
Abstract
Background:
Intra-abdominal infections (IAI) remain a substantial cause of worldwide morbidity, mortality, and healthcare cost burden. The World Surgical Infection Society (WSIS) was organized to help improve global outcomes from surgical infections. An initial project for the WSIS was to assess how surgeons treat common IAI in their regions.
Methods:
A 10-item questionnaire was distributed to members of four surgical societies dedicated to the study of surgical infections. Questions were related to common treatment decisions in the management of IAI, with the intention of identifying differences and potential controversies in patient care. Responses were analyzed by comparing percentages with 95% confidence intervals.
Results:
Globally, management was relatively similar for peritoneal irrigation (most commonly with saline or other crystalloid: China, 83.2% ± 5.8%; North America, 93.2% ± 6.4%; Europe, 85.7% ± 25.9%; and Latin America, 71.8% ± 6.9%). More varied responses were seen for the management of specific disease states; for instance, for cholangitis, endoscopic retrograde cholangiopancreatic interventions were more common in North America (83.1% ± 9.6%) and less common in China (28.1% ± 7.0%). For appendiceal abscesses, percutaneous drainage and antibiotic treatment was most common in North America (93.2% ± 6.4%) and least common in Latin America (19.6% ± 6.1%). Additionally, the management of fascial and wound closures were different by region. Vacuum-assisted wound closure after fascial closure was utilized commonly in North America (32.2% ± 11.9%), Europe (28.6% ± 33.5%), and Latin America (27.6% ± 6.9%), however, was less commonly utilized in China (9.9% ± 4.4%), where there was higher rate of primary skin closure (85.7% ± 5.4%).
Conclusion:
Through its partnership with other surgical infection societies, the WSIS aims to develop evidence-based guidelines for more consistent pattern of IAI management globally. Delving further into why their practices differ may help improve worldwide outcomes.
Intra-abdominal infections (IAI) are a substantial cause of worldwide morbidity, mortality, and healthcare cost burden. Several evidence-based guidelines have been established to standardize the management of IAI, the pillars of which include adequate resuscitation, appropriate antibiotic administration, and obtaining source control [1]. Despite advancements in diagnostics, critical care support, pathogen detection, antimicrobial therapy, and surgical techniques, overall mortality from IAI remains high at 10.5% [6]. The World Surgical Infection Society (WSIS) was organized to help improve global outcomes from surgical infections in resource-limited low- and middle-income countries (LMICs), where management of IAI poses a unique set of challenges [4]. An initial project for WSIS is to assess specifically how surgeons treat common IAI in their regions.
Background
Intra-abdominal infections are a heterogenous set of clinical pathologies, ranging from non-ruptured appendicitis to feculent peritonitis. They are generally classified into uncomplicated and complicated IAI. Uncomplicated IAI involve a single organ, and do not extend to the peritoneum. These may be treated either with antimicrobial therapy alone, with surgical source control, or both. Delay in diagnosis or treatment of uncomplicated IAI can result in progression to complicated IAI. These infections extend beyond the source organ into the peritoneal cavity, causing either focal or diffuse peritonitis. These are a substantial source of morbidity and mortality, particularly if mismanaged. Although this classification separates the two entities by an anatomic barrier, it does not provide information regarding severity of disease [2].
Stratifying the types of diffuse peritonitis offers another way to categorize IAI. Primary peritonitis refers to diffuse bacterial infection without loss of integrity of the gastrointestinal tract. This is generally seen in patients with cirrhosis who have ascites, or patients with an indwelling peritoneal dialysis catheter. These are generally managed with antibiotic agents alone. In contrast, secondary peritonitis is an acute peritoneal infection resulting from loss of integrity of the gastrointestinal tract. This is more common in surgical patients, and typically managed by obtaining source control, as well as antibiotic therapy. Secondary peritonitis can be localized (walled-off or contained by adjacent organs, such as abscess) or diffuse. Recurrent or ongoing infection of the peritoneum that occurs >48 hours after presumed surgical source control of secondary peritonitis is considered tertiary peritonitis. This is often seen in critically ill or immunocompromised patients and may be associated with multi-drug–resistant organisms. Although tertiary peritonitis is essentially a complication of secondary peritonitis, it is considered a separate entity with higher morbidity and mortality [3].
The optimal management of patients with IAI relies on a multimodal approach, involving early diagnosis, judicious use of antimicrobials, and achieving source control. Source control refers to all measures necessary to eliminate infection and ongoing contamination, as well as correct anatomic derangements, to restore normal physiology [7]. Several methods have been described for source control in IAI. These entail drainage of abscesses or infected fluid collections, debridement of necrotic tissues, repair of perforations, removal of infected organ, and resection of ischemic bowel. The procedure of choice depends on the patient's specific pathology and clinical status [2]. This survey-based study aims to elucidate some characteristics of IAI in several international settings, while also examine source control trends of providers in these regions.
Methods
Study design
A 10-item questionnaire was distributed electronically to surgeon members of four societies dedicated to the study of surgical infections: The Surgical Infection Society (SIS) North America, SIS Europe, SIS Latin America, and the Chinese Society of Surgical Infections. The questions were related to common treatment decisions in the management of IAI, such as peritoneal irrigation, fascial closure, skin closure, appendiceal abscess, cholangitis, and perforated viscus (Table 1), each with several answer choices to select from. The survey was administered via electronic mail and an open source platform (www.surveymonkey.com) was utilized to collect the responses anonymously. Participation was voluntary and anonymous. Incentives for participation were not provided.
Questionnaire
Statistical analysis
Data obtained from the completed questionnaires were entered into a Microsoft Excel® database (Microsoft, Redmond, WA). For each question, the answer choice with the highest percentage response was compared with the same answer choice within the other regions. Responses were analyzed by comparing percentages with 95% confidence intervals and compared using the Pearson χ2 with a Yates correction. A Bonferroni correction was used to correct for multiple comparisons. A p value ≤0.01 was considered statistically significant.
