
Abstract
Background:
Vibrio vulnificus is a rare but life-threatening infection that effects the population near warm coastal areas. This infection could be fulminant and rapidly progress to severe sepsis and necrotizing soft tissue infection. Early diagnosis and treatment are critical to saving patients' lives. With multiple studies reporting discrepancies in prognostic factors and different treatment protocols, we aimed through this meta-analysis to assess these factors and protocols and the impact on the outcome of the infection.
Materials and Methods:
In accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, a systematic search of PubMed, Embase, and Cochrane Library databases by two independent reviewers was reported. Studies evaluating prognostic factors and treatment outcomes of Vibrio vulnificus infections were included. Comprehensive Meta-Analysis, version 3.0 was used.
Results:
Two hundred eleven studies were identified. Of those, eight studies met our inclusion criteria. The following factors on presentation were associated with higher mortality rates; concomitant liver disease (odds ratio [OR], 4.38; 95% confidence interval [CI], 2.43–7.87; p < 0.001), renal disease (OR, 3.90; 95% CI, 1.37–11.12; p = 0.011), septic shock (OR, 2.82; 95% CI, 1.84–4.31; p < 0.001), higher Acute Physiology and Chronic Health Evaluation (APACHE) II score (OR, 3.40; 95% CI, 2.26–5.12; p < 0.001), elevated band cells count (OR, 2.61; 95% CI, 1.13–6.0; p = 0.024), hypoalbuminemia (OR, 3.41; 95% CI, 1.58–7.35; p = 0.002), and infection involving multiple limbs (OR, 4.36; 95% CI, 1.72–11.07; p = 0.002). Interestingly, different antibiotic regimens did not have any impact on outcomes, however, delayed surgical intervention after the first 12 or 24 hours was associated with higher mortality rates (OR, 2.64; 95% CI, 1.39–5.0; p = 0.003 and OR, 2.99; 95% CI, 1.54–5.78; p = 0.001, respectively).
Conclusion:
The presence of liver or renal disease, higher APACHE II scores, septic shock, hypoalbuminemia, or elevated band cell on presentation should alert the physician to the higher risk of mortality. Different antibiotic regimens did not impact the outcomes in these patients and delayed surgical intervention is associated with worsening of mortality.
Vibrio vulnificus is a gram-negative motile bacillus that was first isolated in 1964 by the U.S. Centers for Disease Control and Prevention (CDC) [1–3]. It can cause life-threatening infection in high-risk susceptible patients. It thrives in marine and brackish environments, especially in water temperatures from 16°C to 33°C. Therefore, most cases are usually found near coastal areas, and the infection rate tends to be higher in the summer months from April to October [4–6]. Other factors, such as water pH, salinity, turbidity, or pollution appear to have no direct effect [7].
Vibrio vulnificus represents a leading cause of death associated with seafood-related events in the United States [8]. Unlike other old world infections such as Vibrio cholera and malaria, which were introduced to the Americas after 1492, Vibrio vulnificus was recently isolated and classified into three biotypes based on their biochemical characteristics. Biotype 1 is responsible for almost all human infections. Biotype 2 is primarily an eel pathogen. Biotype 3 is limited to Israel and may represent a hybrid between biotypes 1 and 2 [9–12].
Vibrio vulnificus infection is classified into primary septicemia, wound infection, and gastrointestinal illness [2]. Primary septicemia and wound infection types can cause serious complications and manifest clinically as deep soft tissue infection, necrotizing in the majority of cases. On the contrary, the gastrointestinal type is usually self-limited [13,14]. Primary septicemia, which is more common, follows the ingestion of raw seafood (e.g., raw oysters) and mainly affects patients with underlying comorbidities such as liver disease [15,16]. Of note, shellfish such as oysters have a high concentration of Vibrio vulnificus and can be isolated from almost all oysters in the Gulf Coast of the United States at water temperature above 20°C [17]. Wound infection is a less common manner of acquiring the infection such as when a patient is injured in a marine environment or had exposure of a pre-existing wound to seawater [4,18]
Vibrio vulnificus necrotizing fasciitis can be severe and rapidly progress to adverse clinical manifestations and death within 48 to 72 hours from hospital admission. The reported mortality rate is up 71% in cases with septic shock. This may be because Vibrio vulnificus has a relatively short incubation between exposure and onset of symptoms, typically within 24 hours [19]. This rapid course can be explained by the robust ability of Vibrio vulnificus to spread and invade the fascial planes and subcutaneous tissues by the release of several cytotoxins such as metalloproteases, capsular polysaccharides, and cytolysin [20–22].
Patients with underlying chronic diseases such as chronic liver disease, diabetes mellitus, immunosuppression, and hematologic disorders with high serum iron levels are more prone to Vibrio vulnificus infection with a more severe course [23–25]. Additionally, patients presenting with Vibrio vulnificus necrotizing fasciitis and showing signs of septic shock or if their work-up reveals leukopenia, elevated band cell count, low platelet count, and hypoalbuminemia are at higher risk of mortality [26–29]. However, there is no known specific parameter that can detect specifically early Vibrio vulnificus infection [30].
Antibiotic agents and surgery are the key elements in treatment. Antibiotic agents can eliminate the infection in well-perfused tissues and thus limit the spread of the infection [31,32]. There are different antibiotic regimens for Vibrio vulnificus. The CDC recommends intravenous third-generation cephalosporin plus oral or intravenous doxycycline against Vibrio vulnificus, which is more effective than monotherapy. Quinolones also have similar efficacy against Vibrio vulnificus. However, clinical data about the effectiveness of antibiotic agents in Vibrio vulnificus are lacking [33]. Surgical intervention in a timely manner, including debridement, fasciotomy, or amputation has an impact on improving the survival rate among patients with severe necrotizing infections because antibiotic agents cannot reach therapeutic levels within necrotic tissues [34,35].
