
Abstract
Background:
There currently is no standard practice for optimal urinary catheter removal after rectal resection (proctectomy). Delayed removal may increase urinary tract infection risk, an important hospital quality metric. This study aimed to assess the effect of catheter duration on urinary tract infection rate. We hypothesized that early removal would be associated with fewer infections.
Methods:
We performed a retrospective review of patients who underwent proctectomy from January 2007 to December 2017 with urinary catheter placement in our colorectal surgery department. The main outcome measures were urinary tract infection, post-operative urinary retention, and length of stay. Patients were divided into early (post-operative day one or two) and late (day three or later) removal groups.
Results:
A series of 2,429 patients were included; 1,176 in the early and 1,253 in the late group. The early group had a shorter median length of stay (5.26 versus 7 days). The urinary tract infection (n = 77) multivariable logistic regression model showed no association between timing of removal and infection; however, females had more infections (odds ratio [OR] 2.70, 95% confidence interval [CI] 1.65–4.41). The post-operative urinary retention model (n = 280) showed no association between the timing of removal and retention; however, patients who underwent pre-operative radiation (OR 1.55; 95% CI 1.15–2.09) or total proctocolectomy (OR 1.74; 95% CI 1.21–2.49) or were male (OR 1.35; 95% CI 1.02–1.78) were more likely to have retention. When analyzed by specific removal day, each one-day delay in removal increased the odds of infection by 21% (OR 1.21; 95% CI 1.09–1.35] and decreased the odds of retention by 12% (OR 0.88; 95% CI 0.80–0.97] with a cross-over at 9 days. Patients who experienced retention were not more likely to have infection.
Conclusion:
Early urinary catheter removal after proctectomy was associated with a lower urinary tract infection rate and a shorter hospital stay.
The introduction of enhanced recovery protocols (ERPs) beginning in the 1990s has been applied in colorectal surgery [1–6]. An important component of ERP is early removal of indwelling urinary catheters (first developed by Dr. Frederic E.B. Foley in 1929), which secondarily facilitates and is synergistic with early ambulation and feeding [7]. It also likely decreases urinary tract infection (UTI) rates, which is the most common type of nosocomial infection in surgical patients (accounting for approximately 35% of all hospital-acquired infections), as the duration of indwelling catheters likely is the most important risk factor [8–13]. Catheter-associated UTI (CAUTI) are associated with longer hospital stays, higher re-operation rates, higher morbidity, and higher 30-day mortality rates in acute care settings, and the economic burden has been estimated at $676 to $12,000 per single UTI case and $340 to $450 million annually [8,10,11,14,15]. There are several studies confirming the inverse relation between the duration of urinary catheter use and UTI after surgery; however, the investigators emphasize the need to find a balance between decreasing UTI risk and increasing the post-operative urinary retention (POUR) risk [15,16].
Currently, there is no established optimal timing of urinary catheter removal after colorectal surgery [1,15]. The greatest risk associated with early removal is POUR, particularly after low rectal procedures; and it has been suggested that POUR requiring re-catheterization may be a cause of UTI [16]. However, few studies have examined the relation between early removal and the rate of POUR and of UTI from POUR [14,17–19].
This study aimed to evaluate urinary catheter removal practices after proctectomy and to assess the association of dwelling duration with the UTI rate and hospital length of stay (LOS). Our secondary aim was to assess the relation between POUR requiring straight or re-catheterization and subsequent UTI. We hypothesized that early catheter removal would be associated with improved short-term outcomes, including a decreased rate of UTI and shorter LOS. We secondarily hypothesized that POUR after urinary catheter removal requiring straight or re-catheterization would not be associated with an increased risk of UTI.
Patients and Methods
Patients who underwent proctectomy (abdominoperineal resection, total proctocolectomy, anterior proctosigmoidectomy) for any indication from January 2007 to December 2017 and had an indwelling urinary catheter post-operatively were identified retrospectively from an Institutional Review Board-approved, prospectively maintained outcomes database. Patient demographic variables collected were age at surgery, gender, body mass index, urologic history, and diabetes mellitus. Criteria for urologic history were a history of benign prostatic hyperplasia, nephrolithiasis, acute urinary retention, chronic kidney disease, or cancers of the kidney, bladder, or prostate. Patients were excluded if they experienced any urologic injury during their surgery (including fistula takedown/cystostomy/bladder repair or ureteral injury), developed prolonged critical illness, or had a hospital LOS >30 days.
