
Abstract
Background:
Dysregulation of the inflammatory and immune response to injury may increase susceptibility to secondary infections after trauma. It is unknown whether cytokines involved in this response could function as plasma biomarkers for surgical site infection (SSI). We hypothesized that the early cytokine response differs between patients who develop SSI and those who do not and that critical cytokine threshold values could be used to predict risk of SSI.
Patients and Methods:
Using the Glue Grant database, we performed an analysis of severely injured blunt trauma patients who underwent a major procedure and had available cytokine data. Patients were divided into SSI and no SSI groups. Receiver operating curve analysis was used to determine acceptable early cytokine predictors of SSI and critical threshold values. Multivariable regression analysis was then performed to determine the odds of developing SSI using threshold values, adjusting for key patient or injury factors. Cytokine levels were compared between SSI and no SSI groups at three time points.
Results:
The study cohort consisted of 70 patients and 11 patients developed SSI. Monocyte chemoattractant protein-1 (MCP-1) was the only acceptable early predictor of SSI with an area under the curve (AUC) of 0.71 (p = 0.03) and a critical threshold value of 490 pg/mL. Monocyte chemoattractant protein-1 levels above this threshold within 24 hours of injury were associated with SSI (adjusted odds ratio [AOR] 8.1; p = 0.01). Monocyte chemoattractant protein-1 levels within 24 hours of injury were higher in those who developed SSI (994 vs. 259 pg/mL; p < 0.01) and remained higher in the SSI group at 33 hours from injury (338 vs. 144 pg/mL; p = 0.01), but were similar by 106 hours (155 vs. 97 pg/mL; p = 0.19).
Conclusion:
Among cytokines involved in the early response to trauma, only early elevation of MCP-1 predicted SSI after blunt trauma. Monocyte chemoattractant protein-1 may act as a specific and early marker for SSI after blunt trauma, allowing for preventative measures to mitigate risks.
Surgical site infections (SSIs) account for 20% of all hospital acquired infections, making them the most common and costly of all health-care–associated infections [1–4]. Patients with SSIs face up to 11 times the risk of mortality compared with those without SSI and have longer post-operative hospital stays [1]. The resultant morbidity and mortality from SSIs cost the U.S. healthcare system $3.5 to $10 billion annually [1]. Patients with traumatic injuries are at especially high risk for SSIs with an incidence of up to 20% [1,2].
Traumatic injury leads to a genomic storm with simultaneous expression of genes involved in the systemic inflammatory, innate immunity, and compensatory anti-inflammatory responses and suppression of genes involved with adaptive immunity [5]. Although the complexities of this response have not been elucidated fully, dysregulation of this response is thought to increase susceptibility to secondary infections after severe trauma [6]. The key cytokines involved in the early response to severe injury have previously been identified [7,8]. However, it is unknown whether the cytokines involved in this early cytokine response could function as plasma biomarkers for SSI.
Therefore, the purpose of this study was to determine whether cytokines involved in the early inflammatory response to trauma could function as plasma biomarkers for SSI risk. We hypothesized that the early cytokine response would differ between patients who went on to develop SSI and those who did not and that critical cytokine threshold values could be used to predict risk of SSI.
Patients and Methods
We performed a retrospective analysis of the Inflammation and the Host Response to Injury (Glue Grant) database, a large-scale collaborative trauma relational database originally funded by the National Institute of General Medical Sciences (NIGMS). The database is available online and includes clinical, laboratory, and outcomes data for severely injured blunt trauma patients from multiple level 1 trauma centers in the United States from 2003 to 2011 [9]. All data within the database are de-identified. Data collection was approved by the regional Institutional Review Boards of all participating centers.
