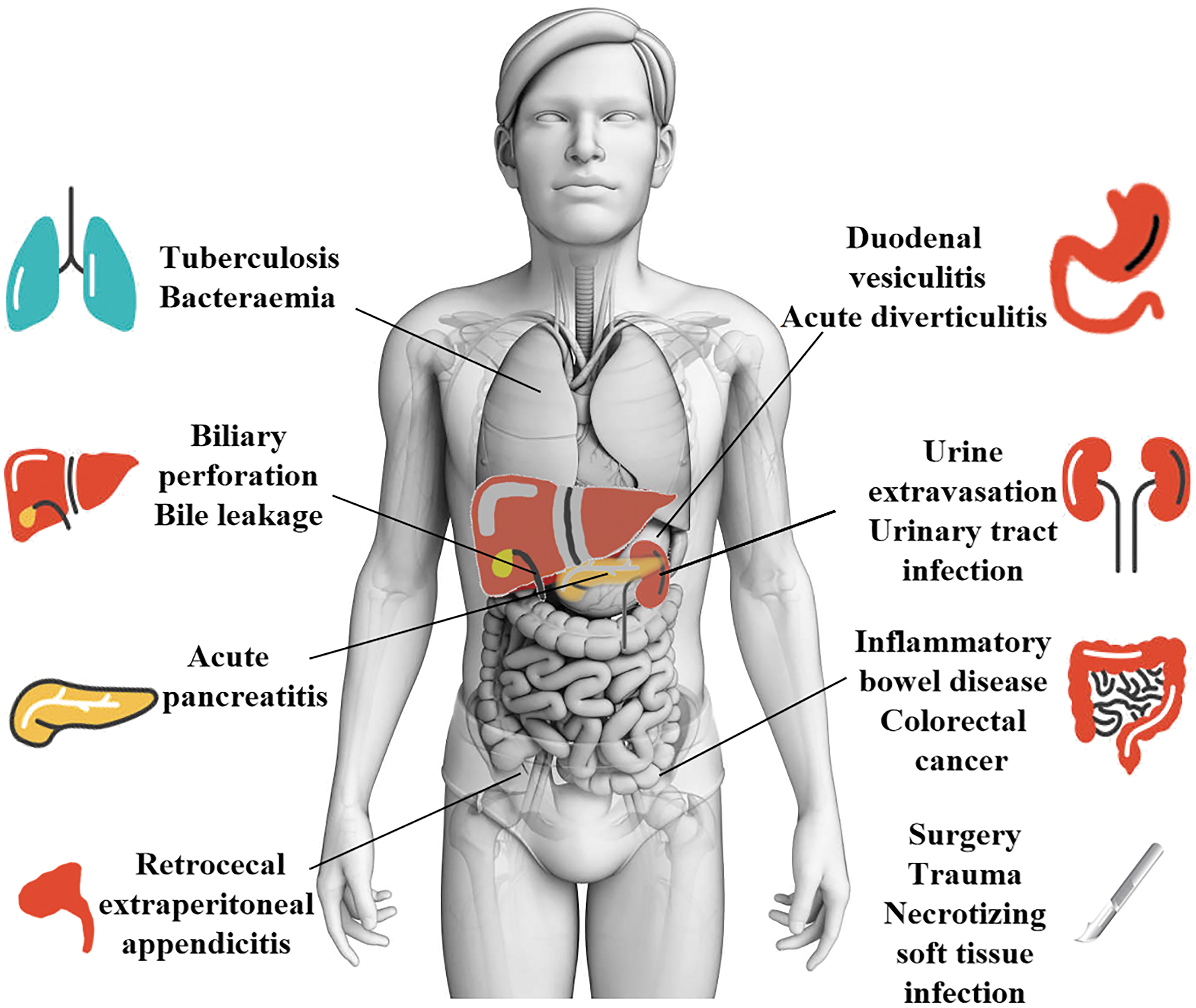
Etiology of retroperitoneal infection.
Retroperitoneal perforations of the gastrointestinal tract
Retroperitoneal perforation of the gastrointestinal (GI) tract, involving the ascending and descending colon, rectum, and duodenum often causes retroperitoneal infection given the special anatomic relation of the GI tract with the extraperitoneal space. Perforation is a serious complication of colorectal cancer (CRC), accounting for nearly 20% of all emergencies related to CRC [8]. Once tumors invade the plasma muscle layer, the intestinal wall becomes susceptible to necrosis and perforation. After the perforation, feces and bacteria diffuse into the retroperitoneal space via loose connective tissue of the peritoneum and the psoas space, forming retroperitoneal infection.
