
Abstract
Background:
Gas-forming pyogenic liver abscess (GFPLA) accounts for up to 30% of all pyogenic liver abscess (PLA) cases. However, little is known of the differences in clinical features and prognosis between GFPLA and non-GFPLA.
Aim:
This retrospective study compared the clinical features and prognosis of GFPLA and non-GFPLA.
Patients and Methods:
Data for 392 patients with PLA treated from January 1, 2007 to December 31, 2016 were reviewed. Gas-forming pyogenic liver abscess was defined as gas in the abscess. Liver abscesses were considered non-GFPLA (n = 326) or GFPLA (n = 66). The clinical features and outcomes of patients with GFPLA were compared with that of patients without GFPLA.
Results:
The groups were similar in gender ratio, age, smoking, drinking, and comorbidities. Klebsiella pneumoniae was the most common pathogenic bacteria, but the negative rate of bacterial culture of the non-GFPLA group was higher than that of the GFPLA. In etiologies, the GFPLA group had more biliary source infection and less cryptogenic infection. In addition, the GFPLA group had a higher rate of previous hepatobiliary surgery, especially biliary enteric anastomosis. Compared with the non-GFPLA group, the percentage of the GFPLA group with antibiotic agents combined with percutaneous drainage was higher, whereas the percentages given antibiotic agents alone and antibiotic agents combined with surgical drainage were lower. Patients with GFPLA had higher rates of sepsis and pleural effusion, and longer hospital stays than did non-GFPLA patients. No patient died during hospitalization.
Conclusions:
The GFPLA group had more biliary source infection and less cryptogenic infection in etiologies. Gas-forming pyogenic liver abscess is associated with past hepatobiliary surgery, especially biliary enteric anastomosis and has high rates of sepsis and long hospitalization. Thus, the patients with PLA with a history of hepatobiliary surgery should be monitored more closely in the early stage of the PLA. It needs to be recognized as a distinct clinical entity.
Pyogenic liver abscess (PLA) is a common infectious disease of the liver, accounting for 80% of all liver abscesses [1]. Compared with the United States and Europe, the rate of incidence of PLA is higher in Asia, specifically approximately 17.6 per 100,000 in Taiwan and 1.1–3.6 per 100,000 in mainland China [1,2]. The difference in incidence of PLA may be because of the differences in risk factors for PLA, including the prevalence of hepatobiliary disease such as cholangitis [3]. The incidence of PLA has increased steadily in recent years, because it is associated with diabetes mellitus, an aging population, increasingly aggressive surgical management of hepatic, biliary, and pancreatic disorders, and the wide use of immunosuppressive agents in patients with transplant and cancer [4]. Gas-forming PLA, that is with gas in the abscess based on ultrasound or computed tomography (CT) imaging data (Fig. 1), may constitute as much as 30% of PLA cases [5].
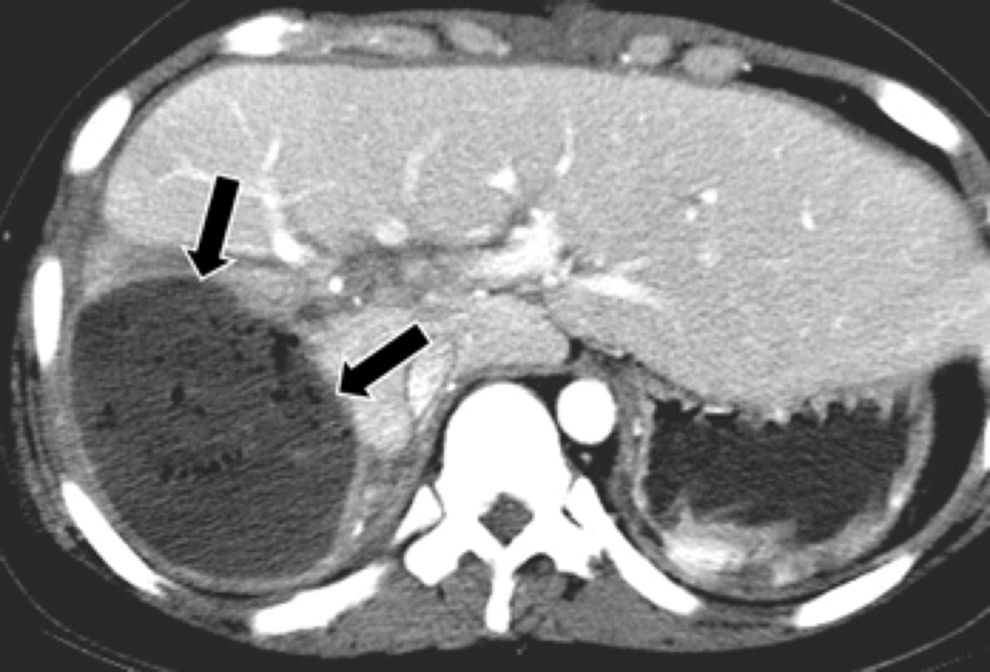
Abdominal computed tomography (CT) findings of gas-forming pyogenic liver abscess (GFPLA). Arrows = GFPLA.