Results
Total responses from each society were as follows: SIS North America (n = 59), SIS Latin America (n = 163), Chinese Society of Surgical Infection (n = 156), and SIS Europe (n = 7). Not surprisingly, the majority of members of each regional society practice surgery in that particular region (Fig. 1)
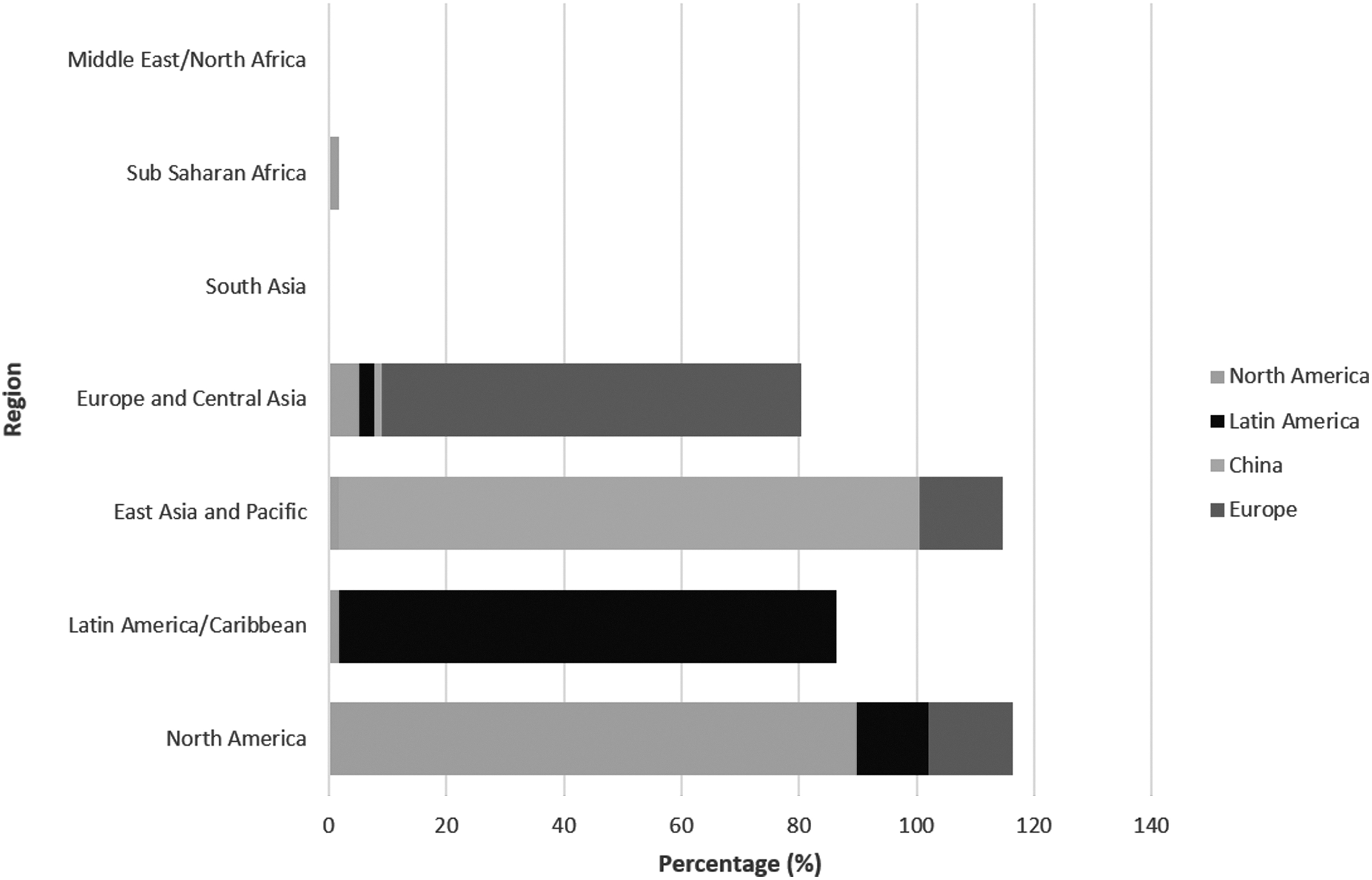
Most common region of practice.
For patients with secondary peritonitis, infections of appendiceal origin were more common in China (57.4% ± 7.8%) and Latin America (59.5% ± 7.5%), compared with North America (29.3% ± 11.7%); p ≤ 0.01. Among North American providers, colorectal infections were more common (48.3% ± 12.9%), compared with China (11.0% ± 4.9%) and Latin America (26.4% ± 6.8%); p ≤ 0.01 (Fig. 2).
