
Abstract
Background:
Infected hernia mesh is a cause of post-operative morbidity. Nitric oxide (NO) plays a key role in the endogenous immune response to infection. We sought to study the efficacy of a NO-releasing mesh against methicillin-resistant Staphylococcus aureus (MRSA). We hypothesized that a NO-releasing polyester mesh would decrease MRSA colonization and proliferation.
Materials and Methods:
A composite polyester mesh functionalized with N-diazeniumdiolate silica nanoparticles was synthesized and characterized. N-diazeniumdiolate silica parietex composite (NOSi) was inoculated with 104,106, or 108 colony forming units (CFUs) of MRSA and a dose response was quantified in a soy tryptic broth assay. Utilizing a rat model of contaminated hernia repair, implanted mesh was inoculated with MRSA, recovered, and CFUs were quantified. Clinical metrics of erythema, mesh contracture, and adhesion severity were then characterized.
Results:
Methicillin-resistant Staphylococcus aureus CFUs demonstrated a dose-dependent response to NOSi in vitro. In vivo, quantified CFUs showed a dose-dependent response to NOSi-PCO. Treated rats had fewer severe adhesions, less erythema, and reduced mesh contracture.
Conclusions:
We demonstrate the efficacy of a NO-releasing mesh to treat MRSA in vitro and in vivo. Creation of a novel class of antimicrobial prosthetics offers new strategies for reconstructing contaminated abdominal wall defects and other procedures that benefit from deploying synthetic prostheses in contaminated environments.
Mesh infection after ventral hernia repair increases morbidity and mortality [1]. Infection complicates 1%–2% of all abdominal wall reconstructions during which mesh is implanted [2]. Mesh construction influences post-operative infection risk, with the highest risk observed in multifilament polyester mesh; infection complicates 7.0%–16% of such implants [3,4]. Although salvage of infected mesh has been reported using long-term antibiotic therapy, device explantation to achieve source control coupled with a shorter course of antibiotic therapy is the current standard of care [5,6]. Long-term antibiotic therapy drives the development of multi-drug resistance, exerts pressure on the colonic microbiome toward the emergence of Clostridium difficile infection, and transforms the microbiome into a pathobiome [7,8]. The efficacy of antibiotic therapy even when the identified organisms are susceptible may be impeded by the biofilm that characteristically accompanies prosthetic mesh infection. These observations necessitate developing alternate approaches to reducing bacterial contamination, invasion, and infection of prosthetic mesh [9,10].
Silver, gold, and chlorhexidine all demonstrate bactericidal activity in a variety of infection models against a wide array of bacteria [10–13]. Indeed, bonding any of these materials to medical devices decreases infection rates associated with central venous catheters, urinary catheters, and endotracheal tubes. Relatedly, antibiotic agents have also been bound to implantable mesh with varied success in vitro and in vivo [14–16]. Whereas elements such as silver and gold demonstrate limited resistance induction, bonded antibiotic agents demonstrate resistance profiles similar to those of systemically delivered agents. Therefore, there is increased interest in non-antibiotic approaches to infection prevention and therapy. Approaches include microbiome support to prevent transformation into a pathobiome, phage therapy, and anti-sense oligonucleotides [17], as well as biologically inspired molecules such as nitric oxide (NO) [18–20].
Nanomaterial development enables the therapeutic delivery of bioactive molecules. As delivery vehicles for antimicrobial agents, they represent a new tool in the design of antimicrobial therapeutics [10,21,22]. Nitric oxide, a diatomic free radical, plays a key role in the endogenous immune response to infection [23]. Polymorphonuclear cells (PMNs, neutrophils) utilize NO to disrupt bacterial cell membranes and interfere with DNA replication [24]. Exogenous NO is effective in preventing biofilm formation and in killing a broad spectrum of bacteria [25,26]. However, NO is limited by an extremely short half-life [12,23,27,28]. To overcome this limitation, NO may be stored and released over time using synthesized nanoparticle-based delivery vehicles; large-volume NO delivery is thus achievable [23]. We functionalized a multifilament composite polyester mesh with a source of NO in the form of N-diazeniumdiolate as a therapeutic to apply against a prototype drug-resistant pathogen, methicillin-resistant Staphylococcus aureus (MRSA). We hypothesized that a nitric oxide-releasing silica nanoparticle (NOSi)-bearing mesh would demonstrate enhanced MRSA killing in both an in vivo and in vitro model of mesh infection.