Enrollment criteria for injured patients in the database included: a blunt mechanism of injury, an abbreviated injury scale (AIS) severity score ≤2 in any body region excluding the head, emergency department (ED) arrival less than six hours from the time of injury, base deficit greater than or equal to 6 mEq or systolic blood pressure <90 mm Hg within 60 minutes of arrival to the trauma center, and red blood cell transfusion within 12 hours of injury. Trauma victims were excluded if they were younger than 16 or older than 90, had a spinal cord injury, isolated brain trauma, or thermal burns >20% of total body surface area. For our specific analysis, only patients with cytokine data were included and patients were excluded if they did not undergo a major procedure. They were then divided into two groups: patients with SSI and patients without SSI.
Patient data reviewed included demographics, injury severity score (ISS), total crystalloids within 12 hours of injury, red blood cell volume transfused within 12 hours of injury, weight, ED vitals, ED Glasgow Coma Scale (GCS), injury mechanism, hospital length of stay (LOS), intensive care unit LOS, ventilator days, and death. Surgical site infection details included days from injury to diagnosis, location in body, type, and specific causative organism. The database used the U.S. Centers for Disease Control and Prevention definitions for SSI type. According to these definitions, a superficial incisional SSI involves only the skin or subcutaneous tissue, a deep incisional SSI involves deeper tissues including the fascia or muscle layers, and an organ/space SSI involves any part of the body deeper than the fascial/muscle layers that is opened or manipulated during a procedure. Specifically, the Glue Grant database defines a surgical site as any site in which an incision has been made. Additionally, per the database protocol, if two types of SSI occurred together in the same region, on the same date, only the deepest infection was recorded.
Trauma-related cytokines that were evaluated included: interleukin (IL)-6, IL-8, IL-10, IP-10, monocyte chemoattractant protein-1 (MCP-1), and granulocyte colony-stimulating factor (G-CSF). Values from blood samples that had been collected within 24 hours of injury for each cytokine were evaluated for every patient. When more than one value was obtained within 24 hours, the earliest one was used. Missing values were assigned a value of 0.6 pg/dL per the database protocol. Cytokines that had more than two patients with missing values total were not included in the analysis. A receiver operating curve (ROC) analysis was performed to evaluate the ability of each cytokine to predict SSI. An area under the curve (AUC) of 0.70 or greater used to identify acceptable cytokine predictors [10]. Threshold values were determined by the highest associated Youden index, which is calculated by the equation: sensitivity + specificity −1 [11].
Next, a univariable analysis was performed to evaluate the association between early patient factors, and the outcome of SSI. If a variable was identified as significant in univariable analysis, using a p value <0.2, it was subsequently included in a multivariable regression model. Cytokines that had been identified as acceptable predictors on ROC analysis were included in the multivariable model using their previously identified cutoff values. Last, second and third values of key cytokines (outside of 24 hours) were reviewed to evaluate for sustained response over time in patients with SSI versus without SSI.
Baseline characteristics and outcomes data were analyzed using χ2 or Fisher exact tests for categorical variables and paired Student t-test continuous parametric data, respectively. Demographic values and cytokine values were reported as mean ± standard deviation or standard error of mean for graphs. An α value of <0.05 was identified for statistical significance. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 25 (IBM Corp, Armonk, NY).
Results
There were 78 patients with available cytokine data who sustained severe blunt trauma. After exclusion of patients without a major procedure, 70 patients remained in the study cohort. Within the study cohort, 11 patients developed an SSI, and 59 patients did not. More than 90% of patients in the study cohort (n = 64), underwent multiple major procedures. There was no difference in the percentage of patients who underwent multiple procedures between the SSI and no SSI groups (91% vs. 86%; p = 0.68). The mean time from injury to first procedure was 0.9 ± 1.8 days. The first procedure occurred outside of the first three days after injury in 6% of the entire cohort. Overall, the cohort was young (33.4 years), white (86%), and male (59%). Patients were severely injured with a mean overall ISS of 31.2 ± 14 and received a high volume of crystalloids within the first 12 hours (14.2 L ± 9). On arrival, patients were tachycardic with a mean heart rate of 116 ± 23 and had a reduced level of consciousness (GCS 9.7 ± 5). For patients who developed SSI and those who did not, the most common mechanism of injury was motor vehicle crash (MVC) with the patient as an occupant in the vehicle. Patients in both groups were similar in terms of demographics, severity of their injuries, volume of crystalloid resuscitation, volume of red blood cells transfused, ED vital signs, and arrival GCS. Mechanism of injury was also similar between patients who developed SSI and those without SSI. Patients with SSI had longer hospital lengths of stay, intensive care unit LOS, and ventilator days (Table 1).