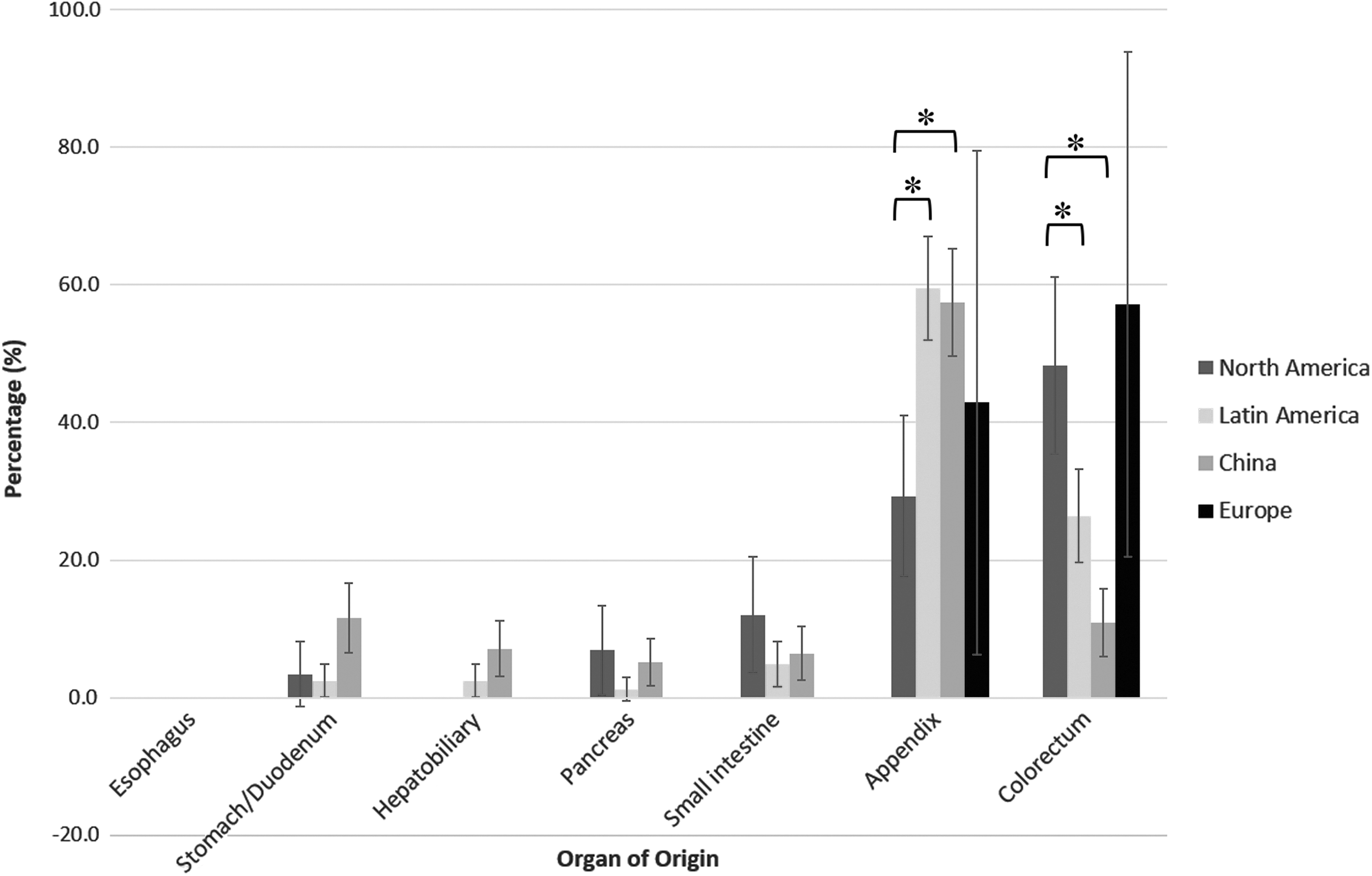
Most common organ of origin in secondary peritonitis.
In patients with localized peritonitis, for example, adults who present with complicated appendicitis and 5-cm abscess, in addition to antibiotic therapy, it was more common for North Americans to perform percutaneous drainage (93.2% ± 6.4%) than in Latin America (19.6% ± 6.1%) or in China (43.4% ± 7.7%); p ≤ 0.01. In Latin America, the most common initial management was laparoscopic drainage, with or without appendectomy (57.7% ± 7.6%); compared with North America (1.7% ± 3.3%) or China (17.6% ± 5.9%); p ≤ 0.01. In China, although percutaneous drainage was most common, 30.8% reported antibiotic agents alone as the most common initial management, compared with North America (1.7% ± 3.3%) or Latin America (3.1% ± 2.6%), where antibiotic therapy was supplemented by a source control procedure (Fig. 3).
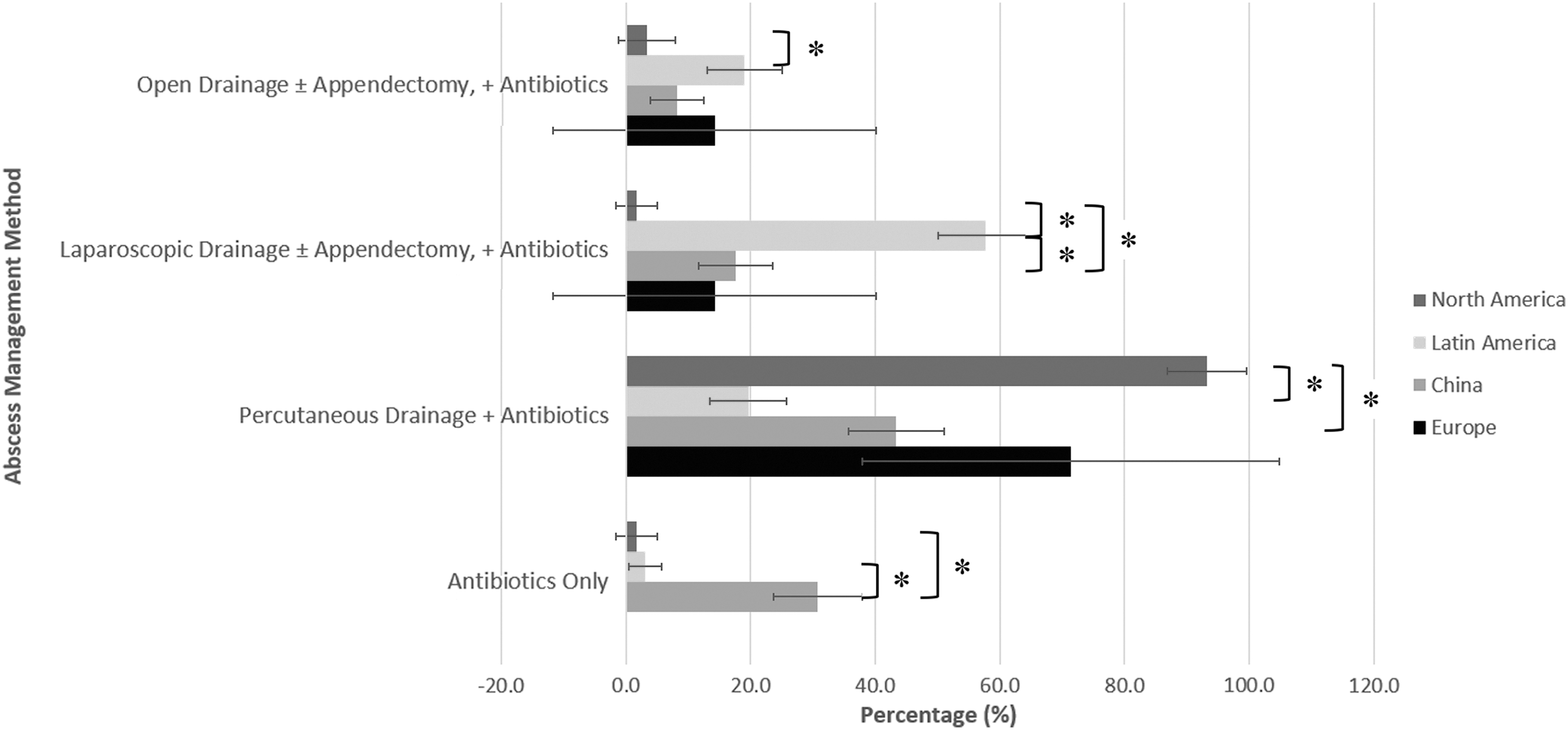
Most common initial management strategy of a 5 cm appendiceal abscess.