Materials and Methods
Synthesis of NO-releasing silica nanoparticles
Nitric oxide-silica nanoparticles were synthesized via a co-condensation of tetraethoxysilane with aminoalkoxysilane under high-pressure nitrous oxide for three days as previously described (Fig. 1) [12,29]. To synthesize the initial silane solution, 2.78 mmol tetraethyl orthosilicate (TEOS; Sigma-Aldrich, St. Louis, MO) was mixed with N-(2-aminoethyl)-3-aminopropyltrimethoxysilane (AEAP3; Gelest Inc, Morrisville, PA) to achieve a 17% mol AEAP3/TEOS solution. This solution was mixed for five minutes and then added in a drop-wise fashion to a mixture of 6 mL of 30% weight-in-water ammonium hydroxide (Sigma-Aldrich) and 22 mL 100% ethanol (Decon Laboratories Inc., King of Prussia, PA). The silane solution was then stirred for 30 minutes under ambient conditions. After this, the solution underwent centrifugation at 5,000 rpm for five minutes to collect the precipitated amine-functionalized silica particles. The product was washed three times with 100% ethanol and then vacuum dried overnight [30,31].
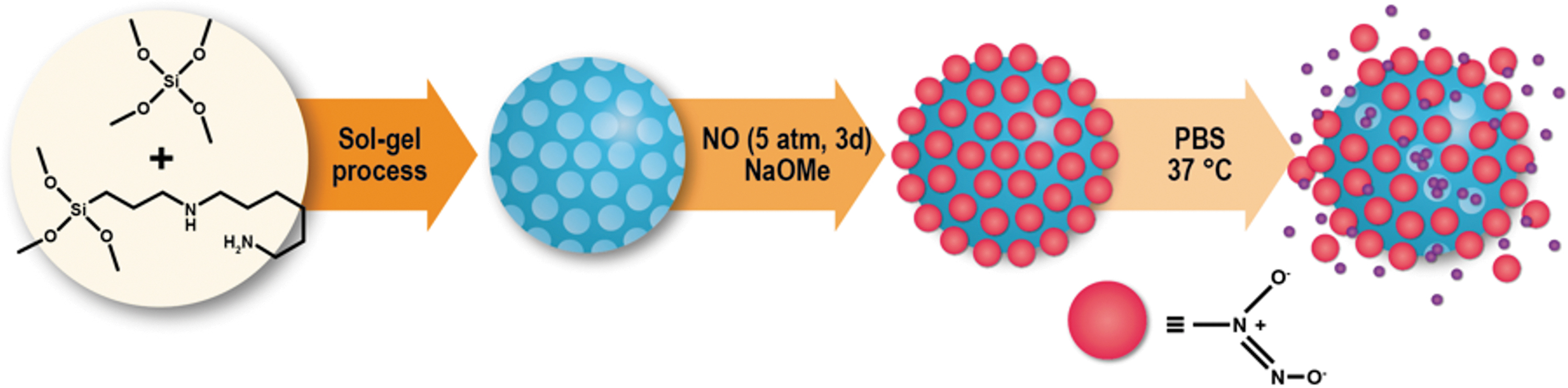
Schematic illustrating nitric oxide-releasing silica nanoparticle (NOSi) synthesis and action. Phases of NOSi synthesis starting with sol-gel reaction and pressurized nitric oxide (NO) and ending with release of NO species upon reaction with aqueous solution. PBS = phosphate buffered saline. Color image is available online.