Patient charts were reviewed for pre-operative radiation therapy, primary cancer site, diagnosis/indication for surgery, surgery date, surgical procedure, use of ureteral stents, surgical approach, operative time, American Society of Anesthesiologists (ASA) score, urinary catheter removal day, UTI occurrence, POUR occurrence, and LOS. We defined UTI as a positive urinalysis or positive urine culture requiring treatment with antibiotics up to one month after surgery, whereas POUR was defined as the need for straight or re-catheterization based on failure to void eight hours after urinary catheter removal or a bladder ultrasound scan showing >400 mL of urine in the bladder. No specialized team was used to insert urinary catheters. The primary endpoint was UTI, and secondary endpoints were POUR and LOS.
Patients were stratified into two groups: Early and late urinary catheter removal based on a study by Kwaan et al. [20], where the early group had removal on post-operative day (POD) one or two and the late group had removal on POD three or later; urinary catheter removal timing was up to the surgeon's discretion. The ERPs were put into practice in October 2016 in our colorectal surgery department, during the study period. Patients also were divided into low risk for POUR and UTI (no diabetes mellitus or urologic history) and high risk (diabetes mellitus or urologic history or both).
The data were analyzed with an intention-to-treat approach. All relevant patient characteristics and operative and post-operative data were presented as mean ± standard deviation, median [25th, 75th percentiles], or frequency (percent). The t-test or non-parametric Wilcoxon rank sum test was used for continuous factors, and the χ2 test or Fisher exact test was used to compare categorical variables between early and late groups as appropriate. Univariable analyses were conducted to identify factors associated with the occurrence of UTI and POUR. Multivariable logistic regression models were constructed to assess the association of urinary catheter duration (early versus late) with UTI and POUR. The number of independent variables in each model was determined following the 10 events per variable rule, and the models of that size with the highest score χ2 statistic are presented. The McNemar test was used to assess overall marginal homogeneity between the occurrence of UTI and POUR. Subgroup analyses were performed in high-risk and low-risk patient subgroups. All comparisons were made at a significance of 0.05, and all analyses were performed with R version 3.6.1.
Results
Patient characteristics
A total of 2,429 patients were included, of whom 54% were male. Overall, 1,176 (48%) were in the early urinary catheter removal group and 1,253 (52%) in the late removal group. The two groups differed significantly (p < 0.05) in several baseline characteristics (Tables 1 and 2). The early removal group had more females and fewer patients with diabetes mellitus, were less likely to have had laparoscopic surgery and ureteral stents, and had a shorter LOS than the late group.
Patient Demographics and Operative Characteristics by Urinary Catheter Duration
Statistics are presented as mean ± standard deviation, median [25th, 75th percentiles], or frequency (percent). Statistically significant findings are shown in
ASA = American Society of Anesthesiologists.
Intra-operative Characteristics by Urinary Catheter Duration
Statistics are presented as median [25th, 75th percentiles] or frequency (percent). Statistically significant findings are shown in
When stratified by risk of UTI and POUR status, there were 711 (29%) patients in the high-risk group and 1,717 (71%) in the low-risk group. These two groups differed significantly (p < 0.05) with respect to age (the high risk group was older, 57.5 versus 50.8 years), gender (male 63.6% vs. 50.1%), time of urinary catheter removal (median day three versus day two), and likelihood of POUR (14.5% versus 10.3%).
Urinary tract infection
The overall rate of UTI was 3.2% (n = 77). We observed a trend of decreasing UTI rate over the study period (p = 0.056). Univariable analysis showed that female gender and urologic history were significantly associated with the occurrence of UTI (Table 3). Multivariable logistic regression showed only female gender (OR 2.7; 95% CI 1.65–4.41) to be associated with UTI (Fig. 1). Adjusted analysis showed that in the low-risk group, female gender (OR 4.11; 95% CI 2.04–8.30) was associated with UTI. The early and late catheter removal groups did not differ significantly in UTI occurrence.

Characteristics associated with urinary tract infection (adjusted analysis; n = 2,426).
Characteristics Associated with Occurrence of Urinary Tract Infection (UTI) (Unadjusted Analysis)
Statistics presented as mean ± standard deviation, median [25th, 75th percentiles], or frequency (percent). Statistically significant findings are shown in
ASA = American Society of Anesthesiologists.