For hemodynamically stable and healthy patients with focal left lower quadrant contamination secondary to sigmoid diverticular perforation, it is preferred by surgeons in China to perform sigmoid resection with end colostomy (Hartmann's procedure) (63.2% ± 7.4%), compared with providers in North America (28.8% ± 11.6%) and Latin America (36.8% ± 7.4%); p ≤ 0.01. North American and Latin American surgeons were more likely to perform primary anastomosis without diversion (44.1% ± 12.7% and 40.5% ± 7.5%, respectively), compared with providers in China (4.9% ± 3.3%); p ≤ 0.01 (Fig. 4).
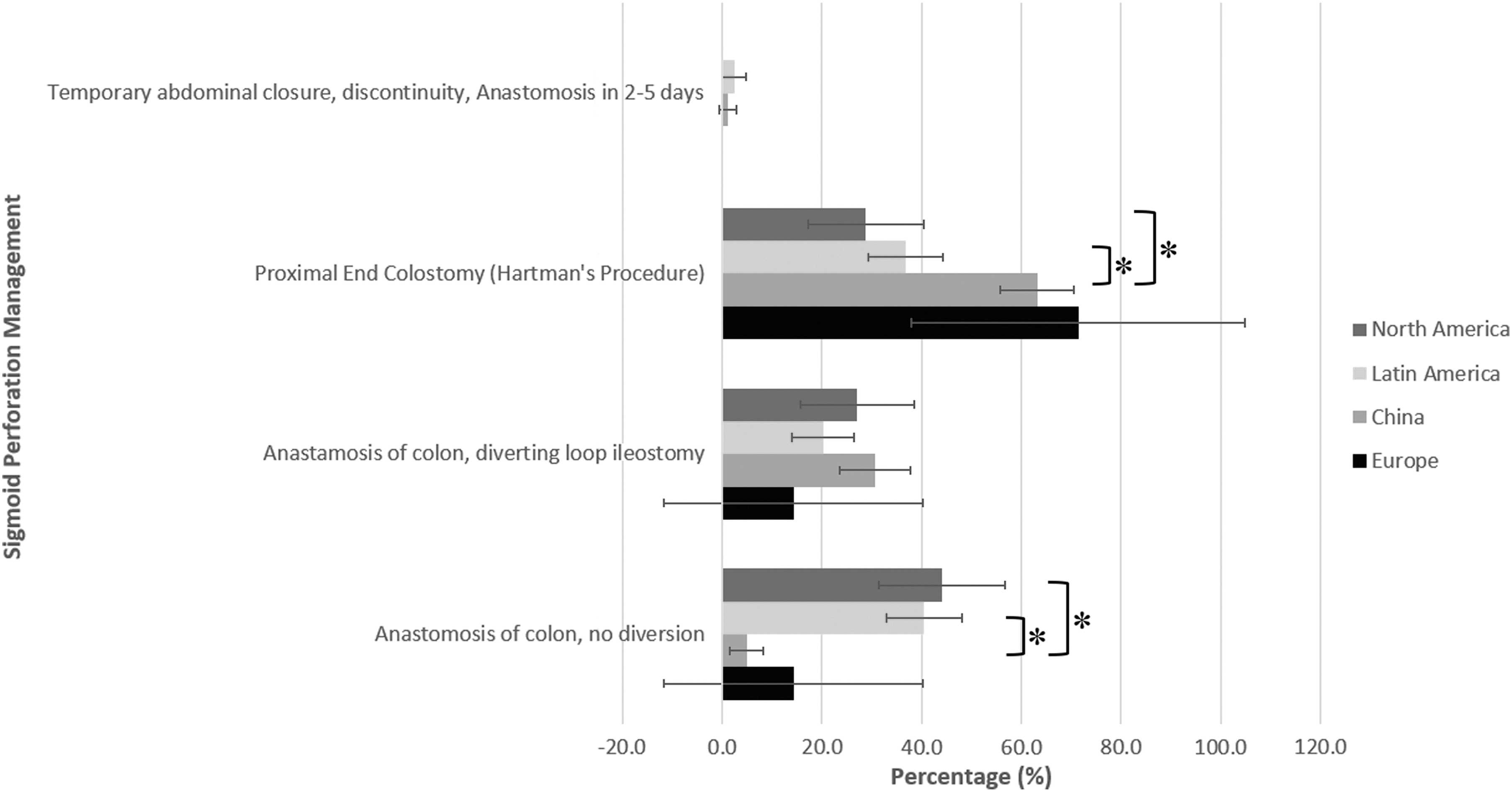
Preferred management of sigmoid diverticular perforation with localized contamination.
