
Abstract
Background:
Surgical antimicrobial prophylaxis (SAP) refers to the utilization of antibiotic agents for the prevention of surgical site infections (SSI), to prevent SSI-associated morbidity and mortality, reduce duration and cost of healthcare, and cause minimal adverse drug effects. The adherence rate among surgeons for the available international and national guidelines and optimal practice remains considerably low in many hospitals, especially in developing countries. The objective of this study was to assess the knowledge and compliance rate for SAP guidelines among various surgical specialties and those involved in providing SAP.
Methods:
An institution-based exploratory, multi-specialty, collective, mixed method approach (qualitative and quantitative) was used to assess the knowledge and compliance rate for SAP guidelines among the consultants and residents of surgical specialties. Quantitative analysis was performed using a pre-tested questionnaire. For qualitative analysis, focus group discussions were conducted. Thematic analysis was conducted by the Theoretical Domains Framework (TDF) and the Capabilities, Opportunities, Motivation and Behaviour (COM-B) model.
Results:
Twenty-eight focus groups and 16 paired interviews were undertaken. On thematic analysis six significant themes were noted and mapped to the COM-B model, and subthemes mapped to the relevant TDF domains in a combined framework. Key themes recognized were: (1) solitary focus on surgical skills; (2) following the hierarchy is more important than guideline compliance; (3) doubts and overcautious attitude of surgeons hinders appropriate SAP prescribing; (4) non-availability in-hospital supply of antimicrobial agents; (5) patient characteristics and type of surgery play a role in prescribing SAP; and (6) lack of national and local guidelines.
Conclusions:
The knowledge and attitudes of surgeons toward appropriate SAP prescribing are crucial factors for execution of guidelines. Including them in policy making decisions can help in strong execution of the same.
Despite recent medical and surgical developments, surgical site infections (SSI) remain a substantial problem and are the leading cause of unintended and potentially avoidable hospital re-admission of patients who have recently had surgeries [1,2]. Data from the United States Centers for Disease Control National Nosocomial Infections Surveillance (CDC NNIS) [3] system show that SSIs have been the second most common cause of nosocomial infections [4–6], thus comprising a remarkable share of health-care-associated infections (HCAI). Whereas the global estimates of SSI have varied from 0.5% to 15%, depending on the procedure, operative site, and degree of contamination, studies in India have consistently shown higher rates ranging from 23% to 38% [7]. Because of the devastating complications of SSIs, there is an urgent need to consider an integral approach for curtailing such infections. A multipronged approach taking into account pre-operative, peri-operative, and post-operative measures is necessary for preventing SSIs as suggested by the World Health Organization (WHO) [8].
Among the other parameters to curtail SSI, surgical antibiotic prophylaxis (SAP) is one of the critical components, because it affects not only the outcome of the patient but also has long-term effect on antimicrobial resistance that in itself is a threat to the patient and to the community.
Surgical antibiotic prophylaxis refers to the utilization of antibiotic agents for the prevention of SSIs and is a short-term antibiotic usage directed at possible agents before, during, or immediately after surgery [9]. The goal of antimicrobial prophylaxis is to avoid SSI-associated morbidity and mortality, reduce duration and cost of healthcare, cause minimal adverse drug effects, and have minimal adverse effects on the microbial flora of the patient and the hospital [10]. Many studies have shown that risk of infection in surgical patients is higher without SAP than those receiving prophylactic antibiotic agents [11,12].
Evidence-based strategies and therapeutic guidelines for SAP have been published by the CDC and WHO [2,13], which provide specialists with a consistent approach to the safe and effective use of antibiotic drugs for the prevention of SSIs, based on currently available clinical indications and emerging issues [11]. Despite this, errors in selection, timing of dose, and duration of prophylactic antimicrobial agents are common. Studies have reported that the adherence rate among surgeons for the guidelines and optimal practice remains considerably low in many hospitals, especially in developing countries [14,15]. Studies worldwide have observed high rates of inappropriate SAP prescribing [16–19]. Inappropriate use, such as prolonged duration of surgical prophylaxis, contributes to the overall encumbrance of antibiotic use in the community and exposes patients to adverse reactions and thus contributes to suboptimal patient care and outcomes, and is also considered a trigger for the emergence of antimicrobial resistance (AMR) [20]. Therefore, appropriate use of SAP is required to improve patient care by minimizing adverse effects, emergence of resistance, and cost by reducing the burden of inappropriate prescribing on both the patient and health care system.