Demographics and Injury Characteristics of Entire Cohort
SSI = surgical site infection; SD = standard deviation; ISS = injury severity score; RBC = red blood cells; ED = emergency department; SBP = systolic blood pressure; DBP = diastolic blood pressure; HR = heart rate; GCS = Glasgow Coma Scale.; MVC = motor vehicle crash; LOS = length of stay; ICU = intensive care unit.
Of the 11 patients who developed SSI, some had multiple SSIs, resulting in a total of 16 SSIs in the entire cohort. On average, SSIs were diagnosed 13.1 ± 7.6 days from injury. There were two patients with synchronous SSIs in the same location, but with different causative organisms. Two other patients had non-synchronous SSIs during their hospitalizations, one of whom had SSIs at two different surgical locations. The majority of all infections occurred in the abdomen or pelvis (56%). Most SSIs were either deep incisional (n = 7) or organ/space (n = 6). There were 10 infections with an identified causative organism, and of these, eight were gram negative (Table 2).
Surgical Site Infection Details
SSI = surgical site infection; SD = standard deviation; CoNS = coagulase-negative staphylococci; NOS = not otherwise specified.
On ROC analysis of the trauma-related cytokines, only MCP-1 was found to be an acceptable predictor of SSI with an AUC of 0.71, p = 0.03. None of the other cytokines evaluated (IL-6, IL-8, IL-10, G-CSF, IP-10) had an acceptable AUC above 0.70 (Table 3). The ROC curve for MCP-1 as a predictor of SSI is shown in Figure 1. The highest Youden index corresponded with an MCP-1 value of 490 pg/mL (sensitivity of 46%, specificity of 88%; Y = 0.34) and therefore, this value was selected as the critical threshold value.
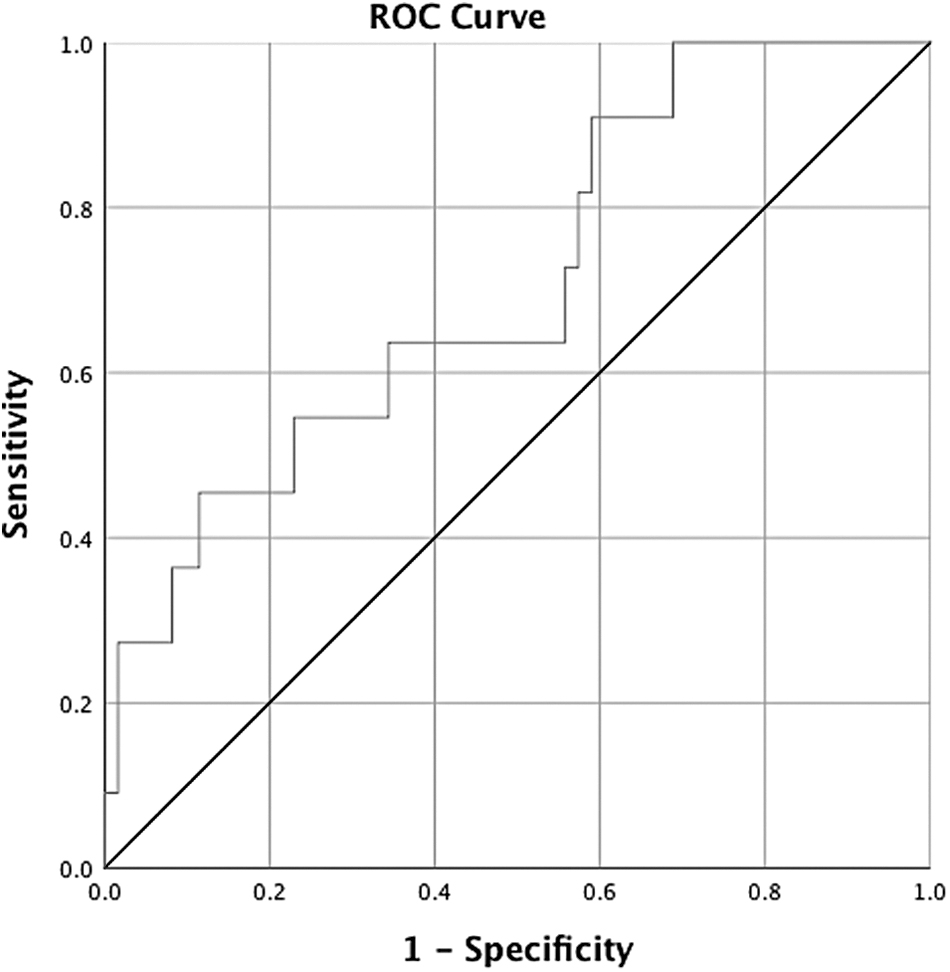
Receiver operating characteristic (ROC) curve for early monocyte chemoattractant protein 1 (MCP-1) elevation within 24 hours of injury as a predictor of surgical site infection.
Receiver Operating Characteristic Curve Analysis: Early Trauma-Related Cytokine Elevation as Predictor of SSI
Early cytokine elevation from within 24 hours from injury.
SSI = surgical site infection; AUC = area under the curve; SE = standard error; CI = confidence interval; MCP- 1 = monocyte chemoattractant protein 1; IL = interleukin; G-CSF = granulocyte colony-stimulating factor; IP = interferon-γ–induced protein.