Gas-forming pyogenic liver abscess was first reported by Smith [6] in 1944. Patients with GFPLA have a high risk of mortality, and because of this it has gained attention [5]. The most common pathogen associated with PLA is Klebsiella pneumoniae, a gram-negative rod-shaped bacterium with a high rate of fatality [7]. In patients with diabetes, for example, the high glucose levels may provide gas-forming micro-organisms with a favorable environment for forming gas through mixed acid fermentation. In an acidic environment (pH <6), mixed acid is metabolized by formic hydrogenlyase, resulting in gas formation [8]. Moreover, the microangiopathy associated with diabetes markedly impairs transport of catabolic end products (i.e., gas) away from the lesion, and thereby results in gas accumulation [9,10].
However, few reports of PLA have focused on the differences in clinical features and prognoses of patients with or without gas-forming abscesses (GFPLA and non-GFPLA, respectively). This retrospective study compared the clinical features and prognoses of patients with GFPLA or non-GFPLA in our hospital.
Patients and Methods
This study was approved by the Ethics Committee of First Affiliated Hospital of Xi'an Jiaotong University (No: XJTU1AF2015LSL-057). The need for patient's informed written consent was waived because of the retrospective nature of the study.
Study population
A total of 438 patients with PLA were admitted to First Affiliated Hospital of Xi'an Jiaotong University from January 1, 2007 to December 31, 2016. Candidates with the following were excluded: 39 with incomplete history, one with amoeba liver abscess, three with tuberculosis liver abscess, and three younger than 18 years of age. The remaining 392 patients were assigned to either the GFPLA or non-GFPLA group, according to the presence (n = 66) or absence (n = 326) of gas in the abscess, respectively. Gas-forming PLA, that is, with gas in the abscess based on ultrasound or computed tomography (CT) image findings. All patients with PLA received second-or third-generation cephalosporins combined with metronidazole or antibiotic agents selected according to the drug sensitivity of pus culture. Depending on the number, size, liquefaction, and separation of the abscess, response to antibiotic agents, and the professional opinion of the doctor, the patients were given antibiotic agents alone, antibiotic agents combined with percutaneous drainage, or surgical drainage [11,12].
Data collection
A retrospective comparison and analysis was conducted of the clinical features and prognosis of patients in the GFPLA and non-GFPLA groups. Clinical data included demographic data (age and gender), lifestyle habits (smoking and drinking), comorbidities, medical histories, symptoms and signs at admission, and changes during hospitalization. Laboratory data included routine blood examination and liver, renal, and coagulation functions. The number, size, and site of the abscess were determined by ultrasound, CT, or both. Bacterial culture included blood culture within 24 hours after admission and pus culture was executed through puncture-guided ultrasound or CT. Treatment included antibiotic agents alone, antibiotic agents combined with percutaneous drainage, or surgical drainage. Complications included sepsis, septic shock, acute kidney injury (AKI), acute respiratory distress syndrome (ARDS), spontaneous rupture of abscess, systemic inflammatory response syndrome (SIRS), pleural effusions, and portal venous thrombosis. The clinical effect was based on the days of temperature normalization after admission, length of hospital stay, and mortality in hospital.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation, and categorical variables as absolute numbers and percent frequencies. Differences between continuous data were analyzed using Student t-test. Differences between categorical data were analyzed with the χ2 test or Fisher exact test, as appropriate. All statistical analyses were performed with SPSS version 22.0 (IBM, Armonk, NY). A two-tailed p value <0.05 was considered statistically significant.
