
Abstract
Background:
Haemophilus parainfluenzae (HPI) is a rare and underreported pathogen. Haemophilus parainfluenzae causes respiratory, soft tissue, and central nervous system (CNS) infections, and endocarditis. Little data on HPI surgical infections are available, especially for intra-abdominal infections (IAI).
Patients and Methods:
Haemophilus parainfluenzae isolates were recovered from patients treated at a rural hospital during a two-year period. Isolation and identification of the pathogen was done according to standard guidelines. A literature review with regard to HPI IAI was done.
Results:
A total of 273 HPI isolates were analyzed, 15 patients had double isolates; HPI was commonly part of a mixed infection. Respiratory tract infections accounted for 64.8%, ear-nose-throat (ENT)/eye infections for 17.9%, genital/urologic infections for 3%, blood stream infections for 1% of cases and 13.2% of HPI isolates involved surgical infections. Thirty-four patients (36 isolates) had HPI surgical infections including 28 skin/soft tissue infections, two bone infections, two perirectal abscesses, one infected hemodialysis catheter, and three IAIs including perforated appendicitis, perforated diverticulitis, and a pelvic abscess 10 days after laparoscopic appendectomy. All three IAIs were mixed infections and successfully managed with percutaneous drainage and antibiotic therapy. More than 90% of HPI isolates in our hospital tested negative for β-lactamase production. A literature review revealed 32 reported cases of HPI IAI including biliary infections (12), peritonitis (9), liver abscess (7), and IA abscess (4) with the majority being monomicrobial; treatment included antibiotic agents and surgery/intervention in most cases. Outcomes were generally favorable.
Conclusions:
Our study confirms data from the literature that HPI is capable of causing a variety of severe surgical infections. More research with regard to this pathogen is warranted.
H
Haemophilus parainfluenzae may be an underdiagnosed cause of infection because of its slow growth, with an incubation period of up to 20 days and fastidious requirement for nicotinamide adenine dinucleotide (or V-factor); which is not always readily available in laboratory culture media [1,16–18]. However, HPI can also be cultured on chocolate agar; best at 35°C in 5% carbon dioxide [1,3,5,19]. According to recent advances in identification techniques, some HPI isolates may have been misidentified and are in fact strains of Haemophilus paraphrophilus [1].
Surgical infections associated with this pathogen have been reported but still little is known about the significance of HPI in patients with intra-abdominal infections (IAI]. However, the pathogen has been reported as both a single infection-causing organism and as part of polymicrobial infections in various settings of IAI such as peritonitis, liver abscesses, biliary tract infections, and retroperitoneal abscesses [8,20–23]. Its significance as part of polymicrobial IAIs is not completely understood. Haemophilus parainfluenzae is frequently found in the gastrointestinal microbiome [1,2,4,19], which may be propagated by the presence of colonic malignancies [24].
We report herein a series of patients with HPI surgical infections in a rural hospital over a two-year period. In addition, a literature search with regard to IAI and orthopedic infections including this rare pathogen was undertaken.
Patients and Methods
This is a retrospective analysis of infections due to HPI in a rural hospital with a focus on surgical infections. During a two-year period (October 2013 through October 2015), the institutional microbiology database was searched for all HPI isolates. A database including all patients with HPI isolates was created and hospital charts were retrospectively analyzed with regard to patient characteristics, hospital course, and outcome, as well as coinfection with other pathogens, with an emphasis on the surgical cases.
Infection was defined as isolation of HPI from any site otherwise considered sterile, together with the presence of clinical symptoms (such as redness, swelling and fever), and laboratory parameters (such as elevated white blood cell count or C-reactive protein), and findings on imaging studies. For surgical cases, HPI was considered a pathogen in all cases including in cases of polymicrobial infections.
The study was approved by the hospital Institutional Review Board. Data are reported as percent of the study population for discrete and as median with range for continuous parameters.
