
Abstract
Background:
Catheter-associated urinary tract infections (CAUTIs) are associated with urinary catheterization. Up to 25% of hospitalized patients may be catheterized during their stay. Urethral catheters are necessary as part of many urologic procedures, but the removal of unnecessary catheters has become more important to reduce infections, healthcare costs, and patient morbidity.
Methods:
Open access data from the U.S. Centers for Disease Control and Prevention (CDC), United States Census, and the American Urological Association (AUA) Census was obtained, and a linear correlation used to determine relations.
Results:
A correlation between the number of urologists per hospital and CAUTIs per hospital was found in both the wards and intensive care units (ICU; p < 0.01). A similar relation was found between the number of urology residencies per hospital and CAUTIs per hospital in the wards (p < 0.01), but this was not significant in the ICU (p = 0.15). The number of urology residencies per state was correlated with the number of urologists per state (p < 0.01). No correlation between state population density and hospital number of CAUTIs, urologists, and urology residencies was found.
Conclusions:
Increased number of urologic procedures and the need for catheterizations likely drives the correlation with urologists and CAUTIs. Despite this, no urologists are on the CDC committee that created CAUTI guidelines. Urologists should be considered for hospital and national committees particularly because they often care for these patients in the outpatient setting.
Catheter-associated urinary tract infections (CAUTIs) are the most common health-care–associated infection reported to the National Healthcare Safety Network (NHSN). During their stay, 15% to 25% of hospitalized patients receive urinary catheters and 75% of in-hospital urinary tract infections (UTIs) are associated with catheters [1]. Foley catheters are often placed peri-operatively for intra-abdominal surgeries to keep the bladder from being distended and inadvertently damaged. They are also placed commonly after urologic procedures for bladder irrigation, tamponade prostate bleeding, or to prevent distention of the bladder that may result in a bladder perforation. Prevention of CAUTIs has become important to prevent prolonged hospital stays, unnecessary patient morbidity, and increased healthcare costs. Increased CAUTI rates can have an adverse effect on patient insurance payments [2]. Many prevention strategies have been attempted, including antibacterial coatings on catheters, peri-urethral cleansing, sealed drainage systems, urinary acidification, and irrigation. However, the best way to avoid a CAUTI is to reduce the use of indwelling urethral catheters as much as possible.
Clean intermittent catheterization (CIC) is used to reduce colonization but can be associated with urethral trauma [3]. Clean intermittent catheterization is also not an option at discharge for a patient who is unable to perform self-catheterization but is still unable to void spontaneously. Indwelling urethral catheters are less time consuming to care for and can be preferred by patients over CIC, despite an increase in bacteriuria [4]. In the acute setting, urologic surgeons may also prefer an indwelling catheter as this would reduce the occasional “difficult catheter” that is not able to be placed despite being performed several times prior. This is often because of urethral false passages and typically seen in males with enlarged prostates [5].
Materials and Methods
Open access data from the U.S. Centers for Disease Control and Prevention (CDC), United States Census, and the American Urologic Association (AUA) census was compiled [6–9]. Linear regression was performed to look for significant relations. P values were obtained to look for a significant correlation using Microsoft Excel Data Analysis Regression Tools (Microsoft, Redmond, WA).
Results
A total of 12,501 practicing urologists were reported in the 2018 AUA census from the United States. A total of 24,684 CAUTIs were reported from 3,654 acute care hospitals to the CDC. A total of 154 urology residencies are in the United States, including military programs. California had the most practicing urologists (n = 1,359) with Wyoming having the least (n = 15). New Hampshire had the highest ratio of urologists to the state population, with one urologist for every 19,378 citizens. Nevada had the lowest ratio of urologists to the state population with one urologist for every 42,144 citizens. New Jersey had the largest number of urologists per acute care hospital at 5.77, with Wyoming having the lowest at 1.07.
New York State had the highest average number of CAUTIs per acute care hospital at 10.82 whereas Wyoming had one CAUTI per hospital in 2018. Several states had no urology residencies, but New York had the most at 21. Vermont had the highest number of urology residencies per hospital at 0.17.