Creation of N-diazeniumdiolate silica (NOSi) particles was performed as previously reported [12,29]. In brief, aminated silica particles were suspended in a solution of 10% v/v methanol (Sigma-Aldrich) in N,N-dimethylformamide (DMF; Fisher Scientific, Hampton, NH). This solution was then transferred to a Q-tube™ (Sigma-Aldrich) pressure reactor with a magnetic stir bar. An equimolar amount of sodium methoxide (Sigma Aldrich) to AEAP3 was then added to the reaction. The Q-tube reaction chamber and tubing was then purged of remnant oxygen with nitrogen gas (Matheson, Houston, TX) three times. Then, the Q-tube was pressurized to 75 psi with NO gas (Matheson) for 72 hours with constant stirring at room temperature. Prior to removing the solution, the Q-tube was again purged with nitrogen gas (Matheson) three times to remove any remaining NO. The solution was then centrifuged at 5,000 rpm for 10 minutes to collect the N-diazeniumdiolate silica nanoparticles. These particles are then washed in isopropanol (IPA; Fisher Scientific), desiccated overnight, placed in IPA in a sealed container, and stored at −20°C until use [31].
Characterization of NOSi
To characterize size and charge, dynamic light scattering and zeta-potential characterization were performed using a Zetasizer ZEN3600 (Malvern, Worcestershire, UK). Scattered light detection was measured at 90 degrees to the incident beam (a 25 mW laser at 660 ηm wavelength) to assess nanoparticle size. For Zeta-potential analysis, the same parameters were used, but scattered light was detected at 15 degrees. Fourier transformed infrared spectroscopy was performed by creating a pellet of 5% sample and 95% KBr (Sigma Aldrich) by volume and analyzing absorbance of the pellet on a Nicolet 6700 FT-IR Spectrometer (Thermo Fisher Scientific, Philadelphia, PA). Samples were prepared for scanning electron microscopy (SEM) by drying nanoparticles onto a titanium stage and sputter coating with a 5 ηm thick layer of platinum/palladium using a Sputter Coater 208HR (Cressington Scientific, Watford, UK). Microscopy images were taken using a Nova NanoSEM 230 (FEI, Hillsboro, Oregon) [32].
Nitric oxide release characterization
Nitric oxide release characterization was undertaken in two steps. Initially, the Griess reaction was utilized to confirm the presence of N-diazeniumdiolate modification through the oxidation of released NO to nitrite in aqueous solution. The cumulative release of nitrite oxidized from NO release from NOSi particles was collected over two hours. Five milligrams of N-diazeniumdiolate silica or AEAP3 silica were suspended in 1 mL Millipore water and continuously agitated. After this, every 15 minutes for two hours, the reaction solutions were centrifuged at 16,000 rpm for five minutes, to pelletize particles, and 900 mcL of the supernatant was removed. A small sample of the collected supernatant was then added to three wells of a 96-well plate (Falcon). After removal, new Millipore water was added to the reaction tubes, and silica was re-suspended via brief sonication using Branson SFX150 Ultrasonic Processor with Converter, 150 W, 40 kHz, 240 VAC (Cole-Parmer, Vernon Hills, IL). At the end of the time points, Griess reaction reagents were added to the collected supernatant, and the colored product was read on a Nicolet 6700 FT-IR Spectrometer at a wavelength of 548 nm. All negative values were interpreted as zero NO release.
To best characterize total NO release and release over time, NO was measured using chemiluminescence [12,29]. The NO release profile for NOSi nanoparticles was measured in phosphate buffered saline (PBS) at 37°C using a Sievers NOA 280i chemiluminescence (General Electric Power, Boulder, CO) NO analyzer. The instrument was calibrated with NO gas that was passed through a 0.2-mcm filter. A known mass of NOSi particles was placed in the collection chamber; generated NO was carried to the analyzer with a stream of N2 bubbled into the buffering solution at a flow rate of 120 mL/min. Within the analyzer, NO was detected via chemiluminescent reaction with ozone as previously described [31,33]. The area under the curve was integrated to quantify total generated NO.