The objective of this study was to assess the knowledge and compliance rate for SAP guidelines among the consultants and residents of the surgical specialties and those involved in providing SAP, namely, orthopedics, surgery, obstetrics and gynecology, otorhinolaryngology, plastic surgery, pediatric surgery, and anesthesiology.
Methodology
Study area
The study was conducted in Jawaharlal Nehru Medical College Hospital (JNMCH), the largest teaching hospital and tertiary referral center of western Uttar Pradesh, India. Approximately 20,000 surgeries are performed annually.
Study population
Consultants and residents of JNMCH from the surgical specialties and those involved in providing SAP, namely, orthopedics, surgery, obstetrics and gynecology, otorhinolaryngology, plastic surgery, pediatric surgery, and anesthesiology were included. A total sample size of 184 participants was selected by purposive sampling technique.
Study design
An institution-based exploratory, multispecialty, collective, mixed method approach (qualitative and quantitative) was used to assess the knowledge and compliance rate among the consultants and residents of abovementioned specialties for SAP guidelines.
Inclusion criteria
Consultants and residents of JNMCH from the surgical specialties and involved in providing SAP, who were interested in participating were included in the study.
Exclusion criteria
Residents and consultants of non-surgical specialties and surgical specialties who did not give consent for participation were excluded.
Data collection
The study included a pre-tested self-administered questionnaire for quantitative analysis and focus group discussions for qualitative analysis. The questionnaire was formulated to evaluate the knowledge concerning the parameters of antimicrobial prophylaxis by six closed-ended questions. Evidenced-based SAP guidelines developed by the WHO and the CDC [2,13] were used as a reference in our study. The questionnaire was validated by face validity and a pilot study on 10% of the sample size.
Focus group discussion
The study was conducted in 28 focus group discussions, with a minimum of six participants in each group, to access the knowledge of decision-making for SAP prescribing from multiple perspectives across a range of surgical specialties. In circumstances in which a minimum of six participants could not be recruited, semi-structured paired interview was conducted.
Focus group guides based upon the Theoretical Domains Framework (TDF) [21] and the Capability, Opportunity, Motivation and Behaviour (COM-B) model [22] were established and applied in the study. Questions allied to roles and responsibilities for SAP prescribing, factors that influence SAP decision-making, and strategies and resources to facilitate change were convoluted during the discussions. A log was maintained throughout the study process to document all responses and key points raised during the focus group discussion.
Data processing and analysis
The descriptive analysis of the questionnaire was performed using SPSS version 20.0 (IBM Corp, Armonk, NY) to characterize the population parameters and study variables.
For focus group discussion, a thematic approach was taken to analyze the data collected during discussion. The thematic analysis of the data was performed using a programmed approach, using the following steps: (1) familiarization, key themes were constituted around which the data were systematized; (2) tabulation, which includes application of themes to text; (3) charting, or use of headings and subheadings to build a picture of the data as a whole; and (3) mapping and interpretation, in which associations were clarified and explanations worked toward. Independent coding of the data was provided initially by members of the research team, which was then cross-checked to facilitate the development of themes, moving toward an overall interpretation of the data. The phases of thematic analysis [23] were adapted to reflect the utilization of the TDF (a behavior change framework) for the codebook structure and deductive coding.
Data quality assurance
The collected data were checked regularly for clarity, completeness, consistency, accuracy, and validity.
Ethical consideration
Permission was obtained from Jawaharlal Medical College Hospital institutional ethical committee for conducting the study. The process of data collection was started after the objectives of the study were explained to the surgeons and verbal informed consent was obtained from all participants. Participants were also informed that participation was voluntary and that they could withdraw from the study at any stage if they desired and that information was kept confidential.
Results
Twenty-eight focus groups and 16 paired interviews were completed over a period of three months. The average number of participants in each group was six.