The majority of Vibrio vulnificus cases were reported as case reports with a few studies reporting different factors associated with mortality. We conducted our meta-analysis to assess and clarify different factors associated with mortality and the impact of different antibiotic regimens as well as surgical intervention and its timing on the course of the infection.
Materials and Methods
Literature search
We followed the Conducting Systematic Reviews and Meta-Analyses of Observational Studies of Etiology (COSMOS-E) guidelines during the preparation of the current meta-analysis. Systematic literature searches in PubMed, Cochrane Library, and Embase were conducted by two reviewers (A.E. and A.A.). The following keywords were used (“Vibrio necrotizing,” “Vibrio sepsis,” “Vibrio infection”).
Inclusion and exclusion criteria
Articles were included if they focused primarily on Vibrio vulnificus sepsis and soft tissue infection and those studies in which each potential prognostic factor and treatment modality was assessed in relation to mortality. We excluded review articles, conference articles, editorial letters, case reports, or comments, non-English studies, studies with insufficient data, non-human studies, and studies with an overlapping patient population.
Data extraction
Data were extracted independently by two reviewers (A.E. and A.A.). They examined and selected all potentially eligible articles in two steps: the first step was to screen titles/abstracts for matching our inclusion criteria; duplicates were removed. The second step was to screen the retrieved full-text articles for eligibility for meta-analysis. Discrepancies in outcome extraction were resolved by re-examination of the relevant study until consensus was achieved. Disagreements were resolved by discussion with a third reviewer (M.A.).
The following information was extracted on a standardized form: name of the first author, year of publication, ethnicity and location of the study population, study design, and total sample size; demographic data (age, gender); mode of infection (history of injury and/or wound or sea food consumption); comorbidities (diabetes mellitus, liver disease, end-stage renal disease, heavy alcohol use, malignancy and immunosuppression); clinical presentation of Vibrio vulnificus infection on admission (Acute Physiology and Chronic Health Evaluation [APACHE] II score, presence of fever, septic shock, hemorrhagic bullae, location and distribution of lesions); laboratory findings (white blood cell counts, band cell count, hemoglobin, albumin, creatinine, and bacteremia); therapeutic modalities (surgical treatment such as debridement, fasciotomy, amputation, antibiotic regimens such as penicillin or cephalosporin monotherapy, third-generation cephalosporin/minocycline, and quinolones/minocycline, length of hospital stay, and duration of intensive care unit admission; and time between admission and surgical intervention. We performed the analysis with cutoff values of 12 and 24 hours.
Quality assessment
The Newcastle-Ottawa scale (NOS) was used to assess the quality of non-randomized studies. The NOS consists of three quality parameters: selection, comparability, and outcome. The total assessment scale ranged from zero (worst) to nine (best). Articles with scores of two or less were designated as low quality, whereas those with scores of six or more were designated as high quality.