Composite polyester mesh functionalization and characterization
After preparation of NOSi particles, mesh samples were prepared for characterization and implantation. Prior to coating with particles, Parietex™ Composite (PCO; Covidien, King of Prussia, PA) mesh was cut into identical oval-shaped pieces measuring 2.5 × 1.5 cm. Increasing amounts of NOSi ranging from 2–140 mg were loaded onto the mesh for characterization and in vitro testing. The NOSi particles were homogenized in 1 mL IPA by sonication and then coated onto the mesh in a drop-wise fashion until the entire mesh was covered. The NOSi particle-coated mesh (NOSi-PCO) was then desiccated at 37°C for 12 hours and weighed to confirm the addition of the specified mass of particles. If the specified mass had not been achieved, particles were added to the mesh to achieve specified mass. Samples were then characterized by SEM to assess the homogeneity of NOSi particle distribution. Samples were prepared for SEM by placing functionalized mesh on a graphite covered titanium stage and sputter coating with a 5 ηm thick layer of platinum/palladium using a Sputter Coater 208HR (Cressington Scientific, Watford, UK). Microscopy images were taken using Nova NanoSEM 230 (FEI, Hillsboro, OR). To confirm that the release of NO was not negatively affected by functionalization, NOSi-PCO were analyzed for NO release by chemiluminescent NO detection as previously described.
Cytotoxicity assay
Human mesenchymal stem cells (MSCs) served as a test platform for cytotoxicity analysis. Adipose-derived human MSCs were acquired from Lonza (Basel, Switzerland) and cultured in αMEM until passage 4 (P4). Human mesenchymal stem cells were chosen given their importance in wound healing and local wound inflammatory signaling [34,35]. Human mesenchymal stem cells at P4 were seeded (15,000 cells per well) in a black-walled, clear-bottomed, 96-well plate (to prevent fluorescence bleeding between wells). Cells were treated 18 hours after seeding with varying concentrations of NO particles (0.5, 1.0, 3.0, and 6.0 mg/mL; n = 3) or chlorhexidine (0.05%, 0.1%, 0.2%, and 0.4% w/v; n = 3). Clinically relevant amounts of both NOSi and chlorhexidine were chosen to assess cytotoxicity. Chlorhexidine was chosen because it is a clinically utilized bactericidal agent with known cytotoxic effects. Twenty-four hours after treatment with either NO or chlorhexidine, treated media was removed and 100 mcL of fresh media (αMEM) was added to all wells with 20 mcL of 3-(4,5-dimethylthiazol-2-yl)-2, 5-diphenyltetrazolium bromide (MTT; Life Technologies, Carlsbad, CA) at a concentration of 5 mg/mL in media. Two hours after incubation with MTT, all media was aspirated and 50 mcL dimethyl sulfoxide (DMSO; 99.5%) was added to lyse human MSCs and dissolve MTT crystals to measure human MSC DNA. Fluorescence readings (λ = 570 nm) were then taken using a plate reader. Absorbance values were normalized and significance was determined using Student t-test. All chemicals were purchased from Sigma-Aldrich.
Microbial assays under static conditions
For all bacterial experiments, USA300 strain LAC was selected because its genome has been sequenced, the strain is genetically representative of MRSA strains causing epidemic infections in the United States, and it has been used in numerous animal infection models [36–38]. Briefly, bacteria were grown for 12 hours in trypic soy broth (TSB) at 37°C, inoculated 1:100 into pre-warmed TSB, and grown to mid-exponential phase (OD600 = 0.4–0.6). The actively growing cells were diluted to OD600 = 0.2 (approximately 108 CFU/mL). The suspension was then further diluted to 104, 106, or 108 CFU/mL and added to a vial containing a standardized volume of NOSi at the indicated concentrations. The three doses were selected to approximate the number of MRSA organisms that may be present in a contaminated hernia repair [39,40]. After two hours of incubation at 37°C, recovered CFUs were counted using quantitative culture. Colony-forming units at each NOSi concentration were normalized to the NOSi-deficient control.