Acute colonic diverticulitis, often affecting the sigmoid or descending colon, is a common gastrointestinal disease in developed countries, especially in the United States and Europe [9]. According to a guideline from American Gastroenterological Association (AGA), approximately 15% of patients will develop serious complications such as abscess, perforation, and fistula, all of which contribute to retroperitoneal infections [10]. The duodenum is the second most common location for intestinal diverticula, and the morbidity of complicated duodenal diverticulitis was estimated at 0.03% per year. Retroperitoneal perforation, which is the most dangerous complication, causes retroperitoneal abscess [11,12].
Chronic inflammatory bowel disease (IBD), including Crohn disease and ulcerative colitis, is a chronic condition of the gastrointestinal tract resulting from abnormal mucosal immune responses, with an increasing incidence and prevalence worldwide [13]. Crohn disease is characterized by transmural inflammation and discontinuous skip lesions, in which the lesion usually involves the entire intestinal wall, causing ulcer and perforation. Nearly 5% of patients with severe ulcerative colitis may develop toxic megacolon, accompanied by acute colonic dilatation and acute perforation. Unlike intraperitoneal GI perforation, retroperitoneal perforation exhibits atypical clinical signs and symptoms, making it difficult to diagnose. Patients may present with severe abdominal pain, lumbago, fever, and positive psoas muscle irritation test. It has poor prognosis and high risk of death.
Additionally, retrocecal extraperitoneal appendicitis can cause peri-appendiceal abscess in cases of delayed diagnosis and treatment, and can further develop into retroperitoneal infection, manifested by lateral abdominal pain or low back pain, without typical metastatic right lower abdominal pain. The findings on physical examination include deep tenderness at the McBurney point, but only mild tenderness in the anterior peritoneal wall.
Severe acute pancreatitis
Severe acute pancreatitis (SAP) is a serious systemic disorder caused by pancreatic autodigestion that is characterized by sudden onset, rapid progression, and difficulties in treatment, with frequent multi-organ failures (MODs) [14]. In patients with severe acute pancreatitis, pancreatic necrosis and secondary infection of surrounding tissues can easily invade the entire retroperitoneal space from the root of the mesentery. In addition to abdominal pain and digestive symptoms, patients with SAP display peritoneal irritation symptoms, bloody ascites, Cullen signs, and Grey-Turner signs. According to the World Society of Emergency Surgery (WSES) in the 2019 guidelines on the management of SAP, interventions for necrotizing pancreatitis should start when the necrosis has become walled-off, usually four weeks after the onset of the disease. A step-up approach with percutaneous or endoscopic drainage should be implemented when the situation deteriorates [15].
Biliary tract perforation and injury
The lower two-third segment below the common bile duct is located in the retroperitoneal space. The impacted gallstone compresses the wall of the common bile duct, resulting in necrosis and perforation. It may also damage the common bile duct during cholecystectomy and common bile duct exploration for calculus extraction, both of which increase the risk of bile exudation and cause bilious retroperitoneal infection. Moreover, spontaneous perforation of the common bile duct, a rare disease in children and even rarer in adults, may cause retroperitoneal infection when the biliary leakage extends into the retroperitoneum [16]. Clinical manifestations of biliary tract perforation and injury include abdominal distension, right upper abdominal pain, chills and fever, right back edema accompanied with pain, and jaundice. For patients with suspected post-operative distal common bile duct injury, B-mode ultrasound or CT examination can be performed to detect the effusion around the duodenum and pancreatic head, and contrast agent can be injected through a T-tube to determine whether it flows into the retroperitoneum.
Urinary system-related diseases
Given that kidneys and ureters are extraperitoneal organs, retroperitoneal infections are secondary to urinary tract infection and urine extravasation. Hematogenous infection, pyelonephritis, or retrograde infection from ureteral obstruction may cause intra-renal abscess. Common causes for perinephric abscess are parenchymal disruption after fulminating pyelonephritis, hematogenous dissemination of furuncles, and renal abscess [17]. The abscess involves fibrous capsule and renal fascia, spreading to the extraperitoneal space and even the psoas major, causing widespread retroperitoneal infection. Clinically, kidney abscess manifests high fever, waist and back acute pain, abdominal mass, percussion pain in renal region, urine leukocytosis, and growth of pathogens in urine culture. The onset of perinephric abscess is more insidious and patients may simply present with anemia and discomfort. Physical symptoms may include flank tenderness, localized fullness, and scoliosis. Moreover, urine extravasation caused by renal and ureteral trauma can also develop into retroperitoneal infection. Computed tomography examination can clearly show the relation between the kidney, the perirenal space, and its adjacent structures and a test of puncture fluid can also be used for diagnosis.