Post-operative urinary retention
The overall rate of POUR was 11.5% (n = 280). We observed an increase in the POUR rate over the study period (p < 0.001). Univariable analysis showed that male gender and urologic history were associated significantly with POUR (Table 4). Multivariable logistic regression analysis showed that pre-operative radiation therapy and total proctocolectomy also were associated with POUR (Figure 2). In the adjusted analysis, in the low-risk group, total proctocolectomy and, in the high-risk group, pre-operative radiation therapy were linked to POUR. The early and late urinary catheter removal groups did not differ significantly in the occurrence of POUR.
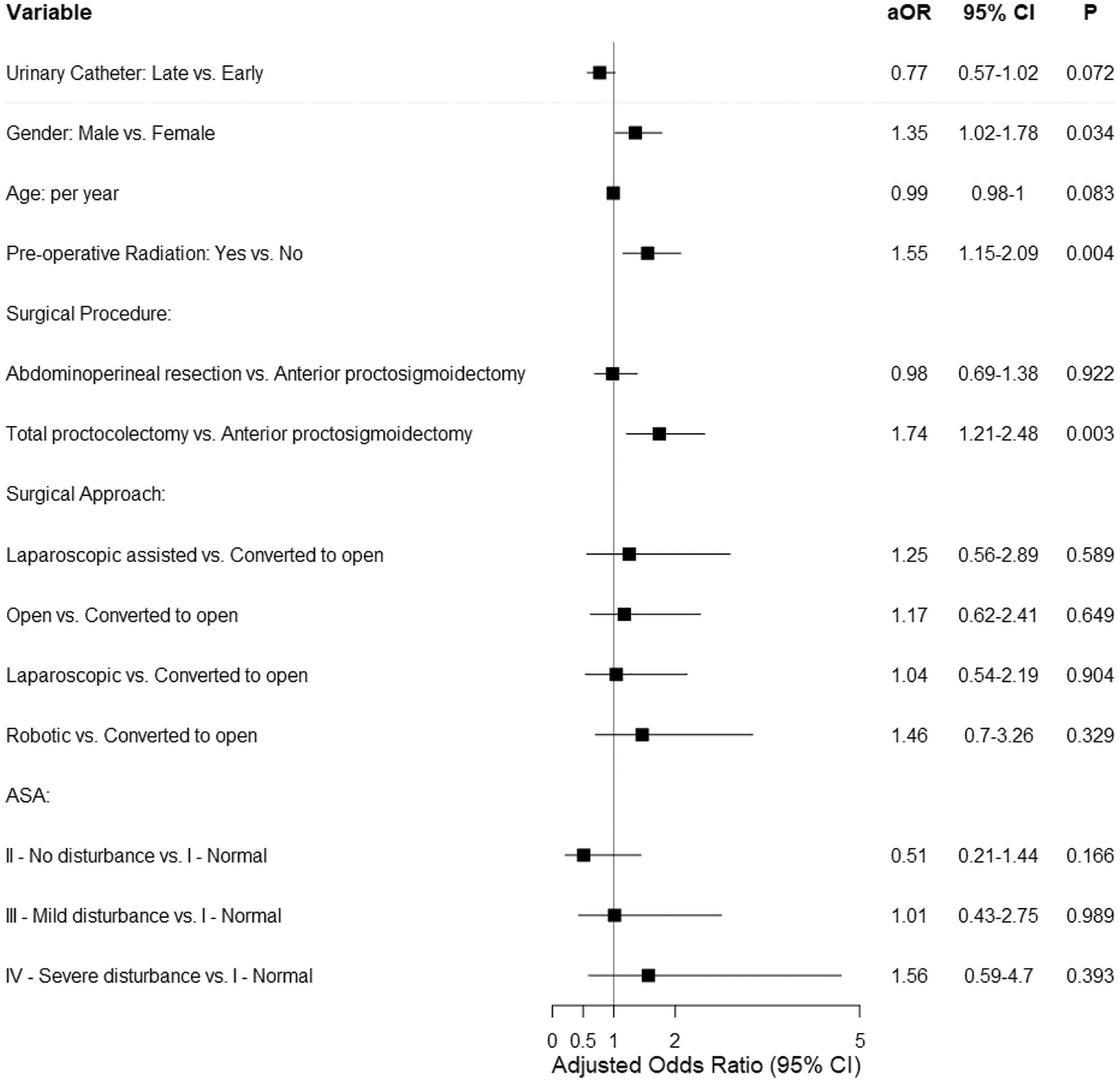
Characteristics associated with post-operative urinary retention (adjusted analysis; n = 1,734).