Animals
Sixty-three male Lewis rats (300–315 g) underwent ventral hernia repair with Parietex-PCO (Covidien Medtronic, Minneapolis, MN). Each group consisted of seven animals and no animals were excluded from the study. Exclusion criteria was established a priori during the development of the protocol. Animals would be excluded from the study if the animals died prior to the pre-determined time point of 24 hours. Animals were randomly assigned by a random number generator. To maintain blinding, animals were assessed independently by blinded observers not involved in the initial operations or tissue harvest. To maintain blinding during tissue analysis, tissues were numbered by a random number generator and handed off to a blinded investigator who then processed them for CFU. Lewis rats were chosen because of their inbred nature. Animals (Charles River, Wilmington, MA) were housed at Houston Methodist Hospital Research Institute (HMHRI) animal facility. The study was approved by the HMHRI Institutional Animal Care and Use Committee (IACUC; Protocol # AUP-1012-0047). All investigators complied with the National Research Council's Guide for the Care and Use of Laboratory Animals. Food and water were replenished daily. Animals were examined daily, and all health issues were addressed.
Abdominal wall defect creation
Abdominal wall defect creation was carried out as previously described [41,42]. Rats were allocated randomly to treatment or placebo groups using a random number generator. Buprenorphine (0.03 mg/kg) and carprofen (5 mg/kg) were administered for pre-operative analgesia. Anesthesia was induced and maintained using a 2.5%–3.0% isoflurane/oxygen mixture through a non-rebreather mask. Aseptic techniques were used for the duration of the surgery. To create the abdominal wall defect, all rats had a 3-cm midline skin incision made and skin flaps raised using sharp dissection. A full thickness abdominal midline fascia/muscle/peritoneum defect measuring 2 cm in length was then created. The defect was left unrepaired, and the skin was then approximated and stapled. The fascial defects were allowed to mature over 28 days. Physical examination was performed, and weights obtained daily for 10 days and then weekly thereafter. Exclusion collars were applied for the first five post-operative days to preserve incision integrity. Staples were removed after 14 days.
Abdominal wall defect repair and inoculation
On day 28 animals underwent hernia repair with NOSi-coated or uncoated mesh. The protruding viscera were freed with sharp dissection and the fascial edges defined. A 2.5 × 1.5 cm piece of mesh was used in order to allow for 5 mm of overlap between muscle and mesh. Animals were allocated into three groups and were implanted with a PCO mesh, PCO mesh and bare silica particles (Si-PCO), or NOSi-treated PCO mesh (NOSi-PCO). Both NOSi-PCO and Si-PCO had 66 mg of NOSi and Si, respectively, loaded onto them. Sixty-six milligrams was chosen because this was the mass of NOSi particles that resulted in no bacterial colony survival at a concentration of 1 × 104. An intra-peritoneal bridging repair was performed using 5-0 Prolene® sutures (Ethicon, Somerville, NJ) spaced equally apart for fascial fixation (Fig. 2A and 2B). Prior to skin closure, 1 × 104, 1 × 106, or 1 × 108 MRSA was then applied directly to the exposed anterior surface of the mesh in a volume of 50 mcl (Fig. 2C). Skin was closed using a 4-0 Monocryl® (Ethicon) running subcuticular stich and then sealed with 3M™ Vetbond™ Tissue Adhesive (3M Animal Care Products, St. Paul, MN) to ensure bacterial solution permanence. Methicillin-resistant Staphylococcus aureus-inoculated animals then survived for 24 hours. It was hypothesized that NOSi-PCO would locally release NO to kill MRSA (Fig. 2D and 2E). Exclusion collars were then re-applied. Buprenorphine (0.03 mg/kg) and carprofen (5 mg/kg) were administered for post-operative analgesia.