To investigate which early patient factors were most associated with development of SSI, univariable regression analysis was performed to create a multivariable model. Diastolic blood pressure and a mechanism of MVC as a motorcyclist were associated with increased odds of an SSI. Adjusting for these two parameters on multivariable analysis, an MCP-1 level >490 pg/mL was associated with increased odds of SSI (adjusted odds ratio [AOR] 8.09; p = 0.01). Using that same cutoff value, patients with an MCP-1 level <490 pg/mL had reduced odds of developing SSI (AOR 0.12; p = 0.01). Diastolic blood pressure and mechanism of injury as a motorcyclist did not remain associated with SSI on multivariable analysis (Table 4).
Univariable and Multivariable Analysis Using MCP-1 Threshold Value as Predictor of SSI
MCP-1 = monocyte chemoattractant protein 1; SSI = surgical site infection; OR = odds ratio; CI = confidence interval; AOR = adjusted odds ratio; ISS = injury severity score; RBC = red blood cells; ED = emergency department; SBP = systolic blood pressure; DBP = diastolic blood pressure; HR = heart rate; GCS = Glasgow Coma Scale; MVC = motor vehicle collision.
The mean MCP-1 levels at three time points are shown for patients with SSI compared with those without SSI in Figure 2. The mean time of the first blood draw was 7.5 hours after injury for the SSI group and 8.5 hours for group without SSI, p = 0.35. The mean MCP-1 level for the SSI group within 24 hours of injury was higher than the mean of those who did not develop SSI (994 ± 612 pg/mL vs. 259 ± 28 pg/mL; p < 0.01). Monocyte chemoattractant protein 1 levels were also higher in the SSI group at the second time point that occurred on average 33 hours from injury and corresponded to the first blood draw outside of 24 hours (338 ± 139 pg/mL vs. 144 ± 21 pg/mL; p = 0.01). Monocyte chemoattractant protein 1 levels were similar between the groups at the third collection time point that occurred on average 106 hours or 4.4 days from injury (155 ± 57 pg/mL vs. 97 ± 16 pg/mL; p = 0.19). Because SSIs were diagnosed on average 13.1 days from injury, the time from normalization of MCP-1 to SSI was approximately 8.7 days.