Characteristics Associated with Occurrence of Post-Operative Urinary Retention (Unadjusted Analysis)
Statistics are presented as mean ± standard deviation, median [25th, 75th percentiles], or frequency (percent). Statistically significant findings are shown in
ASA = American Society of Anesthesiologists.
When urinary catheter removal was analyzed continuously according to the specific day of removal, the multivariable logistic regression models for UTI and POUR showed that a one-day increase in urinary catheter duration resulted in a 21% increase in the odds of having a UTI (OR 1.21; 95% CI 1.09–1.35) and a 12% decrease in the odds of having POUR (OR 0.88; 95% CI 0.80–0.97) (Fig. 3). The McNemar test demonstrated that the proportion of patients who experienced POUR was significantly different from the proportion who had a UTI (p < 0.001). Of the patients who had POUR after catheter removal, 8% (22/280) experienced UTI, and of the patients who did not have POUR, 2.6% (55/2,249) had a UTI (p < 0.001). The median LOS for patients who suffered a UTI was seven days, that for patients who experienced POUR was seven days, and that for patients who experienced both UTI and POUR also was seven days.
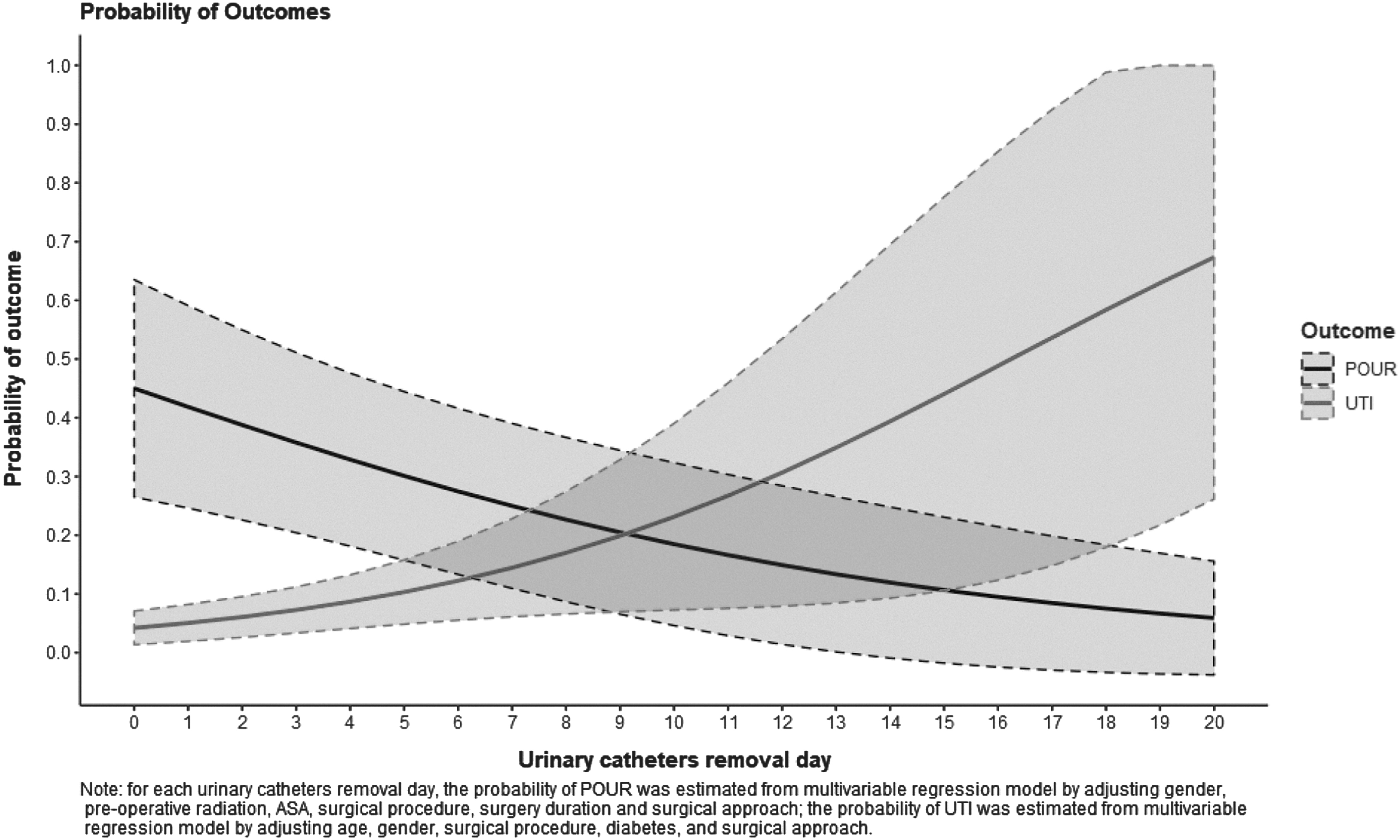
Probability of post-operative urinary retention or urinary tract infection by catheter removal day.