Surgical technique. (
Euthanasia and specimen harvest
Animals were euthanized at 24 hours post-inoculation using 70% inhaled carbon dioxide; asystole was confirmed via thoracotomy. After confirmation of death, the presence or absence of skin erythema was recorded. The abdomen was then entered with a C-shaped incision around the mesh and elevated to allow for inspection and scoring. Mesh adhesion severity, adhesion surface area, abscess formation, skin erythema, and mesh contracture were scored and combined to generate a final composite score termed the Mesh Infection Severity Index (MISI; Table 1). All variables in the MISI were equally weighted. Two blinded observers (F.C. and A.T.) scored the erythema and adhesions. Adhesions were scored using two previously validated indices from the Surgical Membrane Study Group [43] and Leach et al. [44] documenting the percentage of mesh covered by intra-peritoneal contents (i.e., intestine, solid organ, or omentum) as well as the severity of adhesion. Adhesions were lysed, and the mesh was assessed for contracture or abscess formation. Abscess formation was defined as the presence of necrotic tissue or debris, purulence, or obvious fluid collection in association with the mesh. The specimens were then taken directly to microbiology for CFU quantification.
Mesh Infection Severity Index
Variables used in the calculation of the Mesh Infection Severity Score (MISI). Adhesion severity, adhesion surface area, abscess formation, overlying skin erythema, and mesh contracture are all scored and MISI quantified to characterize infection severity.
Colony forming unit analysis
All tissue was excised from the mesh, weighed, and homogenized (Omni International) in sterile phosphate-buffered saline (PBS). Serial 10-fold dilutions of the homogenate were plated onto tryptic soy agar supplemented with 5% sheep blood (Remel) and incubated for 12 hours. Recovered MRSA CFUs were counted.