Statistical analysis
Data were analyzed using Comprehensive Meta-Analysis, version 3.0. For dichotomous scales, the effect size was pooled and expressed as odds ratio (OR) along with a 95% confidence interval (CI), whereas continuous data were analyzed by standardized mean difference (SMD) then converted to odds ratio for easy interpretation. A fixed-effects model was applied. Heterogeneity was examined by Cochrane Q and I2 statistic. Publication bias was assessed using a funnel plot for precision and Egger regression intercept.
Results
Literature search and quality of reviewed studies
A flowchart describing the systematic review search results is depicted in Figure 1. The search yielded 2,262 records. After screening by the titles and abstracts, 211 full-text publications were assessed for eligibility.
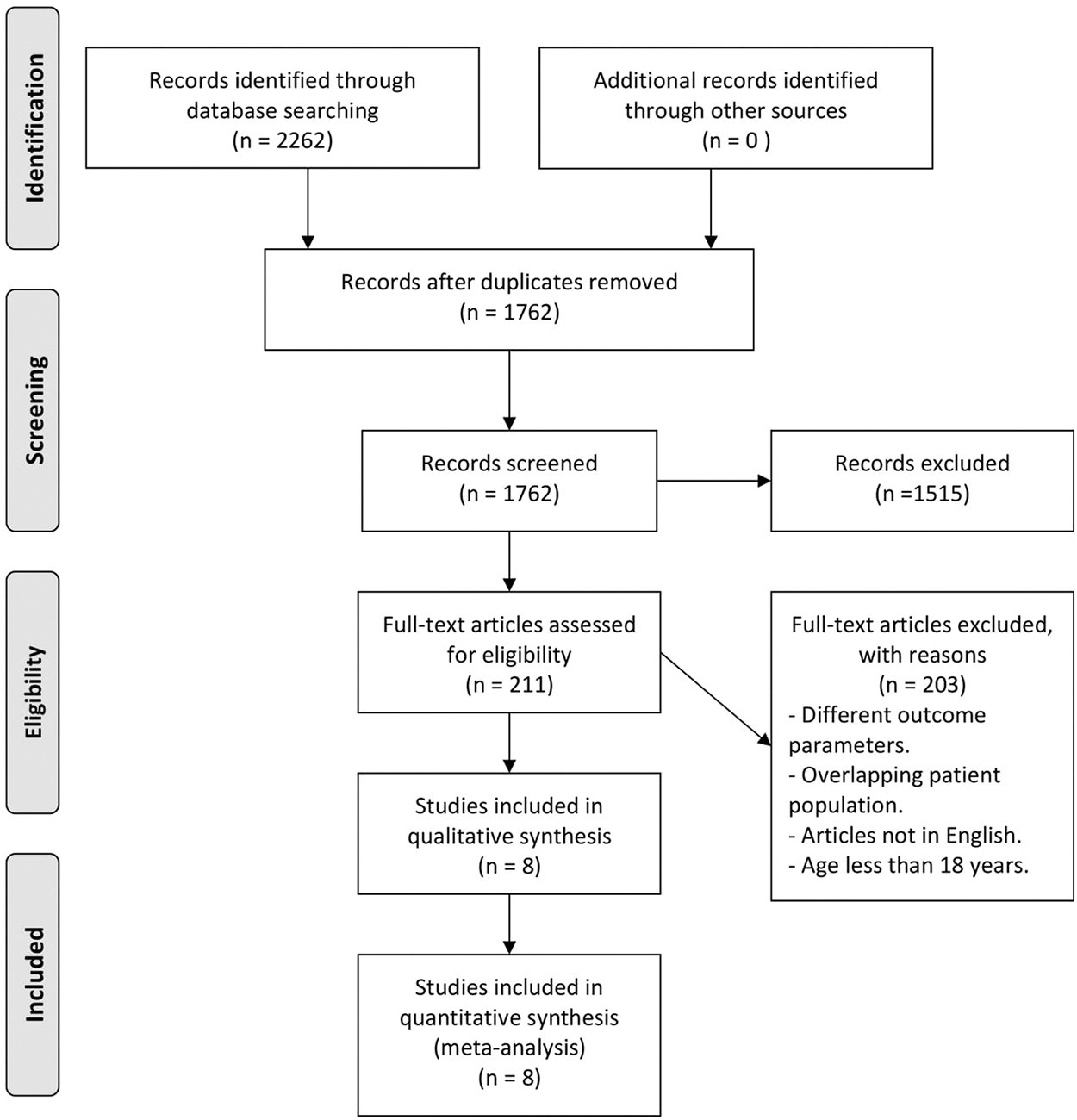
Workflow of literature search and study selection.
Eight studies with a total of 540 patients with Vibrio vulnificus (420 males and 120 females) were enrolled for quantitative assessment, as shown in Table 1. After Vibrio infection, 230 patients died (mortality rate, 42.6%). All eligible studies were performed retrospectively and published in the period between 1980 and 2019. Other than one study in the United States, all study populations were from Asia. The quality score of studies included ranged from six to seven, as assessed by the NOS scale.
Characteristics of the Selected Articles
Data presented as a percentage or mean ± standard deviation. Data extracted in median (quartiles) were converted into mean and standard deviation.
Quality score was assessed by NewCastle-Ottawa scale (NOS).
Retro = retrospective cohort study.
Pooled estimates of associated factors and heterogeneity assessment
Overall pooled estimates for age and gender did not reveal any significant association with mortality (OR, 1.03; 95% CI; 0.74–1.44; p = 0.84) and (OR, 0.91; 95% CI, 0.56–1.47; p = 0.71), respectively (Fig. 2). All studies were homogenous for age comparison (p = 0.15; I2 = 0%) and minimally heterogeneous in gender (p = 0.12; I2 = 40.5%).

Association of patients' demographic data with mortality, age
Comparing the two groups based on the associated risk factors and comorbidities revealed that modes of acquiring the infection or wound infection or history of seafood consumption did not have significant impact on survival rates (OR, 1.92; 95% CI, 0.33–10.97; p = 0.46 and OR, 1.54; 95% CI, 0.67–3.61, p = 0.31, respectively).
Having chronic liver disease was associated with mortality (OR, 4.38; 95% CI, 2.43–7.87; p < 0.001). Pooled studies were homogenous (p = 0.53; I2 = 0%). Similarly, having chronic renal disease was associated with mortality (OR, 3.90; 95% CI, 1.37–11.12; p = 0.011). However, this pooled estimate was extracted from two studies with substantial heterogeneity (p = 0.09; I2 = 64.6%). In contrast, having the following comorbidities was not associated with higher rates of mortality: diabetes mellitus (OR, 0.78; 95% CI, 0.47–1.3; p = 0.33), malignancy (OR, 1.76; 95% CI, 0.56–5.53; p = 0.33), immunosuppression (OR, 0.68; 95% CI, 0.30–1.52; p = 0.34), and heavy alcohol use (OR, 1.18; 95% CI, 0.54–2.58; p = 0.67) as shown in Figure 3.