Discussion
Our study demonstrated a significant increase in UTI rate and decrease in POUR rate with each increasing day of urinary catheter duration. Patients in the early-removal group had a significantly shorter LOS than patients in the late-removal group, and patients who experienced POUR requiring straight or re-catheterization were not more likely to have a UTI. These novel findings shed light on the balancing act of POUR and UTI and add significantly to the available literature on the topic, showing that the benefits of early catheter removal are not outweighed by the risk of POUR.
Patients were more likely to have their urinary catheter removed on POD 3 or later if they were older, male, had diabetes mellitus, rectal cancer, pre-operative radiation treatment, laparoscopic surgery, ureteral stents during surgery, abdominoperineal resection, or a longer surgery time. Although no studies, to our knowledge, compare patient characteristics on the basis of the timing of catheter removal or risk level, many of the characteristics mentioned above were identified as UTI or POUR risk factors in other studies [14,15,22,23].
We found an overall UTI rate of 3.2%, with a downward trend over the study period. In a Nationwide Inpatient Sample study of 93,931 patients having colorectal cancer surgery, Kang et al. observed a UTI rate of 5.91% [14], and Ghuman et al. found a UTI rate of 5.13% in their review of 157 male patients undergoing elective colorectal surgery and POD 2 catheter removal [16]. Kwaan et al. saw a 9.8% UTI rate in a review of 205 patients undergoing rectal resections with a median POD 5 catheter removal time [20], whereas Kin et al. found an overall 4.9% UTI rate in their observational study of 143 patients (n = 64 pelvic operations and POD 3 catheter removal) [15]. The lower UTI rate seen in our study may be attributable to our larger sample and regression toward the mean, differing criteria for UTI, and possibly earlier urinary catheter removal because of secular changes in care, namely the introduction of CAUTI as a quality measure and of ERP.
The implementation of ERPs, and possible shifting practice toward early urinary catheter removal by individual surgeons during our study period, likely contributed to the observed decreasing UTI rate. We found only female gender to be associated with UTI overall. Female gender also was associated with UTI in the low-risk group, likely because of the lower number of females with a urologic history who were classified as high risk. Although Kang et al. also identified female gender as a UTI risk factor, they linked age older than 60 years and diabetes mellitus to chronic complications [14]. Our multivariable analysis may not have been powered to identify these factors; however, on univariable analysis, we observed urologic history and total proctocolectomy to be associated with UTI. We saw no difference in UTI occurrence between early and late catheter removal groups, a finding similar to that by Kwaan et al., who found that patients having catheter removal on POD 2 or earlier were not less likely to develop a UTI than those having later removal [20]. However, we did see a significant increase in the UTI rate with each day of urinary catheter placement, consistent with the literature that longer duration leads to higher UTI rates [15,16,20,24].
We also found an overall POUR rate of 11.5%, with an upward trend over the study period. Similarly, Zmora et al. randomized 118 patients having pelvic surgery to POD 1, 3, or 5 urinary catheter removal and found POUR rates of 14.6%, 5.3%, and 10.5%, respectively, and a 10% overall rate [25]; and Lee et al. prospectively found a 13.6% rate in 352 patients having rectal cancer surgery [22]. In a prospective study, Eriksen et al. found an 18% POUR rate in 22 patients undergoing laparoscopic rectal resection with catheter removal within 24 hours in most cases [1], and Kin et al. noted a 21.9% rate in the pelvic surgery group of their observational study [15]. Our larger sample and different catheter removal times may explain the difference between our POUR rate and those observed by Eriksen et al. and Kin et al.