Spinal osteomyelitis
Spinal osteomyelitis (referred as vertebral osteomyelitis or spondylodiskitis) is a rare spinal infectious disease, and the incidence of admission was 2.2 to 7.4 per 100,000 [18,19]. Spinal osteomyelitis can develop into a paraspinal abscess, spreading to the retroperitoneum and causing retroperitoneal infection. Patients with infection are characterized by back pain, fever, or neurologic symptoms without specificity. Physical signs include localized tenderness or spasm of the paraspinal muscles, pain with hip extension, and loss of lumbar lordosis [20].
Necrotizing soft tissue infection
Necrotizing soft tissue infection (NSTI), characterized by extensive necrosis of the skin and subcutaneous tissue, is caused by severe bacterial infection, with high morbidity and mortality [21]. It is difficult to implement early diagnosis and the disease progresses rapidly. Perineal, buttock, or groin necrotizing fasciitis can spread further through the pelvis to the retroperitoneum followed by retroperitoneal infection. Typical manifestations of necrotizing fasciitis include: soft tissue edema (75%), erythema (72%), intense pain (72%), tenderness (68%), fever (60%), and bullous or necrotic skin (38%) [22]. Once NSTIs are suspected or confirmed, thorough debridement and adequate drainage are required. When the infection involves the retroperitoneum, patients can benefit from a diverting colostomy to reduce the risk of secondary wound contamination triggered by enteric bacteria [23].
Surgery and trauma
Retroperitoneal infections caused by surgery and trauma are relatively frequent. In China, the rate of organ/space infection during abdominal surgery is approximately 1.5%, which is even higher in emergency surgery [24,25]. Surgery and trauma of the retroperitoneal and intraperitoneal organs are more likely to lead to retroperitoneal infection. In recent years, retroperitoneal infections caused by the abdominal war wound and trauma, surgical complications, and lumbar puncture have been reported, increasing the incidence of iatrogenic injury or trauma annually [26–28]. Medical procedure-related retroperitoneal infections are mainly caused by surgeries of the duodenal fistula, common bile duct injury, severe pancreatitis, appendix, sigmoid colon, and the rectum.
Other causes of retroperitoneal infections
Tuberculosis has been shown to cause retroperitoneal infections under certain conditions, such as the spread of cold abscess caused by spinal tuberculosis to the retroperitoneal space, intestinal tuberculosis-induced perforation, and abscesses behind the peritoneum, as well as renal abscesses secondary to renal tuberculosis. Infections caused by bacteremia after retroperitoneal colonization have also been reported [28–30]. With the gradual improvement in anti-tuberculosis treatment and the wide use of antibiotic agents, retroperitoneal infections resulting from the above causes have become clinically infrequent.
Diagnosis
Typically, presentation of retroperitoneal infection includes lumbago, fever, chills, weight loss, subcutaneous edema, abdominal distension, diarrhea, vomiting, and positive psoas muscle irritation test. In the early stage, severe systemic toxic symptoms such as high fever, chills, and general weakness could be perceived, with lumbago being the main local symptom. Laboratory tests show increased inflammatory markers at this stage. As disease progresses, pre-sacral pain, localized fullness, and tenderness of the costal spinal angle and waist, positive stimulation signs of psoas major muscle and iliopsoas muscle, and hypostatic edema could develop. Thereafter, severe infection leads to weight loss, malnutrition, and water–electrolyte disorders. Even with effective treatment, the mortality rate remains high.
As a supplementary means in the diagnosis, radiographs have certain additional indications with associated cost-effectiveness and low radiation. Retroperitoneal infections captured on abdominal plain films often present a shadow of affected area, fluid level, renal shadow, blurring of psoas margin, and scoliosis. Additionally, chest radiographs show elevated diaphragms, decreased respiratory mobility, and pleural effusions.