In patients with diffuse peritonitis, in which a source control procedure has been performed, most providers conducted irrigation of the abdomen with saline or other crystalloid (Fig. 5).

Preferred irrigation method after source control procedures in peritonitis.
In cases in which re-laparotomy is a consideration, for example, in patients with peritonitis secondary to bowel perforation who remain on vasopressor therapy intraoperatively after bowel resection is performed, among providers in China and North America, primary fascial closure with or without retention sutures was preferred (86.6% ± 5.2% and 72.9% ± 11.3%, respectively) over temporary fascial closure devices. In Latin America, temporary fascial closure with mesh or Bogota bag was a common preference, compared with North America or China. Additionally, negative pressure therapy, especially the use of commercially available devices such as Abthera™ (KCl USA Inc., San Antonio, TX), were preferred among North American surgeons compared with China (Fig. 6).
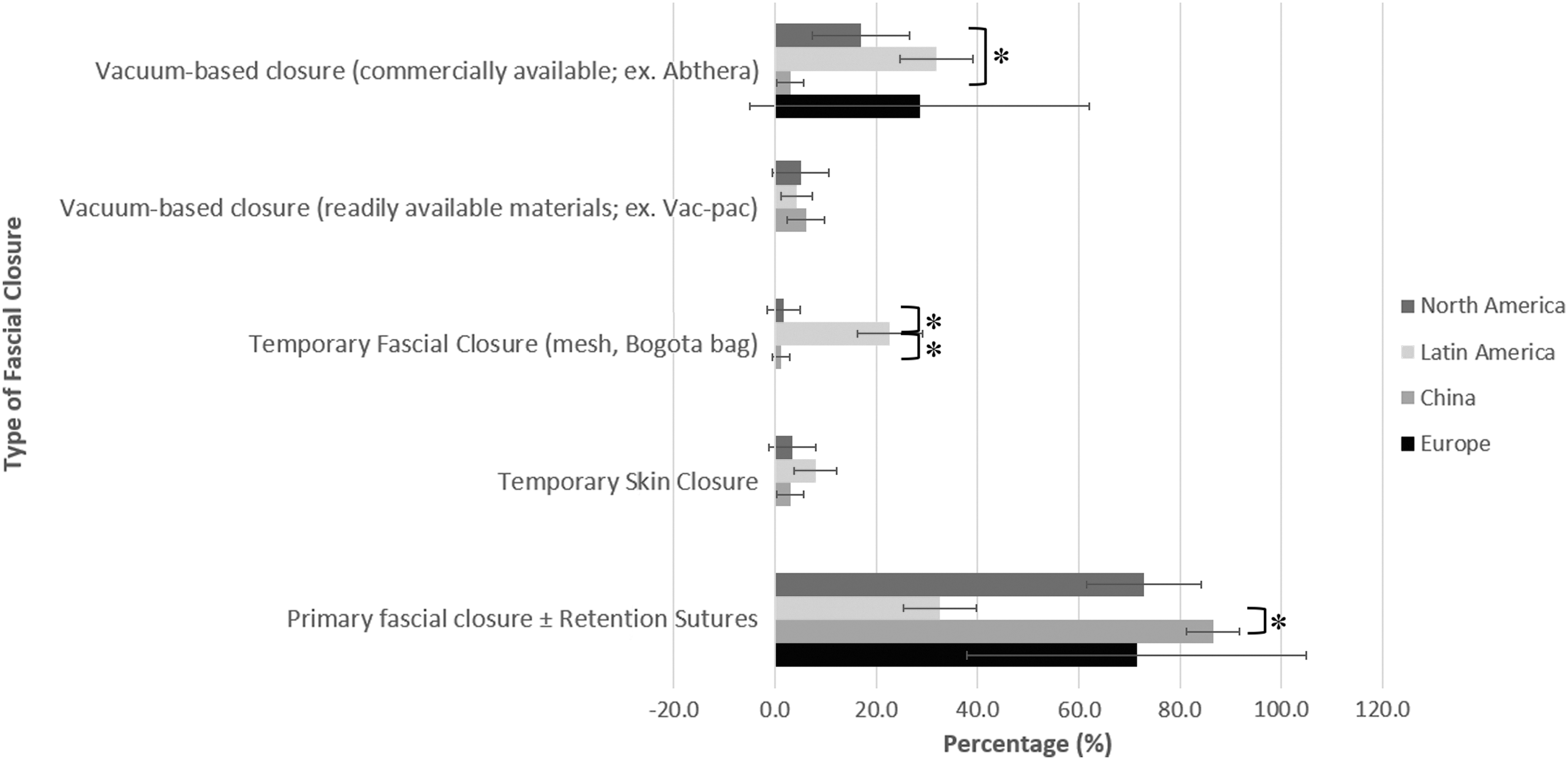
Preferred abdominal fascia management while receiving vasopressor therapy.
In laparotomy cases in which adequate source control has been achieved and the fascia is closed, percentage of vacuum skin closure after fascial closure was fairly consistent between surgeons in North America (32.2% ± 11.9%), Europe (28.6% ± 33.5%), and Latin America (27.6% ± 6.9%), however, was much lower in China (9.9% ± 4.4%), where there was higher rate of primary skin closure (85.7% ± 5.4%; Fig. 7).