Participant characteristics
One-hundred eighty-four participants from surgical specialties or those involved in prescribing SAP were approached. The participants included general surgeons (n = 39; 21%), gynecologists (n = 33; 17.9%), orthopedic surgeons (n = 43; 23.3%), pediatric surgeons (n = 2; 1%), plastic surgeons (n = 6; 3.2%), neurosurgeons (n = 4; 2.1%), otorhinolaryngology (n = 9; 4.9%), and anesthesiologists (n = 48; 26%). Most of the participants were junior residents (136; 73.9%) and on average had 1.84 years of experience (standard deviation [SD] = 0.78) in surgical practice. The analysis of SAP prescribing behavior was categorized into six key themes with supplementary subthemes. These themes were mapped to the relevant TDF and COM-B domains (Table 1).
Themes and Subthemes in Relevant Theoretical Domains Framework and Capability, Opportunity, Motivation and Behaviour Model
COM-B = Capability, Opportunity, Motivation and Behaviour Model; TDF = Theoretical Domains Framework; SAP = surgical antimicrobial prophylaxis.
Theme 1: Solitary focus on surgical skills
Participants noted that multiple factors contribute to the risk of infection. Because most of these factors were considered non-modifiable by the surgeons, prescribing high-end antibiotic agents was considered as the only option (Table 2).
Focus Group Discussion Themes, Subthemes, and Illustrative Quotes
TDF = Theoretical Domains Framework; SAP = surgical antimicrobial prophylaxis; OTs = operation theaters; MDROs = multi-drug–resistant organisma; SSI = surgical site infection; IV = intravensous.
Less preference for SAP
The participants considered the surgical skills and experience of the surgeons as what matters. Most participants in our study did not note any preference to SAP and considered SAP as secondary. They were not concerned about following the standard guidelines for SAP.
Gaps in the knowledge and practice of SAP
On quantitative analysis of the knowledge on SAP (Fig. 1), it was noted that senior residents and junior residents (first year) had the highest scores of approximately 60%. It was noted that the surgeons with more experience had minimum scores. On comparing the scores of various specialties, the surgeons from the department of obstetrics and gynecology were found to have the highest scores followed by the anesthesiologists. Among the six common parameters of surgical prophylaxis that were included in the questionnaire, most of the participants answered correctly regarding the route and the timing of administration of SAP (97.3% and 78.8%, respectively). However, only 35.9% knew about the correct choice of SAP and the duration within which it should be stopped (42.4%). Two-thirds (75%) of the participants answered correctly regarding the assessment of β-lactam allergy before injecting the drug.