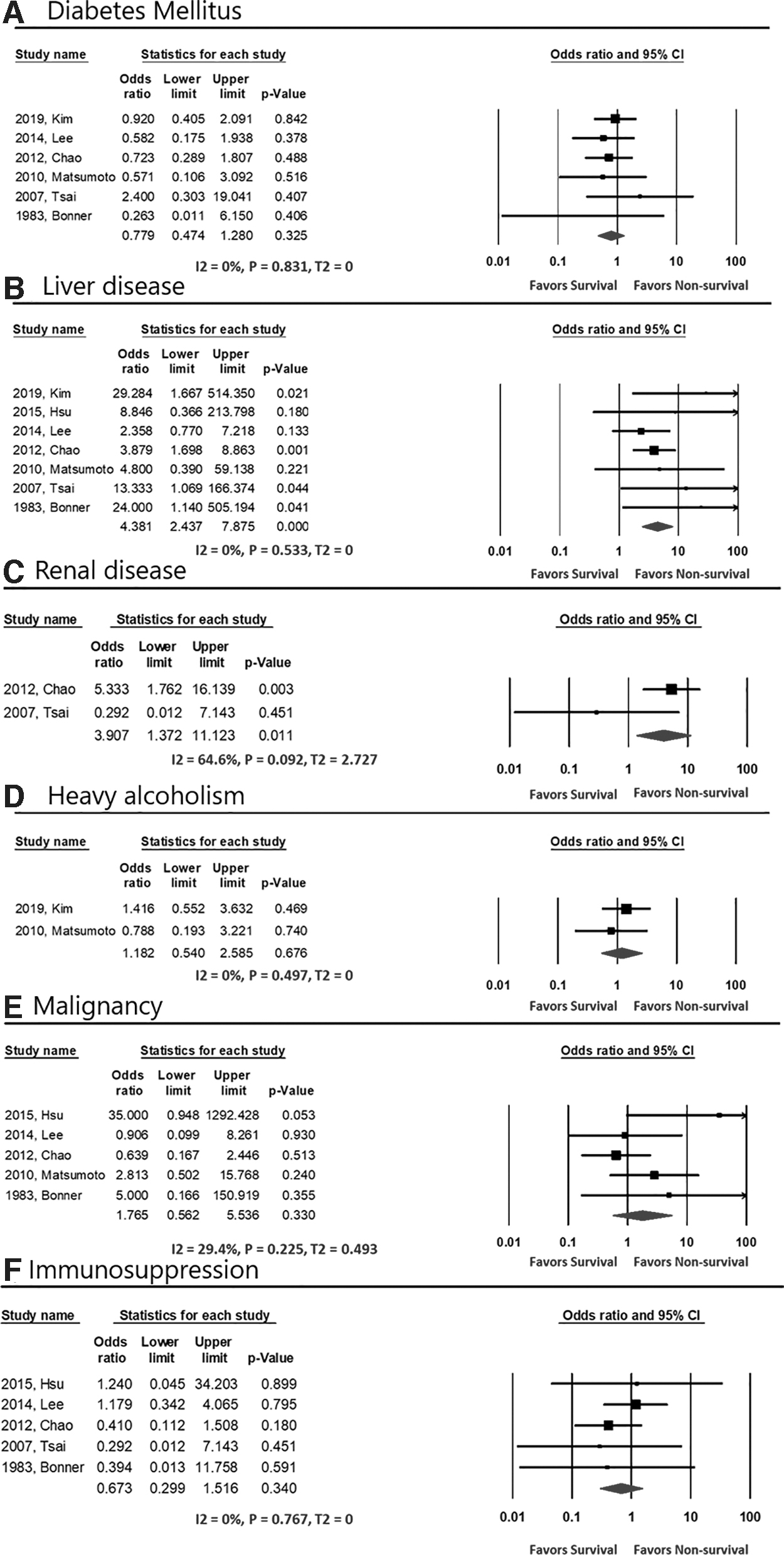
Associated risk factors and comorbidities with mortality, Diabetes Mellitus
Additionally, our analysis showed that patients presented with lesions involving multiple extremities had higher odds of mortality (OR, 4.36; 95% CI, 1.72–11.07; p = 0.002). All studies were homogenous (p > 0.1). However, there was no difference in mortality between upper and lower limb involvement (OR, 2.47; 95% CI, 0.91–6.67; p = 0.07). Patients who presented with septic shock and higher APACHE II score were substantially associated with mortality (OR, 2.82; 95% CI, 1.84–4.31; p < 0.001 and OR, 3.40; 95% CI, 2.26–5.12; p < 0.001, respectively). The presence of fever and hemorrhagic bullae was not associated with higher mortality (OR, 0.77; 95% CI, 0.43–1.41; p = 0.40 and OR, 1.57; 95% CI, 0.64– 3.8; p = 0.32, respectively) as shown in Figure 4. The APACHE II score cutoff value ≥18.5 revealed substantial mortality risk (OR, 2.68; 95% CI, 1.57–4.58; p < 0.000).
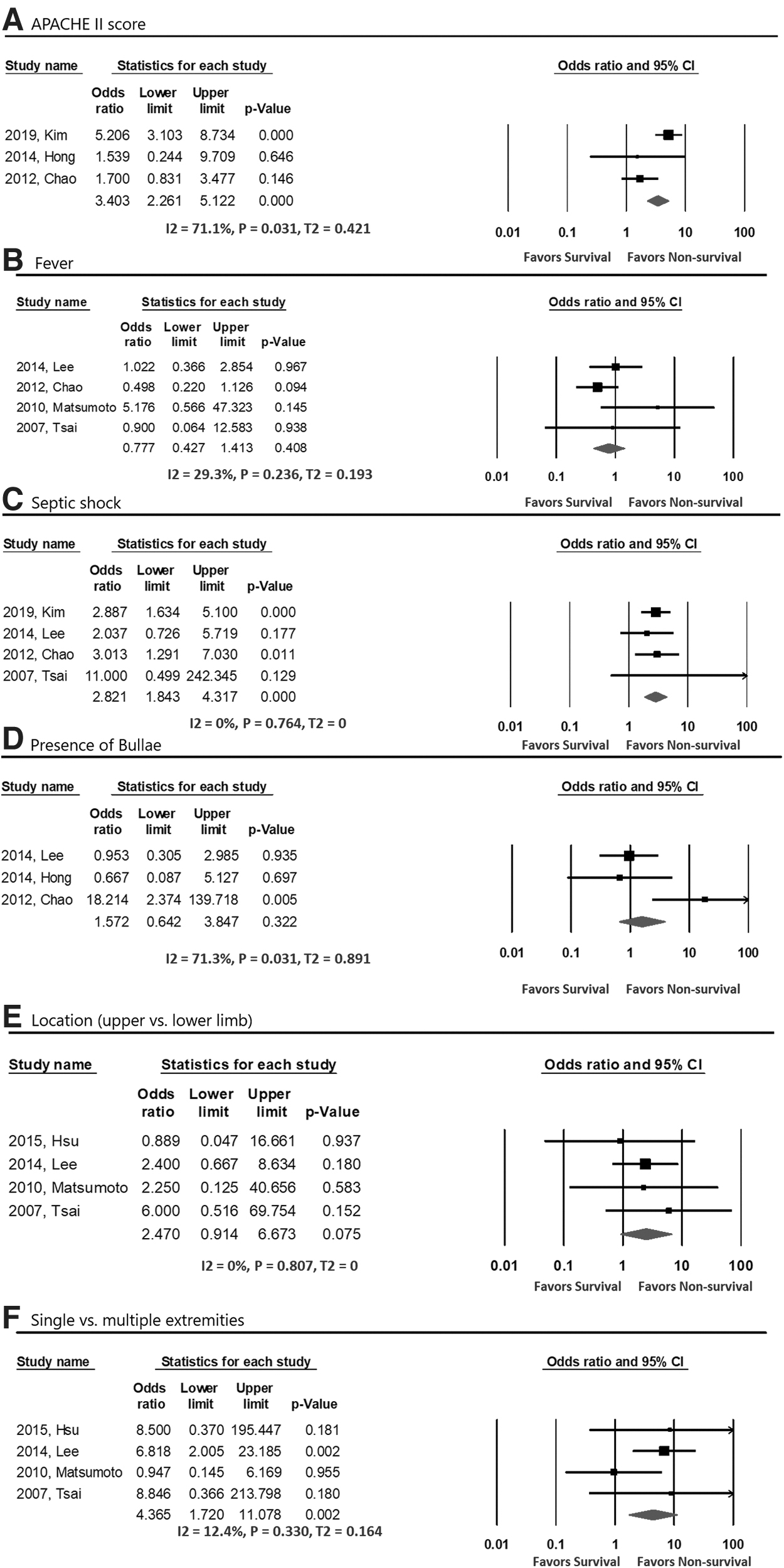
Association between signs and symptoms on admission with mortality, APACHE II score