Results
Demographic data, lifestyle habits, etiologies, comorbidities, and medical histories
Among the overall study population of 392 patients, there were 66 with GFPLA and 326 with non-GFPLA, aged 57.0 ± 13.7 and 56.7 ± 13.3 years, respectively (Table 1). The corresponding ratios of men to women in the two groups were 38:28 and 185:141, respectively. The GFPLA and non-GFPLA groups were statistically similar regard to gender ratio, age, smoking, drinking, and comorbidities. The two groups had similar etiologies in portal vein seeding, bowel and/or pelvic pathology, hepatic artery seeding, hematogenous infection, direct extension, trauma to the liver (all p > 0.05). However, the GFPLA group had more biliary source infection and less cryptogenic infection (p = 0.022 and 0.010, respectively). A history of abdominal surgery was significantly more common in patients with GFPLA compared with non-GFPLA (p = 0.002), especially hepatobiliary surgery (p = 0.024). In hepatobiliary surgery, biliary tract surgery was more common in GFPLA patients (p < 0.001), especially biliary enteric anastomosis (p = 0.030). A greater percentage of the non-GFPLA group had no history of surgery compared with the GFPLA (p = 0.002). There was no significant difference in the medical history of PLA between the two groups (p = 0.086).
Demographic Data, Lifestyle Habits, Etiologies, Comorbidities, and Medical Histories a
Reported as n (%), unless shown otherwise.
GFLPA = gas-forming pyogenic liver abscess; ERCP = endoscopic retrograde cholangiopancreatography; PLA = pyogenic liver abscess.
Clinical manifestations, laboratory results, and imaging findings
Clinical manifestations
Table 2 shows that there were no differences in the symptoms and signs of fever, chill, abdominal pain, nausea, vomit, fatigue, body temperature, respiratory rate, or mean arterial pressure (MAP) between the two groups. However, the heart rate of the GFPLA group was faster than that of the non-GFPLA group (Table 2; p = 0.028).
Clinical Features, Laboratory Results, and Imaging Findings a
Reported as n (%), unless shown otherwise.
GFLPA = gas-forming pyogenic liver abscess; AST = aspartate transaminase; ALP, alkaline phosphatase; GGT, γ-glutamyl transferase; TBIL, total bilirubin; ALB = albumin; Cr, = creatinine; BUN = blood urea nitrogen; PT = prothrombin time; APTT = activated partial thromboplastin time; FIB = fibrinogen.
Laboratory results
Routine blood examination
As shown in Table 2, the GFPLA group had higher leucocytes and neutrophils than did the non-GFPLA group (p = 0.005 and 0.003). However, the lymphocytes, platelets, and hemoglobin of the GFPLA group were lower than that of the non-GFPLA. Specifically, the lymphocyte count in the GFPLA group was lower than that of the non-GFPLA group (p = 0.007). The platelet counts in the GFPLA group was lower than that of the non-GFPLA group (p = 0.019). The hemoglobine content in the GFPLA group was lower than that of the non-GFPLA group (p = 0.01).
Liver and renal functions
As showed in Table 2, there were no differences in alanine transaminase (ALT), aspartate transaminase (AST), alkaline phosphatase (ALP), glutamyl transpeptidase (GGT), total bilirubin (TBIL), direct bilirubin (DBIL), serum creatine (Cr), and blood urea nitrogen (BUN) between the two groups. However, the level of serum albumin (ALB) in the GFPLA group was lower than that of the non-GFPLA group (p < 0.001).
Coagulation function
As shown in Table 2, there were no differences in activated partial thromboplastin time (APTT) and fibrinogen (FIB) between the two groups. The prothrombin time (PT) of the GFPLA group was longer than that of the non-GFPLA group (p = 0.006).