Isolation and identification of HPI was done using previously described methods [1,3,19,25,26]. All specimens were incubated on chocolate agar at 35°C to 37°C in a 5% carbon dioxide atmosphere. If anaerobic bacteria were suspected, aerobic and anaerobic processing was done. For identification of HPI isolates, the RapIDTM NH system (Thermo Fisher Scientific Remel Products, Lenexa, KS) was used. Beta-lactamase production was detected by nitrocefin (cefinase) hydrolysis. No biotyping or testing for mutations in the penicillin-binding protein 3 (PBP3) was done.
PubMed and Google scholar were searched for articles involving HPI in the setting of IAI and orthopedic infections. The data gathered from the literature search were entered into an Excel® (Microsoft Corporation, Redmond, WA) database and analyzed for demographic, clinical, and microbiologic data.
Results
In total 273 isolates were analyzed. In 15 patients (5.5%) this was a double isolation from the same site on two different occasions. The most common site of infection with 64.8% was the respiratory tract. 17.9% of isolates were from patients with ear-nose-throat (ENT)/eye infections, 3% from genital/urologic infections, and three patients (1%) had a blood stream infection (Fig. 1a). A total of 34 patients (36 isolates) with surgical infections caused by HPI were identified. This represented 13.2% of all isolates of HPI (Fig. 1a and 1b). Within the surgical infections, most isolates came from skin/soft tissue infections (n = 28), with the majority being abscesses of the upper extremities (n = 14). The lower extremities, face, and other sites were affected less commonly (Fig. 1c). Most soft tissue infections were monomicrobial and were treated in the emergency department or surgical offices with incision and drainage, followed by oral antibiotic agents such as cefalexin or amoxicillin/clavulanic acid. Subsequent isolation of HPI from the drained pus had no impact on choice of antibiotic agents.

Distribution of 273 Haemophilus parainfluenzae isolates. (
There were two cases of bone infection (one associated with an infected hip replacement) that required orthopedic surgery, two perirectal abscesses (both patients underwent surgical incision and drainage), and one infected hemodialysis catheter (which was subsequently removed).
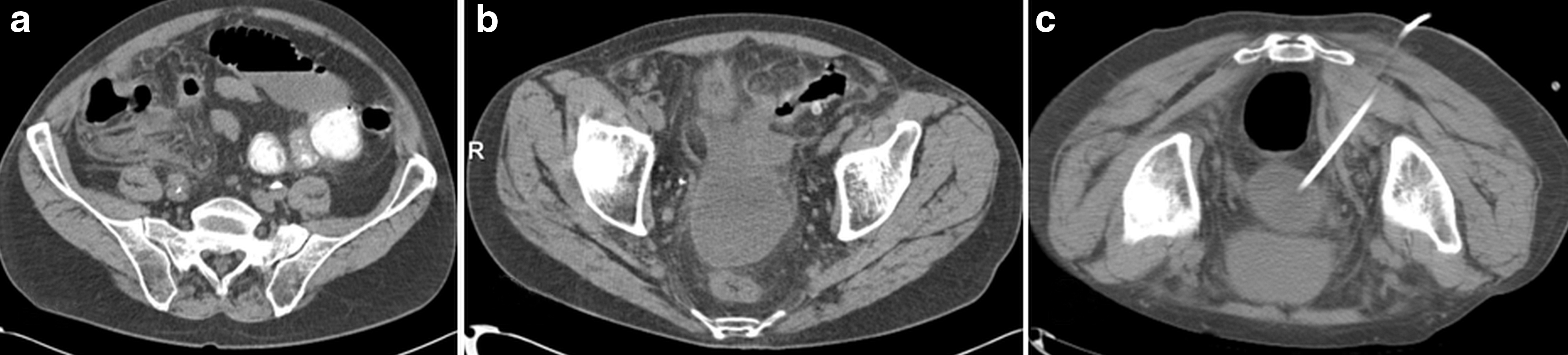
Three patients had IAIs including: a perforated appendicitis in a 78-year-old female (Fig. 2a and 2b), perforated right colonic diverticulitis in a 61-year-old male (Fig. 3a–3c), and intra-abdominal abscesses 10 days post-laparoscopic appendectomy in a 55- year-old female (Fig. 4a–4c). The abscesses were drained percutaneously (Figs. 2b, 3c, and 4c) and all infections were managed successfully with intravenous antibiotic therapy (piperacillin/tazobactam 3.375 g every eight hours in the first patient, levofloxacin 500 mg daily in combination with metronidazole 500 mg every eight hours in the second patient, and ertapenem 1 g every 24 hours in the third patient). The patient with perforated appendicitis underwent interval laparoscopic appendectomy because of ongoing abdominal pain. In all three cases, HPI was part of a mixed infection. Additional pathogens isolated were Escherichia coli, coagulase-negative staphylococci, and diphteroids in the first patient, diphteroids in the second patient, and Escherichia coli, Shewanella putrefaciens, Klebsiella pneumonia, Klebsiella oxytoca, Enterobacter cloacae, enterococci, diphteroids, and Candida albicans in the third patient. Beta-lactamase production was detected in less than 10% of HPI isolates in our hospital. All three isolates from intraabdominal infections were non-beta–lactamase producing [27].