Pooled estimates of laboratory findings showed that patients with increased band cells and low albumin level were positively associated with mortality (OR, 2.61; 95% CI, 1.13–6.0; p = 0.024 and OR, 3.41; 95% CI, 1.58–7.35; p = 0.002, respectively). However, elevated white blood cell count, high creatinine levels, and presence of bacteremia were not positively associated with mortality (OR, 0.47; 95% CI, 0.17–1.29; p = 0.14; OR, 1.81; 95% CI, 0.92–3.55; p = 0.08; and OR, 2.06; 95% CI, 0.76–5.60; p = 0.15, respectively) as shown in Figure 5. Albumin level at cutoff value ≤2.08 g/dL carried three times more risk of mortality (OR, 3.28; 95% CI, 1.33–8.10; p = 0.010).
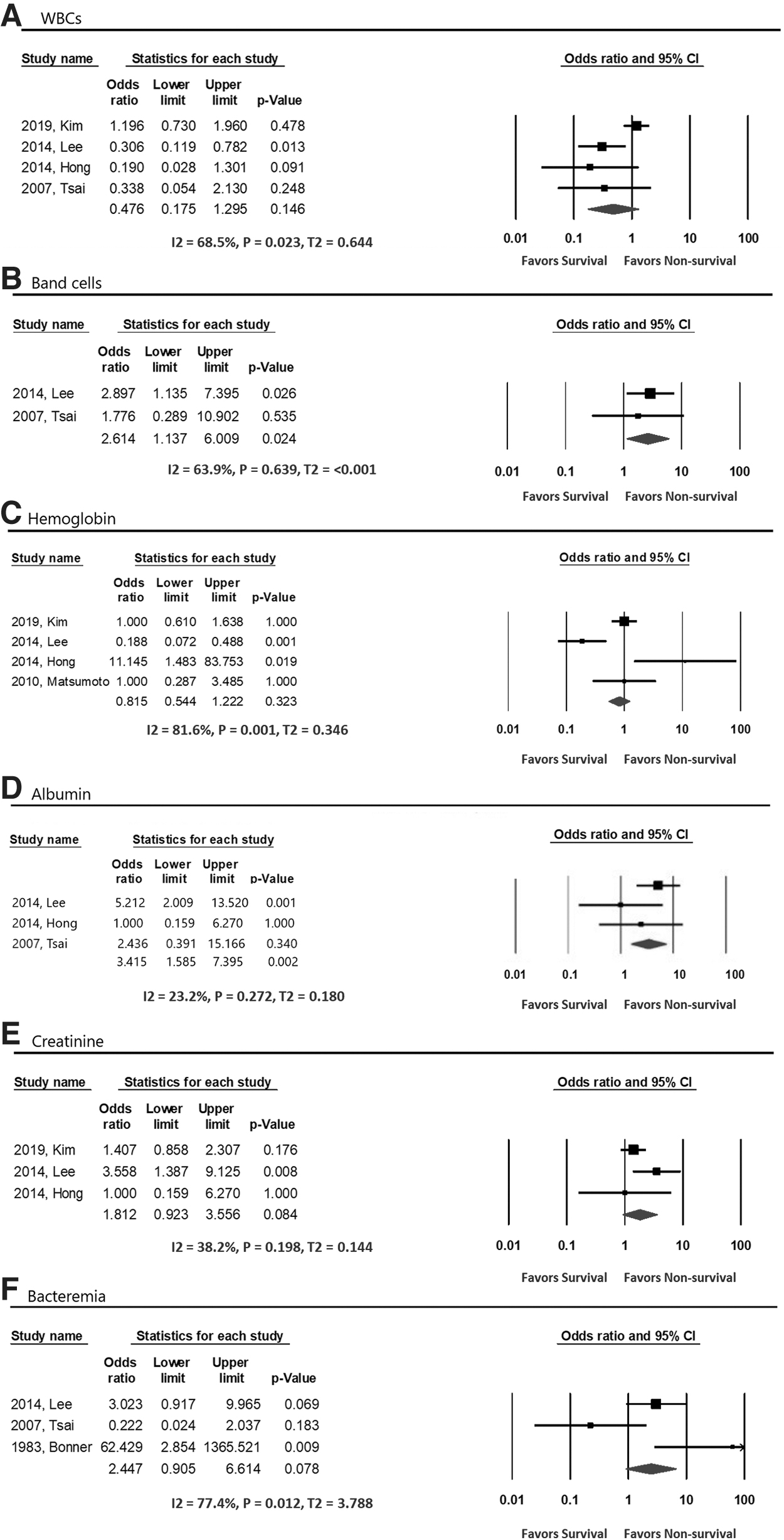
Association of laboratory findings with mortality, WBCs
Analysis of different therapeutic modalities showed the following. Antibiotic regimens of any of the following groups (penicillin or cephalosporin monotherapy, third-generation cephalosporin with or without minocycline, or quinolones with or without minocycline) did not affect outcomes (OR, 1.36; 95% CI, 0.81–2.29; p = 0.24; OR, 1.18; 95% CI, 0.35–3.96; p = 0.77; and OR, 0.84; 95% CI, 0.21–3.5; p = 0.81, respectively). Among surgical procedures, fasciotomy showed 74.2% reduction of mortality (OR, 0.25; 95% CI, 0.08–0.82; p = 0.022) as shown in Figure 6. Additionally, patients with prolonged hospital stay had higher odds of mortality (OR, 2.25; 95% CI, 1.23–4.09; p = 0.008).