Ultrasound is the first choice in the examination of retroperitoneal infection. The ultrasound depicts the local soft-tissue edema, indicates the formation of the abscess by showing a fixed hypoechoic area, and measures the size of abscess as well as helps in determining the location of the abscess. A recent study reported that the sensitivity of ultrasound is 83.1% [31].
Moreover, an abdominal CT constitutes the gold standard in the diagnosis and detection of retroperitoneal infections [3]. The CT scan provides an accurate location of the infection and shows the relation between lesions and surrounding organs. Specifically, the infected area presents a low-density shadow, with fascia thickening, muscle edema, fatty stripes, hydrops, abscess, or even free gas all around. Additionally, a CT scan combined with magnetic resonance imaging (MRI) is effective for the diagnosis and localization of retroperitoneal abscesses, with a sensitivity up to 100% [32,33]. This tool thereby plays crucial roles in the diagnosis of multiple abscesses, the selection of re-operation approaches, and the determination of surgical scope. In addition, alaparoscopy or exploratory laparotomy is applicable if the primary lesion is not diagnosed clearly.
At present, relevant guidelines and consensus on the diagnostic criteria of retroperitoneal infections in clinical practice are lacking. The occurrence of the infection could be dangerous. However, because the onset is always hidden, the chances of missed diagnosis or misdiagnosis remain high. This necessitates the establishment of a diagnostic standard to guide the clinical diagnosis and treatment. By combining the guidelines for abdominal infection and retroperitoneal infection-related cases, we herein provide a simplified recommendation (Table 2).
Recommended Diagnostic Criteria for Retroperitoneal Infection
Patients with any three criterions of the above should be considered to be suspected, and if including 6, the diagnosis can be made.
Treatment
The treatment of retroperitoneal infections consists of the control of infection source, use of antibiotic agents, and nutritional support. Timely and effective control of the source of infection is the most crucial, aiming to remove the infected suppurative and necrotic tissue. Moreover, this form of treatment prevents the recurrence of the infection through adequate drainage. Additional drug therapy also plays vital role in the treatment of retroperitoneal infections.
Control of the source of infection
Measures to constrain the source of infection are divided into percutaneous puncture drainage and invasive surgery with drainage based on the surgical options. In recent years, with the emerging concept of minimally invasive surgery (MIS), most of guidelines on the control of celiac infection have recommended percutaneous puncture drainage with minimal physiologic damage for etiologic treatment [34–37]. To achieve maximum benefit for the patient with the least trauma, the puncture drainage method has been greatly improved, including ultrasound/CT-guided puncture drainage, percutaneous nephroscope puncture drainage, and drainage with a catheter through abdominal puncture device (trocar).
Puncture drainage
Retroperitoneal infections tend to form abscesses at early stage. For most infected patients, percutaneous puncture and drainage is the preferred treatment [38]. Recently, with the continuous advancement in imaging and interventional technology, the puncture and drainage guided by B-mode ultrasound/CT has been improved constantly, and the indications have been gradually increased. B-mode ultrasound-guided puncture is simple and easy to perform at the bedside. In comparison, CT-guided puncture is safer, more accurate, and the angle and direction of puncture is pre-designed in advance. Combining B-mode ultrasound with CT facilitates locating the optimal puncture site and at the same time reduces the incidence of complications. B-mode ultrasound/CT-guided puncture is suitable for isolated abscesses, such as peri-appendiceal abscesses. However, the clinical application of percutaneous puncture drainage has several challenges. For instance, the thick pus or necrotic tissue can easily cause blockage in the narrow pigtail tube, resulting in compromised drainage.
Nephroscopic puncture and drainage, first applied in the treatment of urinary system-related infections, has also been applied to other infections caused by retroperitoneal infections, such as acute necrotizing pancreatitis and iatrogenic bile duct perforation. The necrotic tissue is cleared under direct visualization and with the large operation space indwelling double cannulas are placed for continuous rinsing negative pressure drainage, which shortens the hospital stay substantially. Regarding the infection caused by necrotizing pancreatitis, percutaneous nephroscopic puncture and drainage is generally recommended to reduce incidences of bleeding and gastrointestinal fistula at three to four weeks after disease onset, when the peri-pancreatic infected tissue has formed an abscess [39]. For intra-renal or peri-renal abscesses larger than 3 cm in diameter, however, drainage should be performed as soon as possible to prevent the aggravation of infection if the patient's condition allows [40].