Statistical evaluation
Colony-forming unit recovery counts were log normalized and subsequently analyzed with two-way analysis of variance (ANOVA) followed by Tukey multiple comparisons test. A 95% confidence interval (CI) was determined and a p value ≤0.05 was used to define a statistically significant difference between comparative groups [41]. For severity scoring, normality of population distribution was ensured using Shapiro-Wilk test. For those severity scoring data determined not to be derived from a normally distributed sample, a Kruskal-Wallis test with Dunn multiple comparisons was performed. All statistical analysis was performed with GraphPad Prism 9.0.0 Software (San Diego, CA).
Results
Characterization of NOSi
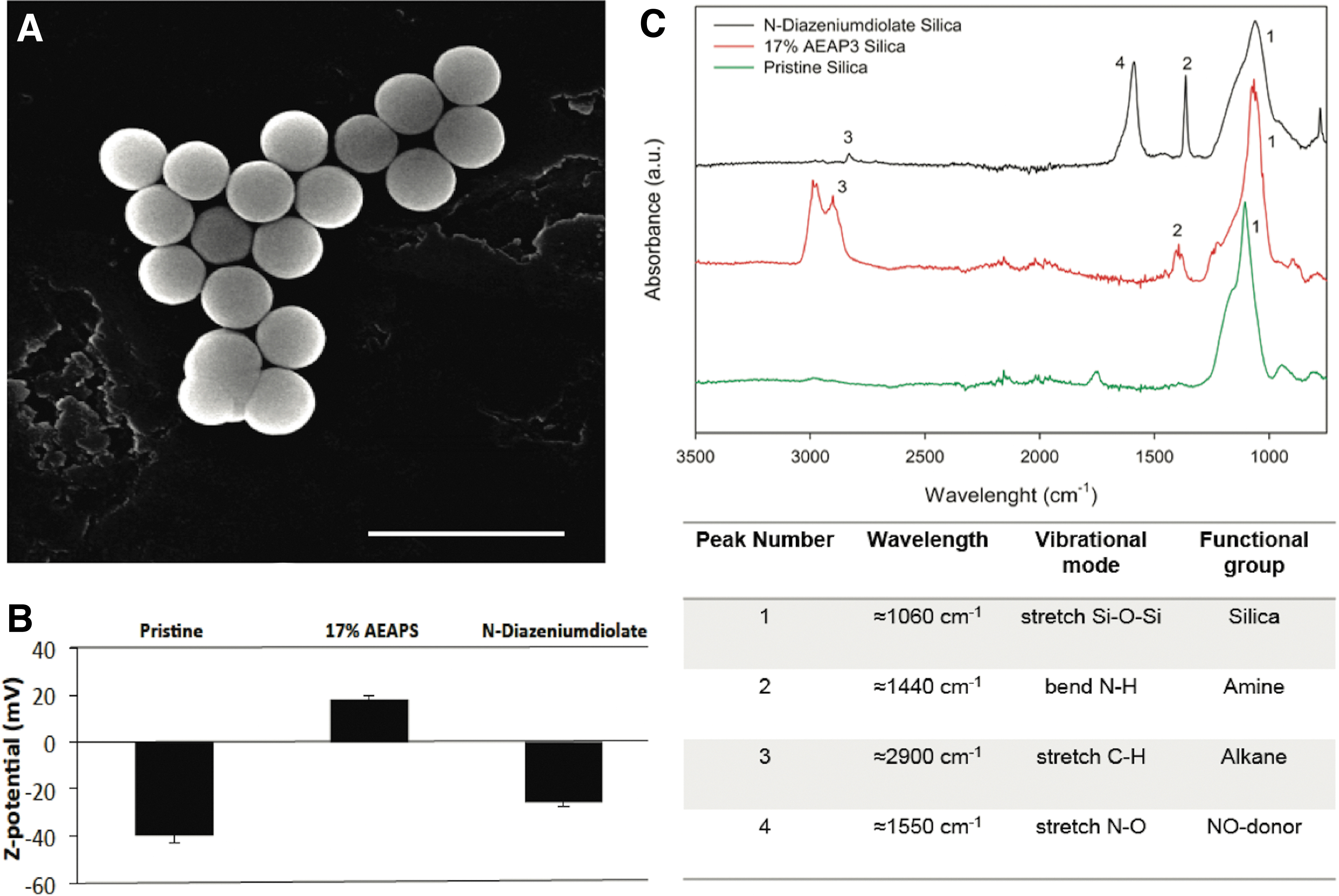
After the co-condensation process and high-pressure NO functionalization, SEM demonstrated spherical particles measuring approximately 600 nm (Fig. 3A). After AEAP3 silica modification, zeta potential analysis demonstrated a mean surface charge of 18.09 mV compared with surface charge of −39.73 mV seen in the unmodified silica (Fig. 3B). Zeta potential after the modification to N-diazeniumdiolate showed a change in charge to −25.38 mV consistent with modification to the negatively charged moiety. Fourier transform infrared (FTIR) analysis through the stages of modification show the appearance and subsequent diminution of the strong alkane C-H stretch at approximately 2,900 cm−1 (Peak 3) in the conversion of AEAP3 silica to N-diazeniumdiolate. This is followed by the concomitant appearance of a strong N-O stretch seen at approximately 1,550 cm−1 (Peak 4) in the N-diazeniumdiolate modified silica, consistent with the creation of the diazenium moiety. Similarly, there is the appearance and progressive sharpening and enhancement of the N-H bend at approximately 1,440 cm−1 (Peak 2; Fig. 3C).