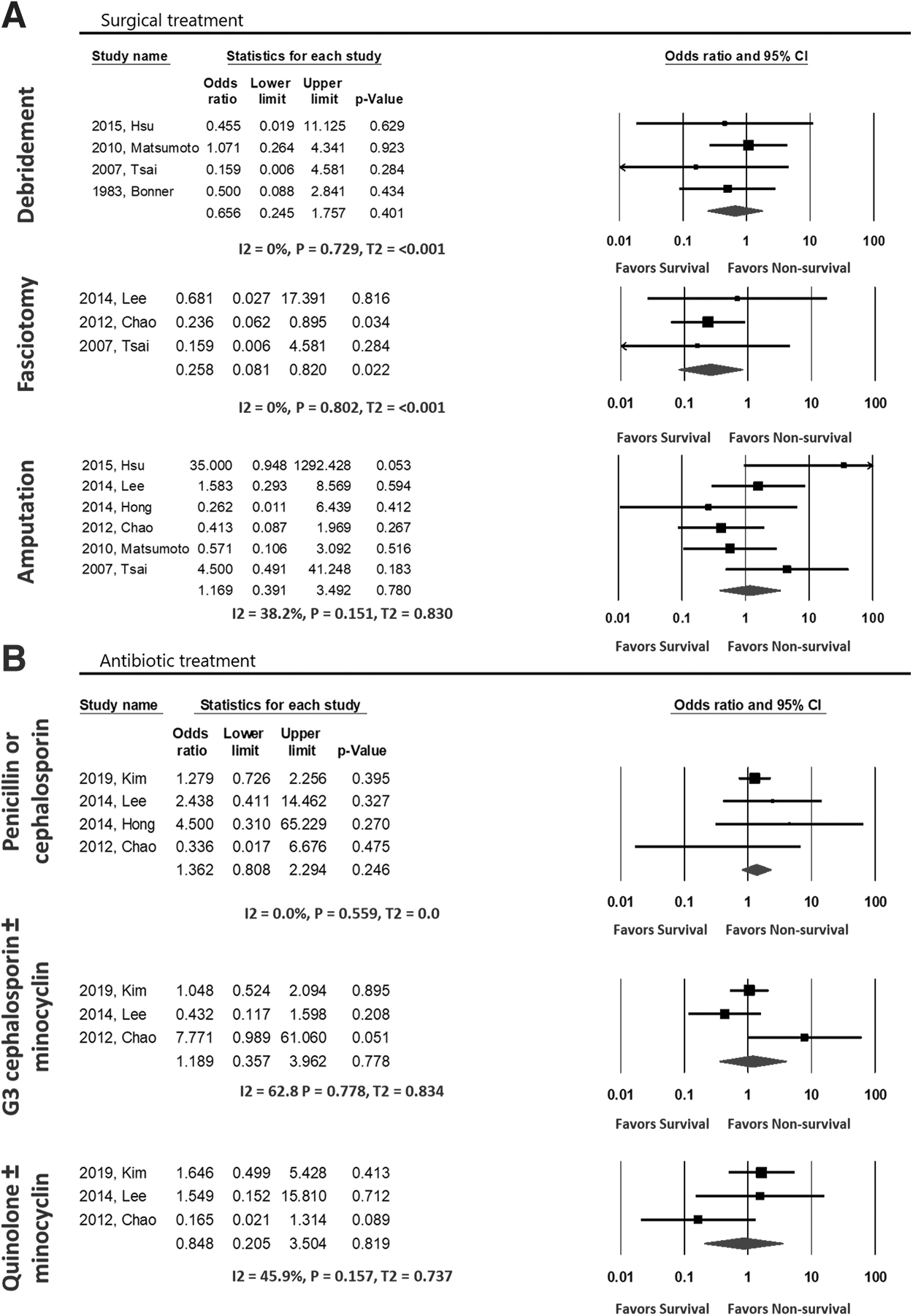
Association of treatment modalities with mortality, surgical treatment
As depicted in Figure 7, delayed surgical intervention was associated with higher odds of mortality; patients who underwent surgical intervention after 24 hours showed approximately three times more risk of in-patient mortality compared with those with earlier intervention within 24 hours (OR, 2.99; 95% CI, 1.54–5.78; p = 0.001) and were more than three times more likely to die compared with those who received treatment within the first 12 hours (OR, 3.72; 95% CI, 1.78–7.76; p < 0.001). Additionally, higher odds of mortality were significant in those who received surgical intervention after 12 hours of admission compared with the first 12 hours (OR, 2.64; 95% CI, 1.39–5.0; p = 0.003). Thus, from our comparisons, surgical treatment within 12 hours of admission showed the best outcomes.