Based on the specific purpose, drainage with a catheter through the abdominal puncture device could be performed with trocars in different internal diameters. It has more extensive indications, more accurate direct visualization for positioning, and better effects for hidden location. Moreover, double cannulas are also placed indwelling to flush the infected site and improve the success rate of treatment. Drainage with trocars is suitable for single and large infective focus such as acute necrotizing pancreatitis and abscess secondary to colorectal perforation, with more accurate direct visual positioning and better drainage effect for hidden location. The patients undergoing catheterization should be re-examined using CT scan to re-evaluate the position of the abdominal infection focus and drainage tube and adjust the tube to the optimal drainage position if necessary. Moreover, CT scan re-examinations are recommended at any time when the condition changes. Because of the unique anatomic structure of the retroperitoneal space, patients are prone to develop multilocular abscesses and need a variety of percutaneous drainage approaches for sufficient drainage.
Invasive surgery
Invasive surgery should be considered when percutaneous drainage alone is unable to control the infection adequately, the spread of infection is too large, or the source of infection is uncertain. There are various surgical methods to control the source of infection, including subcostal and post-waist combining approach of necrosectomy, rib removal, and open drainage of retroperitoneal abscesses and retroperitoneal approach through small incision. Moreover, endoscopic techniques are also widely performed, such as video-assisted retroperitoneal debridement, single-port laparoscopic retroperitoneal debridement and drainage. Severe retroperitoneal infection is often accompanied with abnormal coagulation function. Therefore, on the premise of infection control, principles of injury control should be followed during the laparotomy. The necrotic tissue should not be forcibly stripped to avoid severe bleeding and tissue damage, if not separated from normal tissue. For patients with peritoneal space syndrome, the open abdomen in purpose of debridement and drainage could be applied to improve the perfusion of abdominal viscera [34,41].
Failure in the treatment of retroperitoneal infection is primarily attributed to failure in the control of infection sources. Treatment is considered unsuccessful when progressive dysfunction of organs occurs within one to two days after the infection control; when dysfunctions of the organs do not improve for two days or longer after infection control; and when the inflammation is not considerably alleviated within five to seven days [36]. Inflammatory manifestations are mainly reflected by temperature, leukocyte, procalcitonin, interleukin-6, and CT. If the above tests show no improvement, whereas the imaging findings indicate a remission, other sources of infection should be considered. Additionally, if there is no improvement or deterioration of the patient's condition in two to three days after surgical intervention, the guidelines for abdominal infection in China recommend the use of laparotomy [34]. For patients for whom treatment has with failed, the source of infection should still be controlled with minimal trauma as soon as possible.
Drug treatment
In the early stage of infection, antibacterial drugs are empirically used, based on etiologic analysis and the epidemiologic characteristics of the local pathogens (Table 3). China's guidelines for celiac infection suggest that for mild retroperitoneal infection, moxifloxacin, cefoperazone-sulbactam, or ertapenem can be used alone. However, for critically ill patients, carbapenems such as imipenem-cilastatin and meropenem or broad-spectrum antibiotic agents such as piperacillin-tazobactam are prescribed to cover all possible pathogenic bacteria and to control the infection immediately [34]. When the results of pus/blood culture and drug sensitivity are clear, the broad-spectrum antibiotic agent is adjusted in the de-escalation therapy. Nutritional support should be given as early as possible for malnourished patients [42].
Common Pathogens of Various Causes of Retroperitoneal Infections
Currently, there are inadequate guidelines related to the diagnosis and therapy of retroperitoneal infection. In clinical practice, optimal treatment for retroperitoneal infection could be missed because of the delay and improper diagnosis and treatment, thus aggravating the burden to the patients and even leading to failure of treatment. Therefore, combining relevant guidelines, case reports of retroperitoneal infection, and relevant studies, we summarized the normative diagnosis and treatment recommendations as a reference (Fig. 2).