The implementation of ERPs, and possibly shifting practice toward early urinary catheter removal by individual surgeons during our study period likely contributed to the observed increase in the POUR rate. We found no difference in POUR occurrence by removal group; this was in contrast to the findings of Kwaan et al., who observed that POD 2 or earlier catheter removal was associated with POUR [20]. However, we saw a significant decrease in the POUR rate with each day of catheter placement, consistent with the literature that longer duration leads to lower rates of POUR [15,16,20,24]. Multivariable analysis showed that male gender, pre-operative radiation therapy, and total proctocolectomy were associated with POUR, whereas univariable analysis indicated that male gender, pre-operative radiation treatment, older age, longer surgery time, urologic history, anterior proctosigmoidectomy, and an ASA score of 3 were associated with POUR. Lee et al. reported male gender, laparoscopic surgery, and greater intra-operative intravenous fluid (IVF) volume to be POUR risk factors (22), while Zmora et al. found an association between low anastomosis level and POUR and a trend of epidural analgesia being associated with POUR [25]. Kin et al. described greater intra-operative and peri-operative IVF administration associated with POUR [15]. Differences in identified POUR-associated variables may be explained by different sample sizes and data collection; we did not collect data on IVF administration, anastomosis level, or use of epidural analgesia.
In our study population, pre-operative radiation treatment was performed for low rectal cancers, thought to be a POUR risk factor because of the potential for intra-operative pelvic nerve injury or neuropraxia during procedures such as total proctocolectomy with deep pelvic dissection [14,22,23]. Surprisingly, we did not find that abdominoperineal resection (APR) was associated with POUR, similar to Kwann et al. [20] but in contrast to Schreiber, Changchien, and Kang and their colleagues [14,23,26]; it is likely that patients undergoing APR had later catheter removal and therefore less POUR. Although we did not find an association between urologic history or older age and POUR, male patients may have had undiagnosed or untreated urinary dysfunction that contributed to POUR risk [23].
The median LOS overall was six days; low- and high-risk groups had a median of 6 days LOS, and the early vs. late catheter removal groups had a median LOS of 5.26 versus 7 days, respectively. Kwaan et al. also reported a shorter LOS (6.5 versus 8.9 days) with removal on POD 2 or earlier [20]. The median LOS for patients who experienced UTI was 7 days, 1 day longer than the overall median; Kang et al. reported an LOS increase of 8 days with UTI (17 versus 9 days) [14]. The median LOS for patients with POUR was 7 days, 1 day longer than the overall median LOS. Kang et al. reported an LOS increase of 2 days with POUR (11 versus 9 days) [14], and Zmora et al. reported a non-significant trend of LOS increase with POUR (14 versus 9.7 days) [25]. In patients who experienced both UTI and POUR, the median LOS was 7 days; we are not aware of any studies reporting on LOS with both UTI and POUR.
Although the risk of POUR increases with early catheter removal, the mortality rate and economic implications of UTI are higher [11], while the downstream effects of POUR typically are transient and safe, as demonstrated by our data. As we found no association of POUR with UTI, we suggest this risk is acceptable as long as appropriate POUR surveillance and intervention are in place. In contrast, Ghuman et al. reported the odds of having a UTI on top of POUR was 17.44 (95% CI 3.74–81.36), although this was based on a sample of only 157 patients [16]. We also found that patients with UTI, POUR, or both had the same median LOS of 7 days. There were a much higher number of POUR episodes than UTI (n = 282 versus n = 77, respectively); however, POUR does not carry the same association with death, did not increase UTI risk, and does not require antibiotics [26]. Strategies to minimize POUR after proctectomy may include constraining peri-operative IVF volume, pelvic nerve preservation, minimizing sympathomimetic and anticholinergic medication use, using intrathecal versus epidural anesthesia, minimizing pain medication/narcotic use, and pharmacologic prevention (i.e., prophylactic alpha-blocker) [11,20–22].
We acknowledge limitations to the present review; most significantly, the retrospective (non-randomized) nature prevented pre-operative urinary function measurement. Because of a lack of randomization, the late-removal group was characterized by confounding variables that may have contributed to a longer LOS, such as older age and longer surgery times. We also did not collect data on anastomosis level, epidural use, intra-operative IVF volumes, or benign prostatic hyperplasia medication use, which were not available in our dataset. Our large sample overpowered some of our univariable analyses, leading to statistically significant differences that were clinically insignificant. In addition, the practice patterns and patient population seen at our institution may not be representative of other patient populations and therefore may limit the generalizability of our findings to other medical centers. Despite these limitations, this is still one of the largest reviews of proctectomy and post-operative urinary catheter removal in relation to UTI and POUR.
In summary, this retrospective review found no association between POUR and later development of UTI, and the findings support the removal of urinary catheters on POD 1 after proctectomy. Future studies should focus on the prevention of POUR in proctectomy.
Footnotes
Funding Information
No funding was received for this study.
Author Disclosure Statement
None of the authors has any conflicts of interest to disclose.