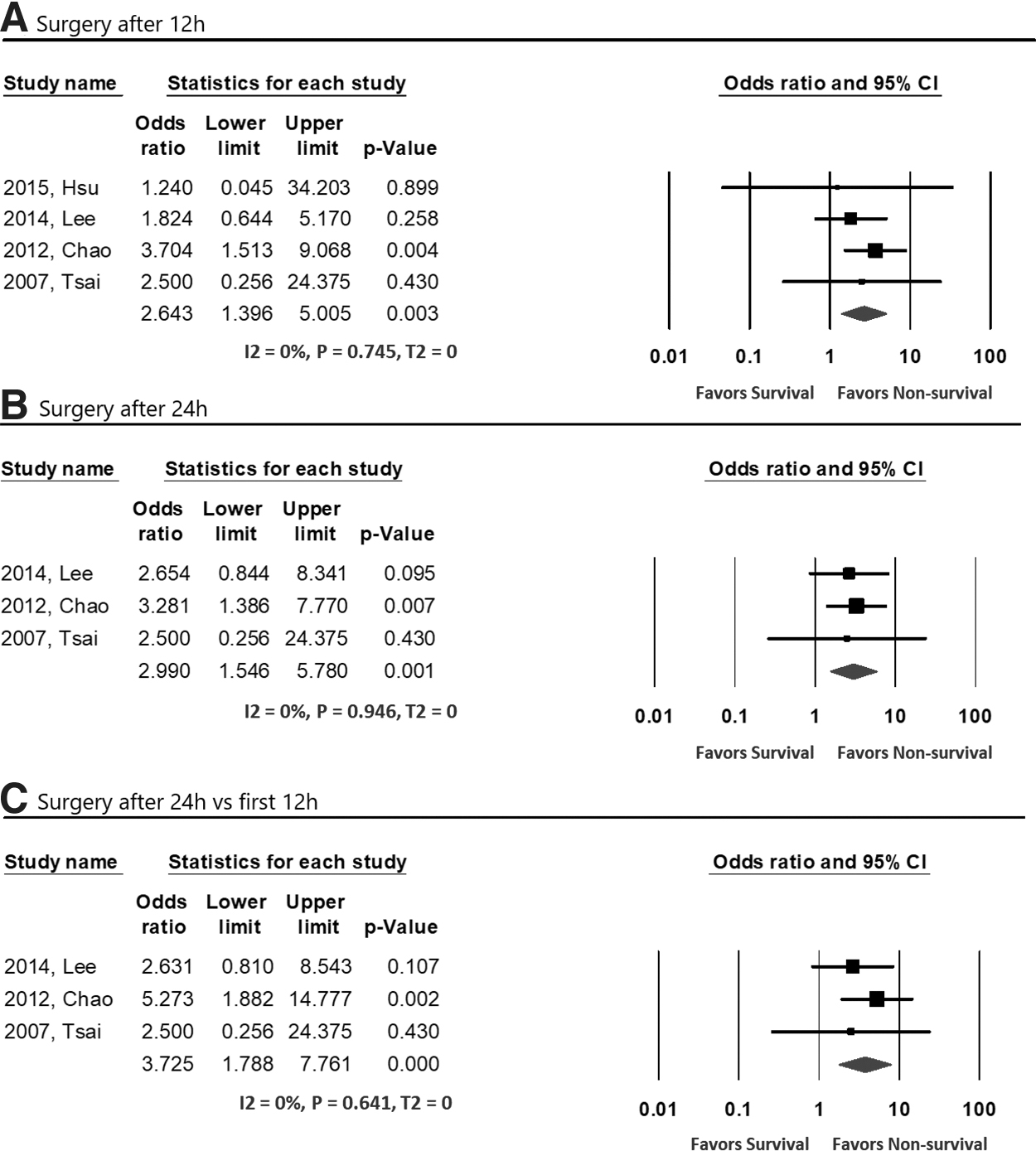
Association of timing of surgical intervention with mortality, surgery after 12 hours
Discussion
Vibrio vulnificus is a fatal infection with a higher incidence in marine-related environments accounting for almost 95% of all deaths in the United States related to seafood consumption rendering it the most fatal food-borne bacteria [41,42]. For prevention of Vibrio vulnificus infection, the CDC recommends wearing protective clothing such as gloves, gowns, laboratory coats, and protective footwear when handling raw shellfish or walking through warm or brackish sea water [43]. Unfortunately, there is no approved vaccine against Vibrio vulnificus [44].
The exact reason behind the increasing incidence of the infection in the United States is not known, however, it could be because of climate change, global warming, and an extended infection season [45]. With increased water temperature and sea level rise, water can extend to more areas altering the ecological range of many bacteria, including Vibrio vulnificus [46]. Early identification and prompt treatment are crucial for survival. With the absence of clear prognostic factors treatment may be delayed when it is needed most, especially in high-risk patients. Although recent studies reported that polymerase chain reaction testing is accurate and fast in confirming Vibrio vulnificus compared with routine cultures, the rapidly lethal nature of the infection renders clinical suspicion and active intervention the mainstay of management [47].