A significant linear correlation (Fig. 1) between the number of urologists per hospital and CAUTIs per hospital was found (p < 0.01). This was important in both the ward and intensive care unit (ICU) beds (p < 0.01). The percent of hospitals with higher ward CAUTI rates were not correlated with the number of urologists in the state (p = 0.18), nor was the percentage of hospitals with lower rates (p = 0.54). The percentage of hospitals with higher ICU CAUTI rates was correlated with the number of urologists per hospital (p = 0.01), but not with the percentage of hospitals with lower than average ICU CAUTI rates (p = 0.5). There was also a correlation between the number of urologists in the state and the population of the state (p < 0.01).

Correlation between number of urologists per hospital and number of catheter-associated urinary tract infections (CAUTIs) per hospital (p < 0.01)
A similar regression was performed looking at the relation between CAUTIs and the number of residencies per hospital (Fig. 2). There was a correlation between ward CAUTIs per hospital (p < 0.01), but no correlation with ICU CAUTIs per hospital (p = 0.15). The percentage of hospitals with higher and lower ward CAUTIs per hospital was not significant (p = 0.18 and p = 0.54, respectively). There was also no correlation between the number of urology residencies per hospital and percentage of hospitals with higher or lower ICU CAUTIs (p = 0.47 and p = 0.51, respectively). The number of urology residencies in the state was correlated to the number of urologists in the state (p < 0.01). A summary of this data is shown in Table 1.
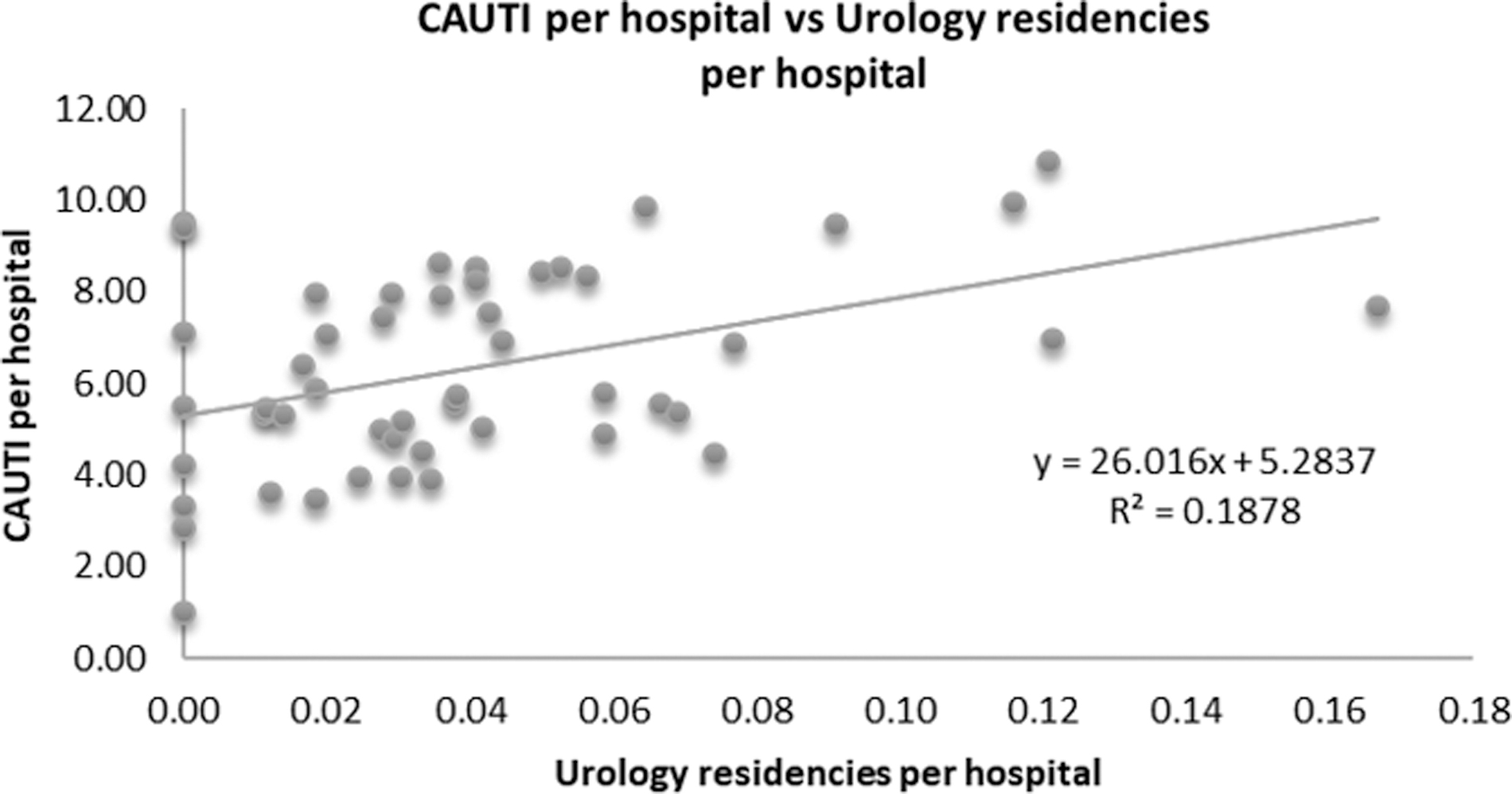
Correlation between the average number of urology residencies per hospital in each state, versus the average number of catheter-associated urinary tract infections (CAUTIs) per hospital (p < 0.01)
Summary of p Values between Average Number of Urologists per Hospital and Average Number of Urology Residencies per Hospital and Their Correlation with Catheter-Associated Urinary Tract Infections
CAUTI = catheter-associated urinary tract infection; ICU = intensive care unit.
The state population density was compared with several other factors. There was no correlation with the number of CAUTIs per hospital (p = 0.41), the number of urologists per hospital (p = 0.85), or the number of urology residencies per hospital (p = 0.89). There was a correlation between population density and the number of acute care hospitals in that state, with more hospitals in areas of higher population density (p = 0.01). A summary of these values is shown in Table 2.
Summary of p Values Comparing State Population Density and Catheter-Associated Urinary Tract Infections, Urologists, and Urology Residencies per Hospital