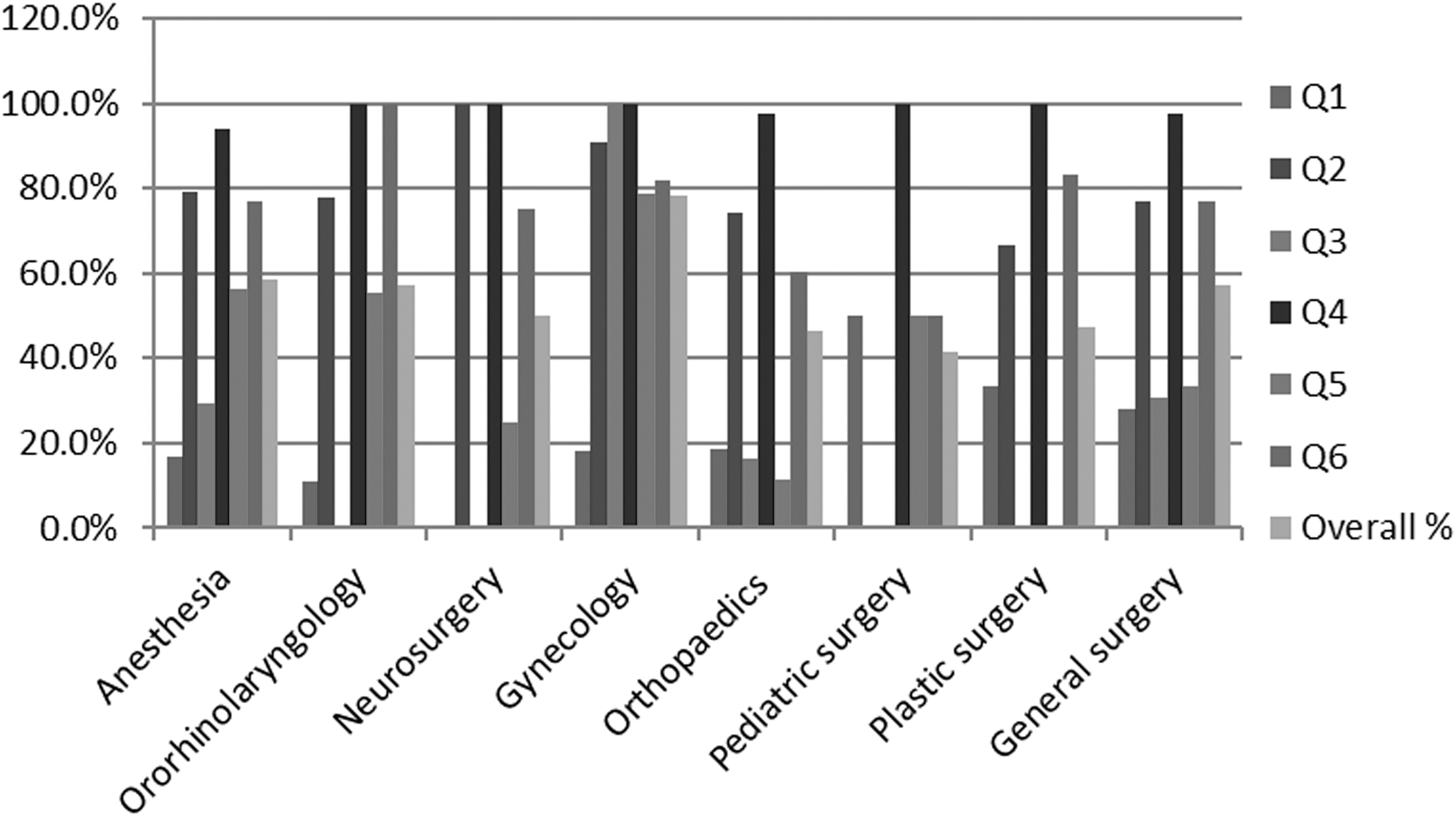
Response to surgical antimicrobial prophylaxis (SAP) questionnaire among different specialties.
Theme 2: Following the hierarchy is more important than guideline compliance
There was a unanimous objection among the residents and junior consultants that despite knowing the guidelines, they were unable to prescribe the desired SAP because the decisions are made at the senior consultant level. Prescribing practices were dependent on the senior consultant's preference irrespective of the guideline recommendations. Surgical antimicrobial prophylaxis decisions were entrenched within hierarchical relationships that are established in hospitals, with decisions inclined by both intra-specialty and inter-specialty grouping and affiliations. Junior doctors considered adhering to decisions made by their seniors as mandatory; not doing so was considered as a risk to interpersonal relationships. Lack of open discussions therefore makes appropriate SAP prescribing difficult in situations in which a consultant makes a decision that is not evidence-based (Table 2).
Theme 3: Doubts and overcautious attitude of surgeons hinder appropriate SAP prescribing
Most of the participants said prescribing broad-spectrum antimicrobial agents and for longer duration was necessary to prevent SSI. Their previous experiences of the patient developing SSI while prescribing SAP according to the guidelines was a clear-cut hindrance in following the desired practice. Orthopedic and plastic surgeons were specifically more likely to prescribe high-end antimicrobial agents as SAP because of the fear of rejection of implants and grafts, respectively.
There was awareness about the development of multi-drug–resistant organisms (MDROs) because of overprescription of antimicrobial agents, but it was overshadowed by the risk of perceived underuse causing direct patient adverse outcomes, particularly SSI (Table 2).
Theme 4: Non-availability of antimicrobial agent in hospital supply
A number of participants who were aware of the SAP prescription practices complained of non-availability of an in-hospital supply of the required antimicrobial agent, which hinders them from providing their patients with the required drugs. Some of the consultants complained that although the drug was available, they prefer standard brands and only then would they prescribe the antimicrobial agents as recommended by the committee. They would not compromise regarding the quality of the product because this may affect the prognosis of their patients (Table 2).