Monocyte chemoattractant protein 1 (MCP-1) levels in patients with surgical site infection (SSI) versujs no SSI. Mean MCP-1 values with standard error of mean ranges from three blood sample collections in patients with SSI versus no SSI. The first value is from within 24 hours of injury and was higher in patients who went on to develop SSI versus those who did not, 994 pg/mL versus 259 pg/mL, respectively, p < 0.01. Monocyte chemoattractant protein-1 levels were also higher in the SSI group at the second time point (338 pg/mL vs. 144 pg/mL, p = 0.01). The second time point corresponds to the first blood draw outside of 24 hours from injury. There was no difference in MCP-1 levels between the groups at the third time point which occurred a mean of 106 hours from injury, respectively (155 pg/mL vs. 97 pg/mL, p = 0.19).
Discussion
Surgical site infections remain a common issue among the trauma patient population. The inflammatory and immune response after traumatic injury is complex and dysregulation may increase susceptibility to secondary infections [5,6]. It is unknown whether this initial systemic response to trauma might predispose patients specifically to development of SSI. Therefore, the purpose of this study was to determine whether cytokines involved in the early inflammatory response to trauma could function as plasma biomarkers for SSI risk. We hypothesized that the early cytokine response would differ between patients who went on to develop SSI and those who did not and that critical cytokine threshold values could be used to predict risk of SSI. Our results show that higher MCP-1 levels within 24 hours of injury are predictive of higher SSI risk. Although MCP-1 levels were higher within 24 hours after injury in patients who developed SSI compared with those who did not, after 24 hours, MCP-1 began to normalize and this difference did not extend past 33 hours from injury. Therefore, early elevation of systemic MCP-1 within 24 hours of severe blunt trauma may serve as an early biomarker of SSI risk.
In support of our findings, growing evidence suggests that genetic variations of MCP-1 polymorphisms influence susceptibility to infectious complications [12,13]. One study of Mexican and Korean patients found that carriers of the MCP-1 genotype GG produce much higher concentrations of MCP-1 and were more susceptible to pulmonary tuberculosis by more than five-fold compared with those with the genotype AA. Patients with a heterozygous genotype of AG experienced intermediate susceptibility and were more than two-fold more likely to develop tuberculous than those with the AA genotype [13].
Additionally, in patients with a history of spinal tuberculosis, MCP-1 levels were found to be elevated prior to development of a recurrence [14]. Our study adds to the current body of literature by demonstrating early elevation of MCP-1 in patients who later developed SSI, supporting MCP-1 as a predictive biomarker for infectious complications. Our findings also support MCP-1 as a unique predictor of SSIs by demonstrating a higher AUC for MCP-1 compared with other early inflammatory markers of trauma, including IL-6. Similarly, in a study of patients with sepsis, MCP-1 was found to be a superior predictor of 28-day mortality compared with IL-6, Acute Physiologic and Chronic Health Evaluation II score, and Sequential Organ Failure Assessment score [15]. Additionally, in a prospective cohort study of patients with severe sepsis that included multiplex analysis of 17 candidate cytokines in the serum, only MCP-1 was independently associated with increased mortality [16].
Several features of MCP-1 elevation may account for its association specifically with SSIs. In endotoxin-treated mice, MCP-1 upregulation was associated with decreased diaphragmatic force. Antibody neutralization of MCP-1 alleviated diaphragmatic weakness and reduced MCP-1 expression. MCP-1 treatment of non-septic muscles also led to contractile weakness [17]. This is relevant to our findings because impairment of respiratory muscle function after surgery may lead to post-operative complications including infections [18]. In our study, patients with SSI had nearly twice as many days on the ventilator compared with those without SSI even though injury pattern, injury severity, and volume of resuscitative fluids administered were similar between the groups. Another feature of MCP-1 that may account for association with SSI is related to hyperglycemia. Exposure of human skeletal muscle cells to MCP-1 at physiologic levels induced a state of increased insulin resistance, whereas exposure to IL-6 and IL-8 at physiologic levels did not [19]. Hyperglycemia is known to be associated with increased risks of SSI, and therefore, MCP-1 elevation may induce insulin resistance and subsequent hyperglycemia [20–22]. However, in our study, maximum glucose levels from within 24 hours of injury were not higher in patients who developed SSI (188 mg/dL vs. 190 mg/dL; p = 0.72) and glucose levels at time points beyond 24 hours were not available.