Image findings
As shown in Table 2, the two groups were similar with regard to percentages of single or multiple abscesses. Specifically, in the GFPLA and non-GFPLA groups there were, respectively, 52 (78.8%) and 239 (73.3%) cases of single abscess, and 14 (21.2%) and 87 (26.7%) cases of multiple abscesses. However, the maximum diameter was significantly higher in the GFPLA compared with the non-GFPLA (p = 0.001). There were 57 patients in the GFPLA group and 288 in the non-GFPLA group. Among them, in the GFPLA and non-GFPLA groups there were, respectively, 11 (19.3%) and 35 (12.2%) located in the left lobe of the liver, and 39 (68.4%) and 216 (75.0%) were located in the right lobe. Seven (12.3%) GFPLA and 37 (12.8%) non-GFPLA were found in both sides of the liver lobe; abscess site was similar in both groups.
Microbiologic characteristics
3.3.1 Pus culture
There were similar pus microbiologic proportions (Table 3; p > 0.05), number of pus bacterial species (Table 3; p = 0.054), and pus negative rate (Table 3; p = 0.491) between the two groups. Most of the positive bacteria in pus culture were Klebsiella pneumoniae, followed by Escherichia coli.
Microbiologic Characteristics a
Reported as n (%), unless shown otherwise.
GFLPA = gas-forming pyogenic liver abscess.
3.3.2 Blood culture
There were similar blood microbiologic proportions (Table 3; p > 0.05) and number of blood bacterial species (Table 3; p = 0.335). Most of the positive bacteria in pus cultures were Klebsiella pneumoniae, followed by Escherichia coli, which was consistent with the results of pus cultures between the two groups. However, the non-GFPLA group had a higher blood negative rate than GFPLA group (Table 3; p = 0.017).
Treatments, complications, and outcomes
Treatments
In the non-GFPLA group, 95 (29.1%), 159 (48.8%), and 72 (22.1%) patients received routine anti-infection therapy, percutaneous transhepatic puncture drainage under the guidance of ultrasound or CT, and surgical drainage, respectively (Table 4). In the GFPLA group, these corresponding treatments were administered to 12 (18.2%), 45 (68.2%), and nine (13.6%) patients. A higher percentage of patients in the GFPLA group received antibiotic agents combined with percutaneous drainage compared with the non-GFPLA, but a lower percentage in the GFPLA underwent either conservative treatment or surgical drainage (Table 4; p = 0.016).
Treatments, Complications, and Outcomes a
Reported as n (%), unless shown otherwise.
GFLPA = gas-forming pyogenic liver abscess; ARDS = acute respiratory distress syndrome; AKI = acute kidney injury; SIRS = systemic inflammatory response syndrome.
Complications
The GFPLA and non-GFPLA groups were similar in the occurrence of the following complications: septic shock, ARDS, spontaneous rupture of abscess, SIRS, and portal venous thrombosis (Table 4; p > 0.05). However, the GFPLA group had higher rates of sepsis (Table 4; p = 0.005) and pleural effusion (Table 4; p = 0.002) compared with the non-GFPLA group.
Outcomes
The groups were similar in days for temperature normalization after admission (Table 4; p = 0.298). However, the patients in the GFPLA group experienced a longer hospital stay compared with the non-GFPLA (Table 4; p = 0.029). There were no deaths in either group during hospitalization.
Discussion
The clinical features and prognosis of GFPLA has not been sufficiently elucidated. Few studies have investigated the role of gas-formation in PLA [5,10,13,14]. In the present study, we retrospectively compared the clinical features and outcomes of GFPLA and non-GFPLA. The analysis found that the GFPLA group had more biliary source infection and less cryptogenic infection in etiologies. Gas-forming pyogenic liver abscess was associated with previous hepatobiliary surgery, especially biliary enteric anastomosis. Gas-forming pyogenic liver abscess was associated with high rates of sepsis, pleural effusion, and long hospitalizations. More importantly, there were no major differences in the overall outcomes between the GFPLA and non-GFPLA patients.