Theme 5: Patient characteristics and type of surgery play a role in prescribing SAP
A consistent concern of most of the participants included in the study was that the patient population is of poor economic status and low socio-economic background, and are unable to bathe for weeks or months before surgery. Additionally, the patients are seen after consuming antimicrobial agents from various local practitioners before coming to the surgeons at the tertiary referral center, thus, the narrow-spectrum agents do not work. Additionally, the type of surgery performed also influences the SAP. Orthopedic and plastic surgeons were concerned about implant and graft rejection if proper prophylaxis is not given. Patients sometimes come with cattle dung applied to their wounds. Hence, whatever infection control precautions are taken, it is ineffectual because as the host is a hub of contamination (plastic surgeon) (Table 2).
Theme 6: Lack of national and local guidelines
The surgeons believe that although guidelines are available, they need guidelines from their own hospital based on the scientific proof. The condition, practices, and patient characteristics are unique to the hospital. Again, patients are seen after consuming antimicrobial agents from various local practitioners before seeing the surgeons at the tertiary referral center, thus, narrow-spectrum agents do not work (Table 2).
Discussion
According to the WHO, of every 100 hospitalized patients at any given time, seven patients in developed and 10 patients in developing countries acquire at least one HCAI. In the developed countries, the most common HCAI is a urinary tract infection whereas among the developing countries SSI is the leading infection HCAI, which affects up to one-third of patients who have had operations. The risk of SSI is up to nine times higher in these settings than in developed countries [24]. In the resource-poor settings, SSIs are involved in one-third of post-operative mortalities and are accountable for 8% of all mortalities resulting from nosocomial infections [25].
The WHO technical consultants led to the adoption of 29 recommendations covering 23 topics for the prevention of SSI in the pre-,intra-, and post-operative periods in 2016 [2]. One of the vital components of the pre-operative bundle is SAP. However, implementation of a proper SAP is a challenge worldwide [26], because it necessitates good familiarity with international and national recommendations and continual evaluations of prophylaxis practice.
This study was undertaken to evaluate knowledge, attitudes, and practices of SAP among the surgeons, analyze the factors that influence SAP decision-making, and the strategies and resources to facilitate change.
We observed in our study that the focus of the participating surgeons was on acquiring high-end surgical skills. Surgical antimicrobial prophylaxis prescription was not considered a priority and therefore there were gaps in the knowledge of SAP as evaluated by the questionnaire.
On quantitative analysis of the knowledge of SAP it was noted that the senior residents and junior residents (first year) had the highest scores whereas surgeons with more experience had lower scores. The first-year junior residents and the senior residents may be updated about SAP knowledge because of regular assessments and because most of the educational interventions target the junior residents. Comparing the scores of various specialties, the surgeons from the department of obstetrics and gynecology were found to have highest scores followed by the anesthesiologists. The department of gynecology had already formulated and disseminated their antimicrobial policy, and this may be the reason that they scored highest. On quantitative analysis of the knowledge, attitudes, and practices of SAP, only 20.1% of participants answered correctly about the indications for SAP. Most of them considered it essential to provide SAP irrespective of the type of surgery. Studies from other developing countries have also reported antibiotic use in 99% of observed surgeries [27].
The most correctly answered questions were the route (97.3%) and timing of administration (78.8%) of SAP. However, only 35.9% knew about the correct choice of SAP and the duration within which it should be stopped (42.4%). Other authors across the developing countries have recounted the use of ceftriaxone or other third-generation cephalosporins for prophylaxis before surgery [28–30]. Broad-spectrum drugs in the surgical setting is reported as a general trend among doctors in developing countries, leading to eventual selection of MDROs, which cause serious post-operative complications [31]. On gap analysis, it was noted that during the regular departmental updates and seminars, rarely were there discussions on antimicrobial policy and practices. Most of the educational activities in the surgical departments focused on surgical skills and techniques.
Most participants highlighted the fact that despite their awareness about the guidelines they were unable to comply with them because of the instructions of senior colleagues. Previous studies have emphasized the role of senior practitioners on antimicrobial prescribing behavior by influencing the juniors and suggested that they would be a crucial cluster to target in interventions that seek to optimize prescribing behavior [32,33]. When trying to shift prescribing behavior, it is important to seek endorsement and involvement from senior surgeons. Change in practice should be expected only after engagement with senior colleagues to certify practitioner buy-in to the development of policy and guidelines and onus of recommendations [34].