A correlation was seen between population density and the number of acute care hospitals per state (p < 0.01).
CAUTI = catheter-associated urinary tract infections.
Discussion
State population was correlated with the number of urologists in that state and the number of residencies, with more urology residencies in more populated states. This likely is a consequence of need, as more job opportunities would be present in states with more potential patients. Additionally, urology residencies would require a hospital system that sees many diverse cases, which would necessitate a greater than average amount of urologists to oversee the residents. However, compared with population density, the number of urologists and urology residencies per hospital did not show a significant correlation. This may represent that in densely populated areas a similar number of urologists can care for a larger population than would be expected because of proximity.
Although the amount of acute care hospitals is reported by the CDC NHCN progress report, this does not include the size of these hospitals. Additionally, the ratio of urologists to population may not coincide accurately with the number of urologic services needed in each state because each population may have different rates of hospitalization, nephrolithiasis, urologic oncology, etc. Additionally, a correlation is seen between population density and the average number of hospitals in each state. This may give insight into sizes of hospitals, as rather than densely populated areas containing larger hospitals, this would indicate that these areas add more hospitals instead. Whether this is a function of business competition, land availability, or logistics is not able to be determined from this study.
The correlation with urologists and CAUTIs is likely multifactorial. Although it may be more telling to see CAUTI rates between patients with urologic consultation and those without, no such data exist from the CDC. However, more urologists would indicate that more urologic procedures would be performed. With the increased procedures, likely there would be more urethral catheterizations and subsequent CAUTI. The correlation with urology residencies and CAUTIs was only significant in the wards, but not in the ICU. There is no clear reason for this from the data, but it would be reasonable to infer that hospitals with more urology residencies would also have additional ICU residents and fellows. These may have an increased focus on up to date CAUTI prevention and possibly more rigorous protocols to avoid hospital-acquired infections. Particularly as they also deal with central-line and ventilator-associated infections that are not seen as commonly on the wards [10].