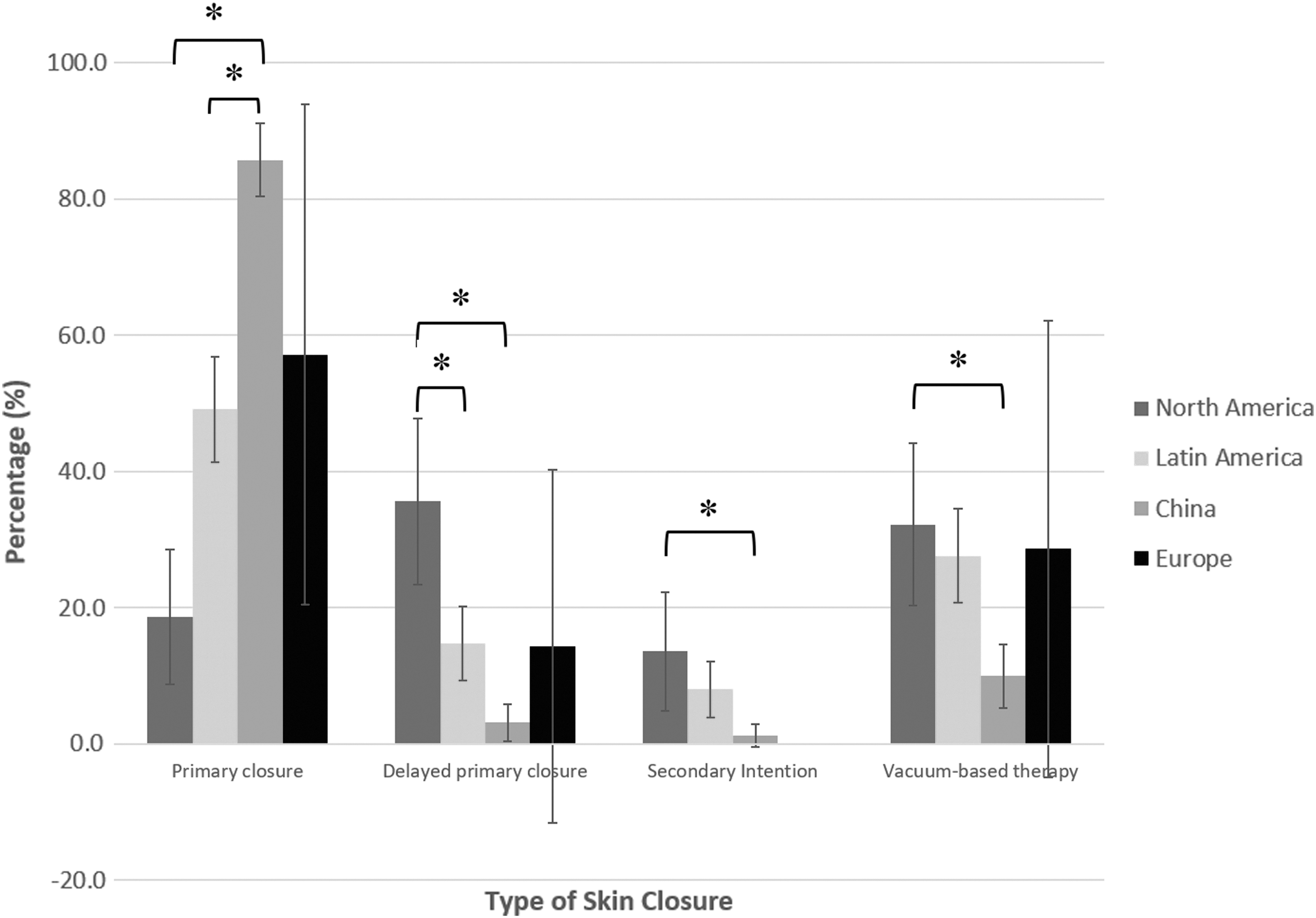
Skin closure after source control laparotomy in diffuse peritonitis.
For patients with cholangitis secondary to choledocholithiasis, endoscopic retrograde cholangiopancreatography with interval cholecystectomy during the same admission was the most common management strategy among North American providers (83.1% ± 9.6%), and less common among Chinese providers (28.1 ± 7.0%); p ≤ 0.01. However, among Chinese providers, laparoscopic or open common bile duct exploration, with cholecystectomy was preferred (36.9% ± 7.5% and 31.3% ± 7.2%), and differed substantially in North America (8.5% ± 7.1% and 5.1% ± 5.6%); p ≤ 0.01 (Fig. 8).