Haemophilus parainfluenzae in perforated appendicitis (computed tomography scan). (
Haemophilus parainfluenzae in perforated right colonic diverticulitis (computed tomography scan). (

Haemophilus parainfluenzae in pelvic abscess after laparoscopic appendectomy (computed tomography scan). (
A literature review revealed a total of 22 articles describing orthopedic HPI infections (Table 1) [28–48], and 30 articles describing IAIs caused by HPI (Table 2). For IAI, one article in Spanish reporting a case of cholecystitis was not considered [49], and four cases reported within larger series of acute appendicitis (n = 1) and cholecystitis (n = 3) focusing on microbiologic data were excluded because no individual patient data were provided [50,51].
Results from Literature Review of Orthopedic Haemophilus parainfluenzae Infections (n = 22)
Demographic and Clinical Data from Literature Review and of Our Three Cases of Intra-Abdominal Haemophilus parainfluenzae Infections (n = 35) According to the Four Major Types of Infection
HPI = Haemophilus parainfluenzae; CAPD = continuous ambulatory peritoneal dialysis.
Table 2 summarizes the demographic, microbiologic, and clinical data of our three cases, as well as the 32 reported cases from 27 articles, according to the four major types of IAI. The first report was published in 1977 by Gallant et al. [55]. Twenty-four single case reports were found, one article included two patients, and three studies included three patients. Only seven cases were reported before 1990 [52–58], 14 between 1990 and 1999 [6,7,18–20,23,59–61], five between 2000 and 2009 [17,21,62–64], and nine (including our three IAI cases) from 2010 until the review was undertaken [8,13,22,65–67]. Fourteen cases occurred in the United States/Canada, 15 in Europe, and six in Asia. The median age of the 15 male and 19 females (one no data reported) was 56 years (range, 9–87).
There were 12 biliary tract infections, nine cases of peritonitis, seven liver abscesses, and seven extra-hepatic intra-abdominal abscesses. All patients received antibiotic agents and the majority (85%) had surgical [18] or interventional [11] procedures done. Cholecystectomy was the predominant surgical procedure [11] and three of the four reported infected continuous ambulatory peritoneal dialysis catheters were removed.
Twenty-four patients (71%) had monomicrobial HPI infections. Regarding the 11 mixed infections, six patients had a single second pathogen and five had multiple additional organisms cultured (Table 1). Outcomes after treatment were generally favorable, with the limitation that no outcome data were reported for nine cases. Five patients had a protracted course or additional surgeries to manage the infection, such as mitral valvuloplasty, liver transplant, and multiple laparotomies with abscess drainage [52,58,64,65]. No fatal outcomes were reported.
Discussion
We herein report a large series of infections caused by HPI. Three cases of HPI IA abscesses were added to the thus far fewer than 40 published cases on HPI IAIs. We analyzed a large series of soft tissue infections (28 patients) and the first two HPI perirectal abscesses and confirm that HPI is involved in joint and bone infections. Nevertheless, HPI is predominantly a respiratory pathogen [1,3]. Because special media are needed to culture the pathogen, HPI may be underreported in various disorders.
