
Abstract

To the Editor:
A
Authentic ICUs were charged with managing the sickest patients. Consequently, the surgical ICU was emptied to prepare for a rapid influx of COVID-19 patients. Within 24 hours, all 20 beds were occupied by patients with severe acute respiratory failure.
Our mission as surgical intensivists was manifold: To care for numerous critically ill patients while learning about the new and unique COVID-19 syndrome; to train colleagues with limited-to-no critical care experience to provide care to these patients; and to revise existing protocols and create new ones to standardize critical care across multiple temporary ICUs as they opened to receive patients, and to which we anticipated re-deployment.
Our task was confounded by the unstable, rapidly changing nature of these newly admitted patients; given their remarkably similar presentations, it could become difficult to keep track. Moreover, arterial blood gas determinations often exceeded 100 tests/day. This, combined with the need to follow a battery of other tests that were otherwise ordered infrequently (e.g., procalcitonin,
A visual tool, analogous to a dashboard, was created to facilitate rapid, accurate transmittal of crucial information, even to clinicians coming to the bedside for the first time. The glass doors of each cubicle were utilized as a dry-erase board, and a standardized display format was devised (Figs. 1, 2.). Information could be updated as received by any member of the care team as long as formatting was preserved. Substantive updates of the care plan were made on twice-daily formal rounds. Check boxes allowed tracking of progress toward fulfillment of each patient's daily plan. In addition to demographic data required for drug dosing and ventilator settings, the patients tier status [1], reflective of severity of critical illness, and “code” status were displayed prominently, as were daily and cumulative Sequential Organ Failure Assessment (SOFA) scores [2] used for both prognostication and triage (and resource allocation, had it become necessary).
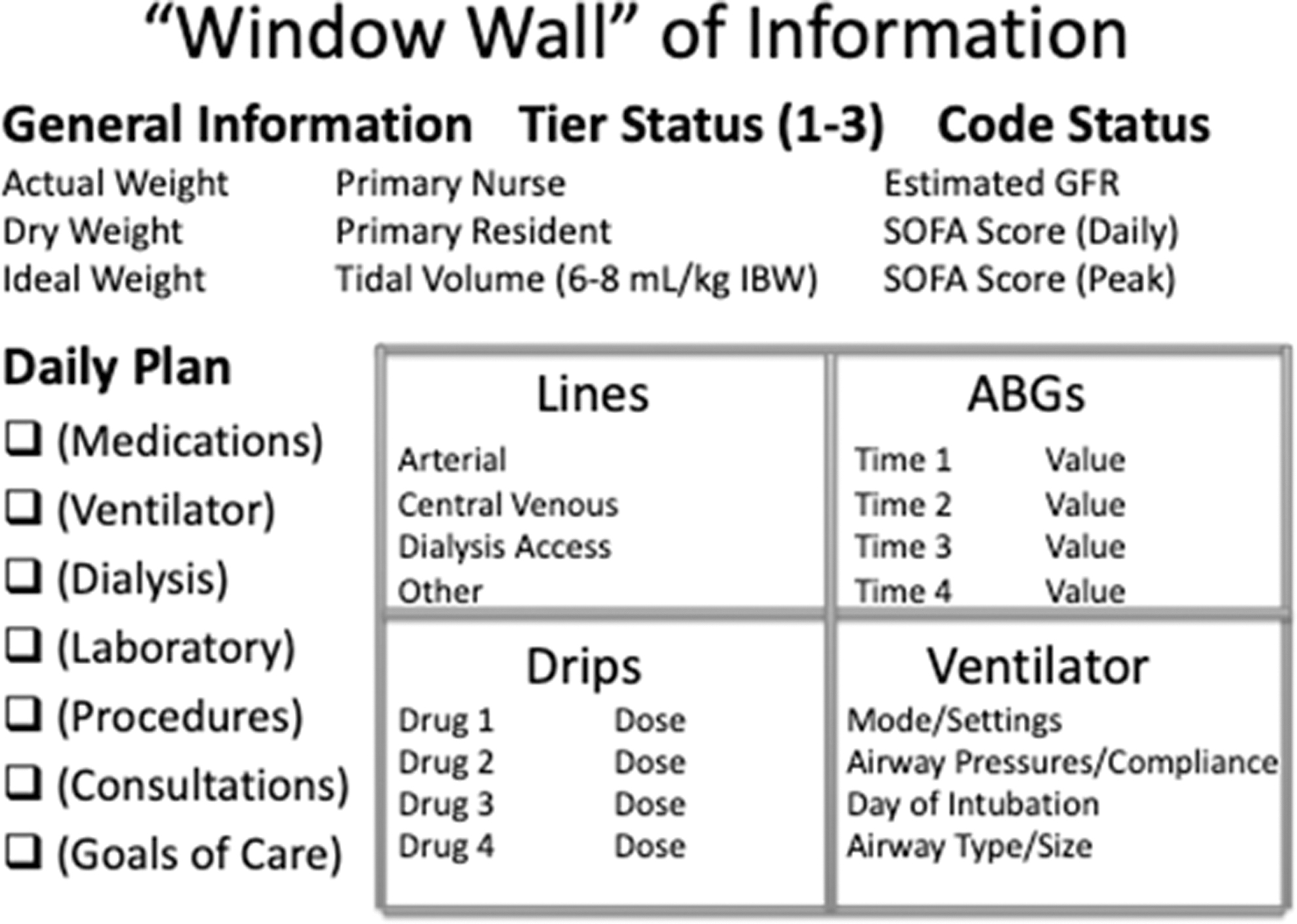
Cartoon depicting the formatting and content of the “window wall” of information. GFR, glomerular filtration rate; SOFA, sequential organ failure assessent; ABG, arterial blood gas.

Prototypical example of window wall of information. Image does not reflect actual patient data. IBW, ideal body weight; SOFA, sequential organ failure assessent; ABG, arterial blood gas.
The patient's primary nurse and physician were listed for identification and facilitation of order writing. Vascular access devices (and location) were noted. Dosages of parenteral vasoactive, analgesic, and sedative drugs that could potentially affect cardio-respiratory function and the neuromuscular blocking agent used (if necessary) were reported. Detailed mention was made of ventilator settings, lung mechanics, and gas exchange, derangements of which were usually the precipitant of ICU admission and the reason for protracted ICU care, and the focus of particularly dense data capture.
Owing to the nature of the crisis, the window wall was evaluated during patient care prospectively in the surgical ICU for 48 hours before adoption by all critical care areas hospital-wide. The system remains in place as the crisis in New York City enters its fifth week. Rounding time has decreased substantially, and handoffs have been facilitated greatly. Far fewer tasks are delayed or overlooked. Because of infection control measures including suspension of patient visitation, cessation of resupply of disposables to individual cubicles, and suspension of food delivery on trays, all persons entering critical care areas during the pandemic were deemed entitled to Protected Health Information (PHI) under the terms of the Health Insurance Portability and Accountability Act (HIPAA), permitting open display of PHI. The PHI was erased between patients before room cleaning by Environmental Services.