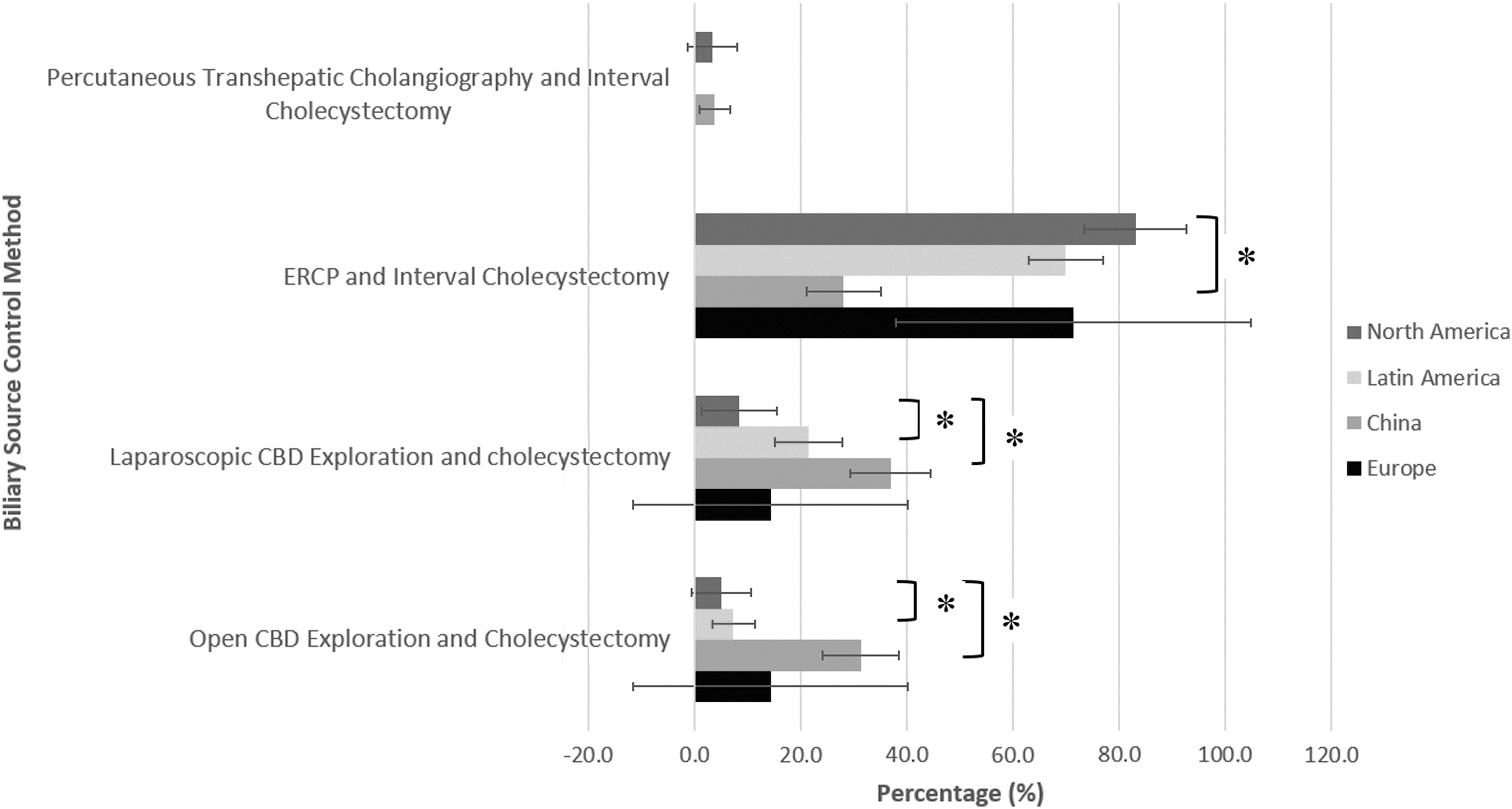
Most common management of cholangitis secondary to choledocholithiasis.
In patients with typhoid ileal perforations that present after four days of symptoms, providers in North America preferred to perform segmental bowel resection and anastomosis (80.4% ± 10.4%), compared with providers in Latin America (44.2% ± 7.6%) and China (19.6% ± 6.1%), where exteriorization of the perforation with ostomy creation was preferred (Fig. 9). Statistically significant differences were not observed between providers in other regions and providers in SIS Europe, given their paucity of responses.
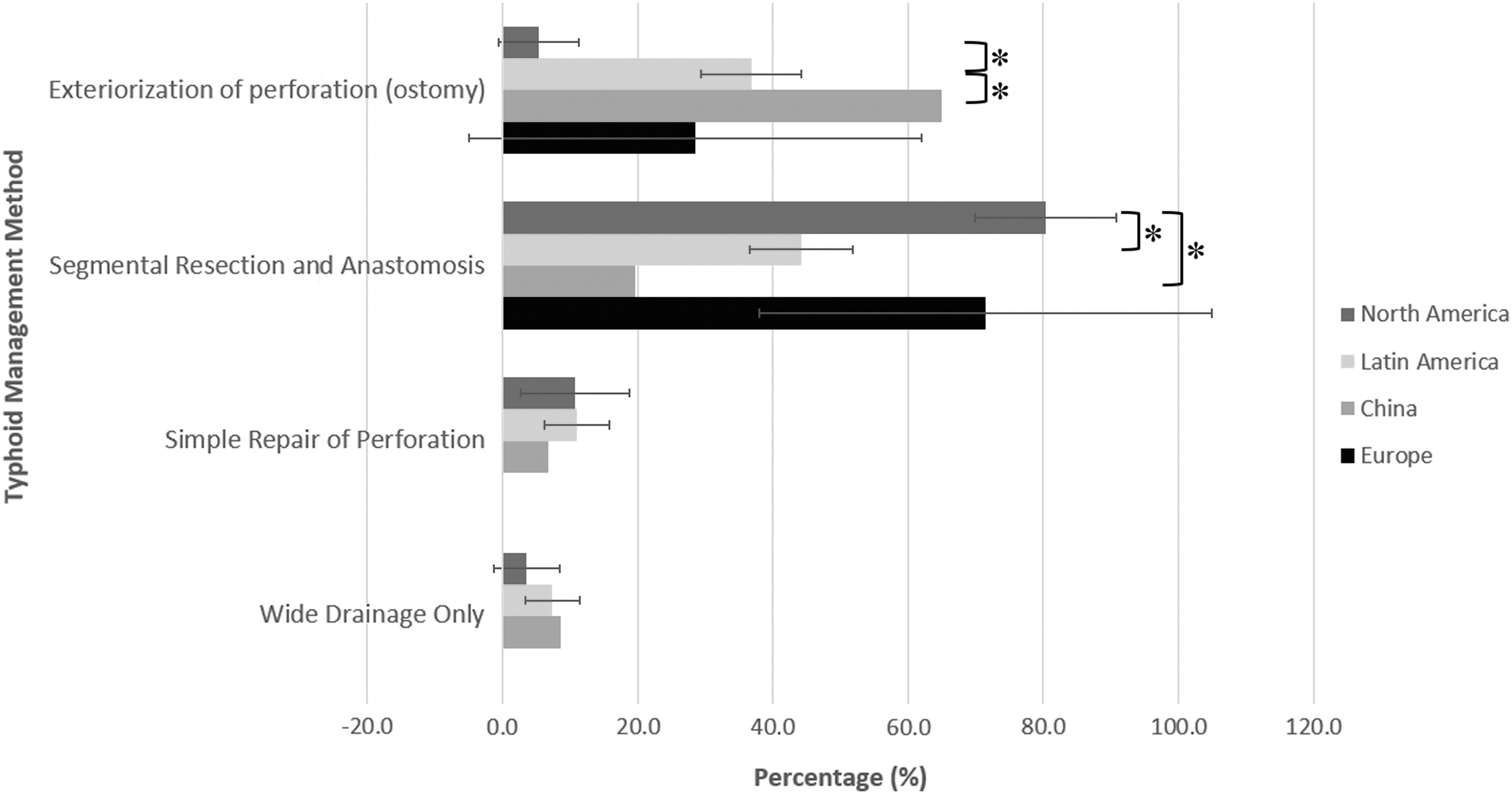
Preferred management of generalized peritonitis secondary to typhoid ileal perforation.