To our knowledge, this is the first meta-analysis to identify the prognostic factors associated with mortality in patients with Vibrio vulnificus sepsis and soft tissue infection. Our study showed that chronic liver disease is associated with four times higher mortality risk. Patients with chronic liver disease, including cirrhosis and hepatitis, are typically more prone to the infection and tend to have a worse prognosis [25,48]. This may be explained by impaired phagocytic function and the presence of arteriovenous shunts allowing bacterial invasion to the systemic circulation, along with complement deficiencies and abnormally high serum iron, which is essential to the growth of Vibrio vulnificus [39]. Additionally, end-stage renal disease was also associated with four times more risk of mortality. However, elevated serum creatinine levels did not reflect a significant association with mortality. Although diabetes mellitus, immunosuppression, malignancy, and heavy alcohol use are known risk factors favoring the infection [43], they did not show a significant impact on mortality in our results, which is consistent with Yao et al. [30].
In this meta-analysis, patients with higher APACHE II score on admission were four times more likely to face a fatal outcome; specifically, APACHE II score higher than 18.5 as a significant cutoff value that is lower than 20 as a cutoff value suggested by Chen et al. [49]. This finding is supported by data from previous studies [50–52]. Several previous articles recommended its use as a prognostic factor in soft tissue infections by Vibrio vulnificus [49,53].
Our analysis showed that the involvement of more than one extremity with necrotizing lesions is an independent factor for mortality. Soft tissue involvement was much more common in the lower limbs. However, no differential impact was found in our study whether the involvement was of the upper limbs or lower limbs, consistent with Tsai et al. [29].
Previous studies reported that patients with hypotensive shock, low platelet count, hypoalbuminemia, leukopenia, and elevated band cell count are at higher risk of mortality [30,54]. In this meta-analysis, septic shock on admission was a significant factor for mortality, consistent with previous studies [14,50]. Additionally, on admission, patients with elevated band cells and low albumin levels were at higher risk of mortality. Albumin is a negative acute-phase protein, and low levels can be caused by liver disease, renal disease, sepsis, or malnutrition, however, the differentiation depends mainly on the clinical picture [55]. Elevated white blood cells, elevated creatinine levels, or low hemoglobin levels did not have an observable impact on mortality, which is also consistent with Nakafusa et al. [14].
The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score was developed as a tool for diagnosing necrotizing fasciitis. It consists of six laboratory tests: white blood cell count, hemoglobin, sodium, glucose, creatinine, and C-reactive protein. The LRINEC score showed good results initially, however, recent studies showed low sensitivity in diagnosing necrotizing fasciitis. Hsiao et al. [56] included 19 patients with Vibrio vulnificus necrotizing fasciitis and reported that they had lower LRINEC scores than patients with other bacteria, suggesting that the LRINEC score can be different according to the causative organism and its clinical picture.
Different antibiotic agents are effective against Vibrio vulnificus, limiting the spread of the infection into the blood and further soft tissue involvement [33,34]. However, extensive necrosis and diminished vascularity with thrombosed blood vessels limit the ability of the antibiotic agents to reach effective levels in the infected tissue. Our findings remain consistent with this conclusion. Three groups of the most commonly used antibiotic agents among the studies included in our meta-analysis (penicillin or cephalosporin alone, third-generation cephalosporin plus minocycline, and quinolones plus minocycline) did not have an impact on patient survival. It is also important to note that patients who received antibiotic agents alone without surgical intervention had worse outcomes [33,49]. This emphasizes the importance of early surgery in the management of soft tissue infections caused by Vibrio vulnificus.
Most recent studies on Vibrio vulnificus soft tissue infections and necrotizing fasciitis report better survival with surgical intervention in the first 24 hours [21,49,57]. Our meta-analysis is consistent with these results, with a threefold reduction in mortality when surgery is performed in the first 24 hours. Moreover, surgery in the first 12 hours after admission confers a reduction in mortality risk of 2.6 times. This finding is consistent with previous studies [34,35]. Although there was no observed difference between surgical intervention in the first 12 hours and the following 12 hours on survival, our data points to the importance of early surgical intervention.
Although some studies focused on the importance of early diagnosis and aggressive surgical debridement to have a favorable outcome [58,59], other studies showed that early less invasive surgical interventions such as simple incision or fasciotomy followed by later definitive surgery have a greater impact on survival [35]. Our meta-analysis findings are consistent with the latter findings wherein early fasciotomy followed by later definitive surgical management improved the survival rate. However, to what extent fasciotomy is done and the degree of associated debridement during fasciotomy was not clear among the included studies. Additionally, debridement or amputation did not positively impact survival, although it can be indicated at a point during the course of the infection. However, whether to do simple incision or fasciotomy followed by definitive surgery or early aggressive surgery from the beginning remains a question for future studies.
Limitations
All the studies included in this meta-analysis were retrospective studies, which may be because the nature of the infection is rare with rapid course. Future studies done prospectively may provide more insight, despite the uncommon occurrence of Vibrio vulnificus infection in humans.
Conclusion
Vibrio vulnificus infection is fatal with very poor outcomes. Septic shock and necrotizing fasciitis develop rapidly; in this meta-analysis, the mortality rate was 40%. Through our study, we were able to establish high APACHE II scores, septic shock on presentation, soft-tissue involvement of multiple limbs, liver disease, renal disease, hypoalbuminemia, and a high count of band cells as predictors of mortality in Vibrio vulnificus infection. Early surgical intervention (preferably within the first 12 hours) is extremely important for survival. Different antibiotic regimens did not have an impact on survival. With these findings, we hope to provide some insight into the factors that physicians should be aware of when dealing with Vibrio vulnificus infection.
Footnotes
Authors' Contributions
Study design: Elnahla, Nichols, Toraih, Kandil. Search and data abstraction: Elnahla, Attia, Akkera. Statistical analyses: Toraih. Data interpretation: Elnahla, Attia, Toraih, Nichols, Kandil. First draft: Elnahla. Final draft: Kandil, Nichols, Guidry, Schroll, Killackey. Critical review and approval of final version: All authors.
Funding Information
This research did not receive any specific grant from sponsors or funders.
Author Disclosure Statement
No competing financial interests exist.