Although more is known about MCP-1 as a predictor of poor outcomes in the setting of sepsis, less is known about its association with outcomes after traumatic injury. However, one prospective observational study of severely injured trauma patients found higher levels of plasma MCP-1 in those who went on to develop sepsis [23]. In agreement with our findings, they found that MCP-1 levels from post-trauma day one differentiated the sepsis and non-sepsis groups, while the MCP-1 levels were similar between the two groups by day three. Interestingly, the mean day one MCP-1 level in the group with sepsis (1013 pg/mL) was above the threshold value from our study (490 pg/mL), whereas the mean MCP-1 in the non-sepsis group (325 pg/mL) fell below the threshold and both values were similar to mean MCP-1 levels from the SSI (994 pg/mL) and no SSI groups (259 pg/mL) in our study. Lastly, in their study, the AUC for MCP-1 as a predictor of sepsis was 0.82 compared with 0.63 for IL-6, supporting our findings of MCP-1 as a superior predictor of SSI compared with IL-6 based on AUC values.
If MCP-1 is involved in the development of infectious complications, it follows that its inhibition or deletion should reduce or prevent these complications. In a murine model of septic peritonitis and lipopolysaccharide-induced endotoxemia, MCP-1 blockade with bindarit, both prophylactically and therapeutically reduced MCP-1 levels and myeloperoxidase activity, an indicator of neutrophil recruitment. Treatment also protected mice from lung and liver damage histologically as evidenced by decreased thickening of alveolar and neutrophil infiltration [24]. The authors suggest anti-MCP-1 strategies may therefore have potential therapeutic value in the treatment of sepsis and endotoxemia. Other studies demonstrated that a genomic deletion of MCP-1 in mice contributed to resistance against major Leishmania infection, whereas excessive MCP-1 expression in transgenic mice predisposed them to infection with Listeria monocytogenes and Mycobacterium tuberculosis [25,26]. Together, these studies of MCP-1 blockade or deletion support the role of MCP-1 in infectious complications, although the exact underlying mechanism remains unclear.
This study has several limitations. The operative details regarding class of contamination for major procedures were not available and therefore, we could not control for this variable in our model. It is possible that patients with early elevation of MCP-1 had higher wound classes during their procedures, putting them at higher risk for SSI. Additionally, appropriate antibiotic administration surrounding the procedure was assumed. Next, our findings are limited by the relatively small number of SSIs and retrospective design of the study. Nonetheless, our finding of MCP-1 as a potential biomarker for the development of SSI is supported by multiple other studies implicating MCP-1 as a key mediator in the development of infectious complications.
Conclusions
The cytokines involved in the response to severe trauma are relatively well known. We sought to identify a biologic marker from this early systemic response that could predict SSI after trauma and identified MCP-1 as a potential biomarker with a critical threshold value of 490 pg/mL. Our findings add to the growing body of evidence that supports MCP-1 as a useful biomarker for infectious complications and may help with earlier identification of patients at risk for SSI, allowing for preventative measures to reduce risks.
Footnotes
Acknowledgments
The authors would like to thank the Inflammation and the Host Response investigators for providing the data for this study.
Funding Information
The Glue Grant database was supported by the Inflammation and the Host Response to Injury Large Scale Collaborative Research Program (Glue Grant U54 GM062119), awarded to Dr. Ronald G. Tompkins, Massachusetts General Hospital, by the National Institute of General Medical Sciences. Our work represents a secondary use of this public database. The conclusions and discussion are the authors' and do not necessarily represent the views of either the Glue Grant, Massachusetts General Hospital, or the National Institute of General Medical Sciences. The authors did not receive any funding.
Author Disclosure Statement
No competing financial interests exist.