Discussion
The optimal management of patients with IAI relies on a multimodal approach, involving early diagnosis, judicious use of antimicrobials, and achieving source control [4]. Despite advances in methods and technologies for achieving source control, mortality from IAI remains high [6]. In cases of focal peritonitis with abscess, such as in complicated appendicitis, non-operative methods, such as percutaneous drainage of the abscess, either under ultrasound or computed tomography (CT) guidance, provides a means to avoiding a more involved surgical procedure. However, CT may not always be available in LMICs, and ultrasound-guided therapy is likely limited to superficial abscesses. An interventional radiologist performs these procedures and is often not available in certain regions. Thus, operative intervention for abscesses such as laparoscopic or open drainage are the more commonly available option. Laparoscopic procedures, either for diagnosis of pathology, removal of infected organ (appendix, gallbladder), or for drainage of abscesses, are performed routinely in high-income countries. Laparoscopy offers benefits of reduced pain, faster return to normal function, reduced hospital stay, and reduced post-operative surgical site infections [7]. However, its use in LMICs is limited because of high cost, lack of equipment, and lack of training programs for providers [8]. Therefore, laparotomy with open drainage remains the primary method of achieving source control in many regions.
In patients with localized contamination, for example in the left lower quadrant from a sigmoid diverticular perforation, Hartmann procedure has been considered the procedure of choice in unstable and unhealthy patients, however, in clinically stable patients, primary resection and anastomosis, with or without a diverting ostomy, remains an option [7]. Interestingly, despite having a hemodynamically stable and healthy patient, some of the surveyed providers still most commonly perform a Hartmann procedure.
In diffuse peritonitis, inadequate source control is associated with increased mortality. Several strategies for re-operation have been described, such as the open abdomen concept and re-laparotomy, either planned or on-demand (when patient's condition necessitates re-operation) [7]. In resource-limited settings, commercially available negative pressure closure devices are expensive, and the use of Bogota bags or sandwich-type vacuum packs made of readily available materials have been described for damage control operations [9]. Regarding a re-laparotomy strategy, in an LMIC setting, no difference was observed between planned re-laparotomy versus on-demand laparotomy in terms of length of hospital stay, morbidity, or mortality. However, patients who underwent planned relaparotomy were found to have increased need for ICU admission, and those who underwent multiple re-operations were found to have worse outcomes [10].
For cholangitis secondary to choledocholithiasis, endoscopic retrograde cholangiopancreatography is the treatment of choice for biliary decompression [7]. However, in settings in which endoscopic decompression may not be an option, either because of availability of the technology or patient factors, laparoscopic or open common bile duct exploration with concurrent cholecystectomy are still performed routinely.
Typhoid fever is endemic in parts of Latin America, Asia, and Africa and typhoid ileal perforations are a substantial public health concern because of high morbidity and mortality rates [6]. These are rare in Western countries, where small bowel perforations are more commonly caused by non-infectious etiologies [7]. In our survey, for patients with delayed presentations who have generalized peritonitis, interestingly, the preferred management strategy among North American providers was resection with anastomosis whereas in Latin America and China, surgeons preferred to exteriorize the perforation and create an ostomy.
Given the complexity of IAI, observational studies and database analyses need to be encouraged [11]. Our study is important because it is the first study that demonstrates practice trends between members of the various surgical infection societies regarding management of IAI in their regions. Strengths of the study are the high response rates from most of the societies, and the variety of questions asked, which can help provide an overview of emergency surgical decision-making across the globe. However, there are several limitations. The study was survey based, with pointed multiple-choice answers containing the most commonly performed procedures. Providers may have alternative management strategies that are not provided as answer choices. In addition, the generalizability of the responses is hindered by the fact that little is known about the actual demographics of the providers. Practice habits can be affected by social, cultural, and economic factors. It is not clear from the responses as to what type of working environments the surgeon practices, for example, whether they practice is a high-resource or low-resource center. In addition, their level of training is unknown. For example, a practitioner may prefer to perform an open source control procedure if they are not laparoscopically trained.
Conclusion
Through its partnership with other surgical infection societies, WSIS aims to develop evidence-based guidelines for source control in the setting of IAI. This initial observational study into IAI management habits of surgeons globally may help elucidate regional differences and where improvements can be made. Although multiple international studies have sought to determine etiologies, outcomes, and mortality rates of IAI, in order to create standards and evidence-based practices that could potentially improve management worldwide, these studies are unable to incorporate data on variations in patient populations and specific care provided at individual institutions. This offers areas for quality improvement, where internal institution review by stakeholders (hospital management, policymakers, clinicians) and evaluation of local data, for example, review of practice habits of surgical providers, can help strengthen the specific care needed for IAI in that particular population [4]. Future directions may involve delving further into reasons why their practices differ, and analyzing their individual outcomes (rates of infection, antibiotic resistance, etc.), may help formulate solutions that are targeted to those regions.
Footnotes
Funding Information
The authors have no financial disclosures.
Author Disclosure Statement
No competing financial interests exist.