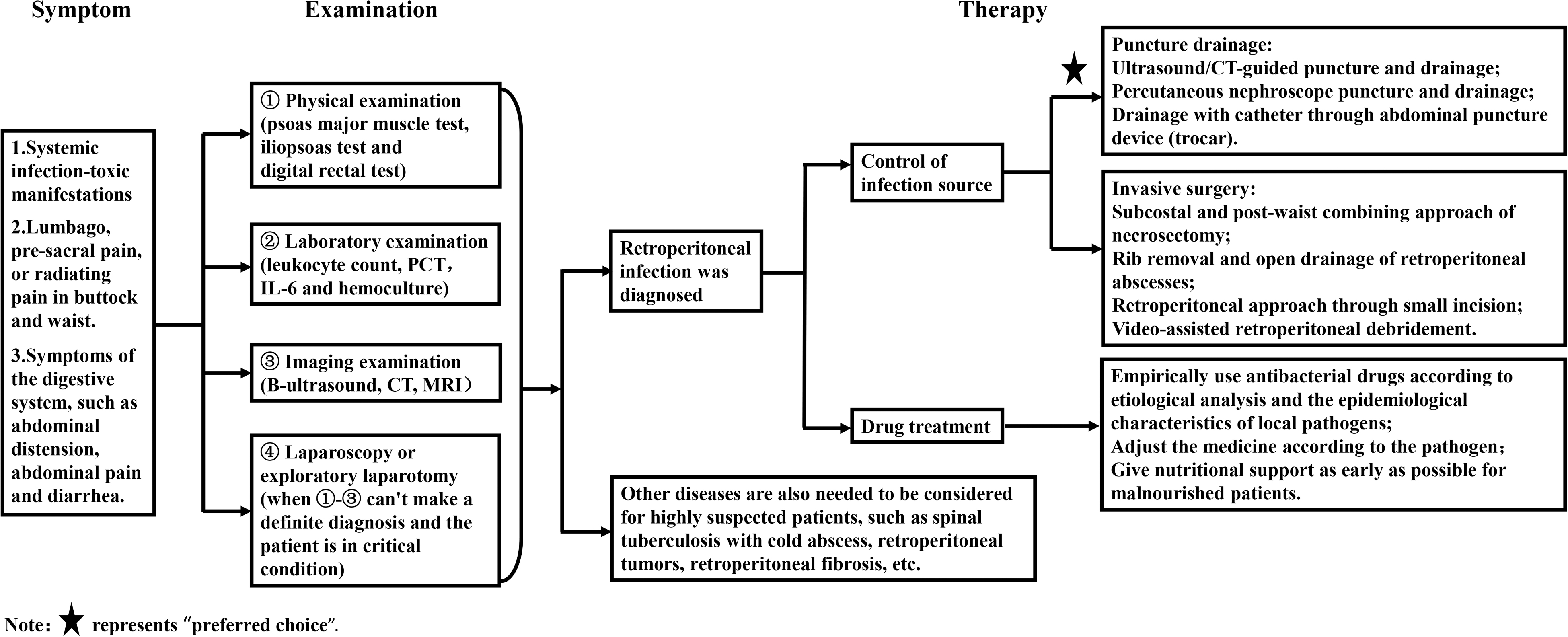
Diagnosis and treatment of retroperitoneal infection.
Conclusions
Retroperitoneal infection is a persistent and widespread intractable infectious disease with increasing morbidity. The disease has an insidious onset, with no evident signs of peritoneal irritation in the early stages. Main symptoms of retroperitoneal infection are lumbar and back discomfort and infection-toxic symptoms. It is mainly diagnosed with imaging tools such as abdominal CT. Early diagnosis improves the disease prognosis substantially. Active control of the origin of infection and judicious use of antibiotic agents are the primary treatment methods. However, challenges remain in the disease diagnosis and treatment of retroperitoneal infection. For example, the sensitivity and specificity of CT need to be confirmed further because of cases of misdiagnosis and missed diagnosis. The conventional diagnosis methods should be improved. The persistent nature of retroperitoneal infections increases burdens to the patients and medical institutions. However, there is currently no standardized timing for surgical intervention or treatment choices. Given the complexity of retroperitoneal infection in terms of affected organs, joint efforts are required from multidisciplinary physicians to treat the infection effectively. Collectively, models for effective multidisciplinary treatment should be developed, consistent with the concept of MIS.
Footnotes
Authors' Contributions
Peige Wang and Jianan Ren designed the review. Ze Li and Yinbing Tang both reviewed the paper. Peige Wang and Jianan Ren criticized the original paper. All authors read and approved the final manuscript.
Funding Information
This study was funded by Taishan Scholar Foundation of Shandong Province (Grant no.2018092901).
Author Disclosure Statement
The authors declare that they have no competing interests.