The state that appears to have performed the worst in terms of CAUTIs and CAUTIs per hospital was New York. This is despite having the second most total urologists, percentage of all urologists, and urologists per hospital. It was also the state with the most numerous urology residencies and highest percentage of all urology residencies in the country. Conversely, Wyoming had the lowest number of CAUTIs, percentage of total CAUTIs, and number of CAUTIs per hospital. They had the least number of total urologists, the smallest population, and the least urologists per hospital. They have no urology residencies, but interestingly is forty-third in the number of acute care hospitals. Although these states appear to demonstrate the difference between urban, population-dense states, and rural, low population density states in terms of urologic needs and care, there was no correlation found between population density and number of CAUTIs per hospital. This may indicate more environmental, political, or patient demographic differences that exist in these areas that have an effect on catheterizations and infections.
The prevention of CAUTI is mostly based on the removal of urethral catheters as soon as no longer necessary. The daily increase in bacteriuria is 3%–10%, with nearly all catheters colonized by 30 days [1]. Often CIC is used instead of a Foley catheter because of the decreased amount of bacteriuria [3]. Whereas this may be useful in the patient who can self-catheterize, having this performed in the acute setting requires nursing care several times daily. This would reduce the time nursing has for alternative responsibilities in comparison to an indwelling Foley catheter. The increased incidence of catheterizations can be painful for the patient, particularly if the catheterization technique is not reproducible between nursing providers. This is also true of post-operative patients, such as female hip fracture patients who cannot tolerate repeat positioning for CIC because of pain. Lack of lubrication can lead to false passages in the male urethra making catheterization difficult and potentially causing urethral strictures in the future [11]. In men with enlarged prostates, this can also cause hematuria that may require treatment with continuous bladder irrigation of fulguration. Furthermore, patients who are unable to void spontaneously at discharge would either need to be taught CIC and be supplied with catheters (if able to perform themselves), or have an indwelling catheter placed with outpatient urologic management.
Placement of a suprapubic tube rather than a urethral catheter has been considered in CDC literature as a possible way to reduce CAUTIs. This is inappropriate in non-emergent short-term use as its placement has risks of placement including damage to the bowel, bleeding, and infection. These must be placed by a physician rather than nursing. The data showing the difference in bacteriuria is lacking between suprapubic and urethral catheters, with no apparent difference unless in place longer than five days [12]. This is likely recommended because a suprapubic tube is not considered a reportable CAUTI source, along with straight catheterization, nephrostomy tubes, or ileal conduits [13]. Medications to acidify the urine, such as methenamine, have been considered to reduce CAUTIs. However, most studies have only been performed looking at preventing encrustation in chronically catheterized patients [14]. Although reduction of bacteriuria may be observed, this may not translate to decreased clinical infections. Reducing the amount of urine cultures ordered unless clinical suspicion of UTI should be attempted because there is an association with catheters and asymptomatic bacteriuria that may have no clinical effect on patient care.
The guidelines for CAUTI prevention from the CDC were written by a committee of physicians, epidemiologists, social workers, microbiologists, and nurses. Of the members, 13 of 35 (37%) were infectious disease physicians. No urologists are on the committee despite being the physicians who manage the catheters after discharge from the hospital and commonly treat complicated urinary tract infections in the outpatient setting. With a correlation between urologists and CAUTIs per hospital, there should be consideration given to adding urologists to infection control committees. It is likely that there is an increase in procedures being performed that require longer catheterization at hospitals with more urologists. It is also possible that there is increased urologic consultation for urinary retention, with treatment deviating from hospital protocol by focusing more on preventing genitourinary injuries that may require surgical repair and preparing the patient for outpatient urologic treatment.
Conclusions
There is a correlation between the amount of CAUTIs per acute care hospital and the average number of urologists per hospital. There is also a correlation between urology residencies and the number CAUTIs in the wards, but this was not significant in the ICU setting. Consideration should be given to including urologists on infection control committees to help prevent CAUTIs in the acute care setting.
Footnotes
Funding Information
No funding was received for this project.
Author Disclosure Statement
The authors have no conflict of interest and no competing financial interests exist.