Lee et al. [10] reported that patients with past gastrectomy may be prone to GFPLA because of alteration of gut flora. In the present study, the GFPLA group had more biliary source infection and less cryptogenic infection in etiologies. Gas-forming pyogenic liver abscess was more prevalent in patients with a history of hepatobiliary surgery, especially biliary enteric anastomosis. A comparative study found that PLA with cryptogenic infection had higher improvement rate without complication and recurrence than PLA with biliary source infection [15]. Although our current data cannot confirm that hepatobiliary surgery is an independent risk factor for GFPLA, it does suggest an association, which may predict a worse prognosis.
The symptoms and signs of the GFPLA and non-GFPLA groups were not statistically comparable, except that the higher heart rate in GFPLA. It has been reported that an elevated heart rate is associated with increased mortality and cardiovascular risk in patients with no substantial heart disease [16]. Moreover, the GFPLA group had higher levels of leucocytes and neutrophils, lower levels of lymphocytes, hemoglobin, platelets, and albumin compared with the non-GFPLA. All of this suggests more severe infections and a poorer prognosis. In addition, plain abdominal radiograms can be used for detecting gas. The air-fluid level or mottled gas pattern are the most common findings of GFPLA patients on plain abdominal radiograms [17]. However, ultrasonography and CT are more sensitive than plain abdominal radiograms for detecting PLA with or without gas. In our study, imaging analysis showed that the abscesses of the GFPLA group were usually larger. This finding is consistent with Chou et al. [13] and may be caused by the expansion of the abscess with infection and gas formation.
In the past, abscess drainage was mainly accomplished through surgery. However, percutaneous aspiration or drainage has now become the standard [18,19]. Our study showed the same results. However, the rate of antibiotic agents combined with percutaneous drainage was higher in the GFPLA group, and the rates of antibiotic agents combined with surgical drainage and antibiotic agents alone were lower. This may be because the patients with GFPLA had a higher positive rate of bacteria in blood culture. It was thus easier to select sensitive antibiotic agents for curing the disease. Although no in-hospital deaths occurred in either group, the GFPLA group had a higher occurrence rate of pleural effusion and sepsis and longer hospital stays than the non-GFPLA group. Earlier studies reported that patients with GFPLA have a high mortality rate [14,20], however, because of differences in the etiologies, diagnosis, and treatments of PLA, the mortality of GFPLA still needs investigation. Patients with GFPLA deserve more attention from clinicians because of the higher rate of complications.
Several limitations of this study need to be considered. First, the data were from only a single center, and most of the patients reside in the Shaanxi Province of China. Considerable differences in etiology, treatment, and outcomes of PLA have been revealed in recent studies from different parts of the world [21–23]. Therefore, our findings need to be verified by multicenter research. Second, this is a retrospective study and subject to selection bias and residual confounding. Finally, we only investigated the short-term results of PLA in this study. This is because the underlying disease would influence the long-term outcomes of the patient. To evaluate GFPLA for higher incidence and mortality, a prospective study with propensity score matching is necessary.
Conclusions
The GFPLA group had more biliary source infection and less cryptogenic infection in etiologies. Gas-forming pyogenic liver abscess preferentially occurs in patients with a history of hepatobiliary surgery, especially biliary enteric anastomosis. Although both GFPLA and non-GFPLA can be cured timely and effectively, the GFPLA group had a more serious infections, larger abscesses, higher incidence of pleural effusion, sepsis and longer hospital stay compared with the non-GFPLA group. Thus, the patients with PLA with a history of hepatobiliary surgery should be monitored more closely in the early stage of PLA. It needs to be recognized as a distinct clinical entity.
Footnotes
Acknowledgments
This study was approved by the Ethics Committee of the First Affiliated Hospital of Xi'an Jiaotong University (XJTU1AF2015LSL-057). The patient's informed written consent to analysis of their medical records was waived because of the retrospective nature of this study. And no further permission from the hospital was required.
Authors' Contributions
R. Wu designed the research; Z. Wu and Lv supported the research; Zhang, Gao, Du, Bi, and Du collected the data; Zhang analyzed the data; R. Wu and Zhang wrote the manuscript; R. Wu supervised the whole research. All authors have read and approved the final manuscript.
Funding Information
This work was supported by grants from the National Natural Science Foundation of China (No. 81770491) and the Innovation Capacity Support Plan of Shaanxi Province (No. 2020TD-040).
Author Disclosure Statement
The authors declare that they have no competing interests.