Haemophilus parainfluenzae should be considered a primary pathogen in a wide spectrum of surgical infections [8,10,68,69]. It is present in more than 20% of fecal samples and up to 10% of bile samples, and has been isolated in the appendix lumen and perirectal swabs [2,19,70]. Therefore, its presence in IAI should not come as a surprise, with cholecystits and cholangitis reported most often. We have not identified any HPI biliary infections but do not routinely culture bile from cholecystectomy patients.
Our three IAI patients are unique because all suffered perforation of the proximal colon (appendicitis in two patients and ascending colon diverticulitis in the third), and presented with polymicrobial infections, although the exact roles of each pathogen isolated such as central nervous system (CNS) and diphteroids is unclear. Namnyak et al. [71] reported one case of acute appendicitis caused by Haemophilus segnis and Welch et al. [72] reported five cases. Although related to HPI, this pathogen has been re-classified as Aggregatibacter segnis within the Pasteurellaceae family [3].
This analysis was performed at a rural hospital. It is unclear why large series of HPI isolates have not been reported thus far from academic centers and if HPI is more common in our patient population than at other hospitals. At our center, all specimens are routinely cultured on chocolate agar. This single-center observation needs to be confirmed by other centers.
Haemophilus parainfluenzae has also been found to complicate vascular surgery by causing graft failure [73], and in our series, one patient developed infection in a dialysis shunt graft that required removal. Our series also included two bone/joint infections, indicating that HPI is also an important pathogen in orthopedic patients [28–40,43]. Haemophilus parainfluenzae septic arthritis seems more common than osteomyelitis and may involve prosthetic devices.
Haemophilus parainfluenzae soft tissue infections have thus far rarely been reported [74] and this is a first series of such patients. We routinely culture specimens from drained abscesses, and specimens are submitted for aerobic and anaerobic culture. Three HPI psoas abscesses have been published with two developing after endoscopic retrograde cholangiopancreatography (ERCP) [20,22,61], however these reports were unable to confirm if HPI had been translocated from the oropharynx or the biliary tract.
Haemophilus parainfluenzae should also be recognized as a pathogen in non-surgical patients. We had three patients with HPI-positive blood cultures (all were single isolates). No surgical patient had a positive blood culture and there was no case of endocarditis. Blood cultures were drawn as part of our sepsis protocol and the three patients had clinical symptoms of infection. Haemophilus parainfluenzae was concluded as the causative pathogens of these infectious episodes, with the respiratory tract being the most likely source.
Most Haemophilus spp. are susceptible to β-lactam antibiotic agents, aztreonam, fluoroquinolones, tetracycline, chloramphenicol, macrolides, and trimethoprim/sulfamethoxazole. Beta-lactamase–producing HPI strains and strains resistant to beta-lactams because of mutations in penicillin-binding protein 3 (PBP3) have recently emerged [75,76]. Tinguely et al. [77] reported a multi-drug–resistant (MDR) HPI isolate in a homosexual male. Although most HPI isolates remain susceptible to carbapenems, resistance to this class of agents has also been found [75), leaving few treatment options [77–-79). More than 90% of HPI isolates in our study were found to be negative for β-lactamase production, however, resistance data are limited because no testing for mutations in PBP3 was done.
Haemophilus parainfluenzae is predominantly a respiratory pathogen. Its role in endocarditis is well known to cardiothoracic surgeons, however, it is also causes a wide spectrum of other surgical infections. To isolate and identify HPI from surgical infections, adequate intra-operative samples should be obtained, strict culture procedures should be followed, and microbiology laboratories should be aware of the potential presence of atypical organisms because not all surgical infections are caused by common pathogens such as staphylococci and gram-negative bacilli, among others [80). Emergence of MDR HPI strains is a concerning development and HPI may cause endocarditis when entering the blood stream [16], which is well documented by the case reported by Miquel-Goulenok et al. [13]. Most recently, De Castro et al. [81] reported a pregnant female suffering from coronavirus (not COVID19) infection who developed HPI endocarditis with multiple cerebral emboli requiring emergent cesarean delivery followed by open heart surgery.
Recognition of HPI as an important surgical pathogen seems essential. More research regarding this emerging pathogen in surgical patients is certainly needed.
Footnotes
Funding Information
There are no financial disclosures to be reported.
Author Disclosure Statement
There are no conflicts of interest.