A major concern of the surgeons was the fear of adverse patient outcomes, which they considered a matter of reputation among the peers and patients. Previous experiences were a major determining factor for complying with the antibiotic guidelines because all previous adverse outcomes, either correctly or non-correctly, were linked with antibiotic usage. A reason was the fear that most of the surgeons did not have had confidence on the infection control practices of the operation room and the hospital and considered antibiotic agents as a shortcut to the same. Similar to our observation, authors from other studies have reported overprescribing of antibiotic agents as perception of personal accountability and responsibility for patient outcomes, along with culturally determined acceptance of uncertainty as social factors influencing antibiotic use [35]. We recommend that doctors from surgical specialties should be made aware of infection control protocols so as to gain their confidence.
Unavailability or interrupted supply of the antimicrobial agents proposed in the SAP guidelines are a major logistical problem that puts the surgeon in a position to prescribe antimicrobial agents from the limited options available. Influences from pharmaceutical companies such as repeated promotions of the drug and its multiple benefits and offers to surgeons if they choose their brand makes the surgeons unable to distinguish between promotional information and scientific benefits and affects the surgeons' prescribing behavior [36]. This also contributes to the prescribing of a certain company's drug over guidelines suggested by committee. Hence, a barrier is created in following what is required. Therefore, self-regulatory guidelines and legislative checks are required to regulate the relationship between physicians and pharmaceutical industries and their representatives, and prevent the surgeons from being pressured by them [36]. Also, regular audits should be performed to ensure the proper supply of the required drug and its multiple brands in inventory to allow surgeons to choose from available options and determine what is correct for their patients.
Most of the patients who come for surgery are from a low socio-economic background, which creates a poor hygienic environment. Surgeons complained that patients who do not take a pre-operative shower may become a nidus of infection, which puts a stress on the surgeons to prescribe high-end antibiotic agents to prevent infection. In addition, the type of surgery performed also influences the SAP. Plastic and orthopedic surgeons criticized the SAP guidelines for prescribing cefazolin/cefuroxime, because they were more concerned about the prognostic impact of giving narrow-spectrum antibiotics. Fear of failure of surgery and the perception of patient's expectations were the major driving force for prescribing high-end antibiotic agents. The surgeons were not willing to take risk at the cost of losing the doctor–patient relationship.
Participants were aware of national and international guidelines, but generally emphasized the apparent presence of many gaps in the current evidence and how these warranted exceptions to guideline recommendations. These guidelines were considered as general and inadequate to account for the broad range of surgical procedures and any environmental and patient-specific factors, and thus are a barrier to optimal SAP decision-making in complex scenarios.
A common perception among the participating surgeons was lack of evidence-based local guidelines. Given the high rate of inappropriate antibiotic use in low-income countries, and the subsequent high rate of antibiotic resistance, the need for local guidelines based on local susceptibility data is among the more reasonable concerns expressed. Every region has its own characteristic population with varying range of antimicrobial resistance, and thus, requires a policy tailored for implementation in individual hospital.
Changing the behavior of individual prescribers is an important factor while considering implementation of SAP programs. When designing hospital policies for antimicrobial prescribing, it is essential that primary research into the prescribing behavioral intention of individuals is done and that intercessions are customized to the target population in whom behavior change is anticipated. This can lead to an understanding of the barriers to and facilitators of behavior change, enable development of interventions that utilize facilitators and overcome barriers, and promote more sustainable and effective outcomes.
Conclusions
Hospital bureaucrats and institutional quality-improvement departments are required to offer approaches to reduce the antibiotic abuse to improve patient care by minimizing adverse effects, emergence of resistance, and financial burden on both the patient and healthcare system. Departments or units demonstrating higher compliance should be taken as model for implementing the same in other units. The knowledge and attitudes of surgeons toward appropriate SAP prescribing are crucial factors for implementation of guidelines. Including surgeons in policy-making decisions can help in strong execution of the same.
Footnotes
Acknowledgments
We are grateful to the Hospital Infection Control Committee, particularly Mr. Soyab Khan for his valuable inputs.
Funding Information
No funding was received.
Author Disclosure Statement
There were no conflicts of interests.