Characterization of nitric oxide-releasing silica nanoparticle (NOSi) particles. (
Nitric oxide release characterization
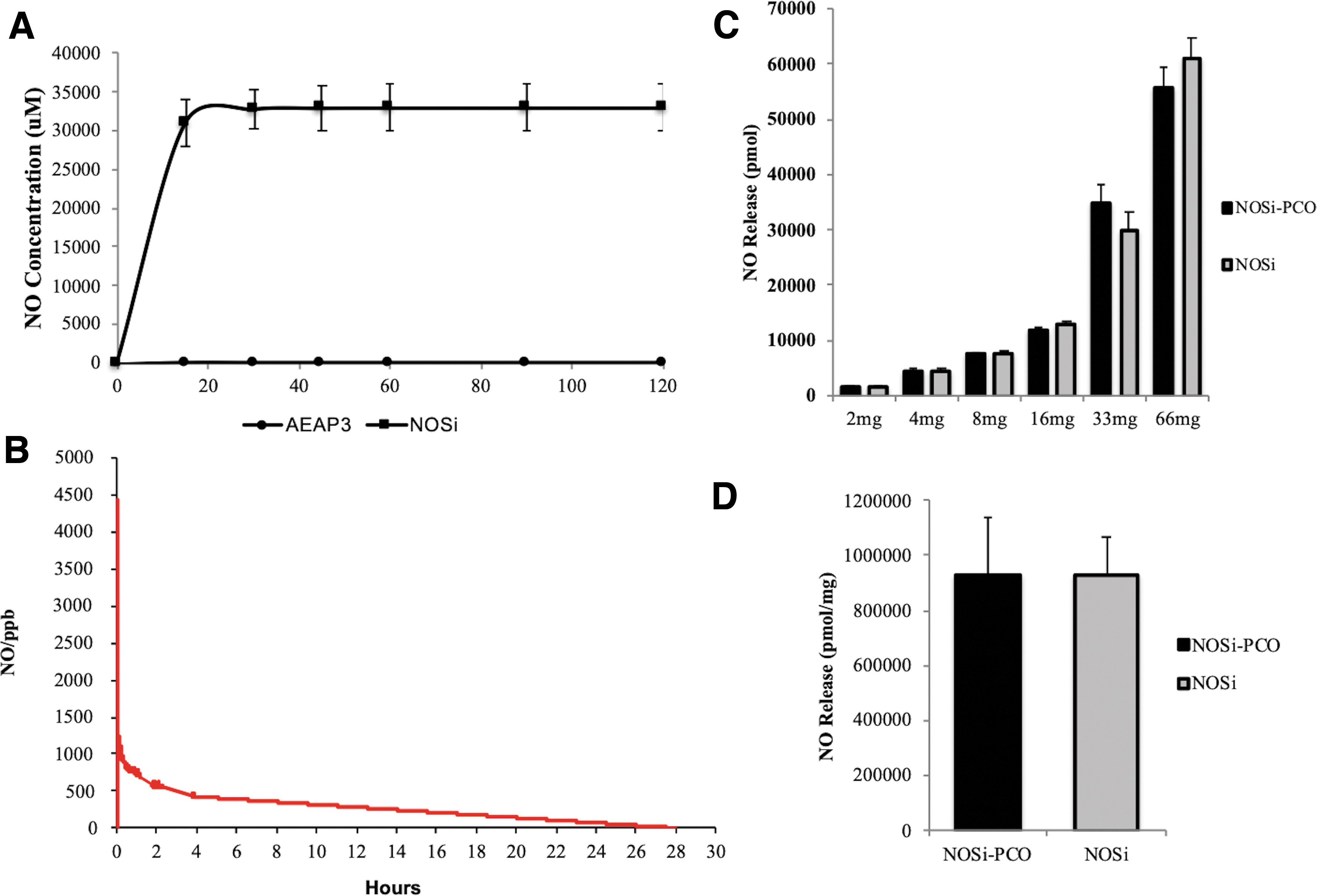
After incubation in aqueous solution, NO released and detected through the Griess reaction as nitrite reached a cumulative concentration of 32,800 mcM (Fig. 4A). Chemiluminescent analysis of released NO demonstrated a characteristic burst release pattern followed by slow NO release (Fig. 4B). Half-life of NOSi NO release is 13.9 ± 0.6 hours (Fig. 4B). Nitric oxide release (nmol) from NOSi and the NOSi-PCO increased with each equivalent increased in mass amount (Fig. 4C).
Nitric oxide-releasing silica nanoparticle (NOSi) nitric oxide (NO) release characterization. (
Characterization of NOSi-PCO mesh
After confirmation of appropriate NO release, mesh was then prepared for characterization. To assess if the addition of NOSi particles to the mesh altered NO release, functionalized mesh underwent fluorometric analysis. Coating of mesh with particles does not affect NO release (Fig. 4C and 4D). Mesh coated with NOSi exhibited similar incremental dose-dependent release profiles. Scanning electron microscopy demonstrated complete and homogeneous surface coating of the mesh with particles (Fig. 5).
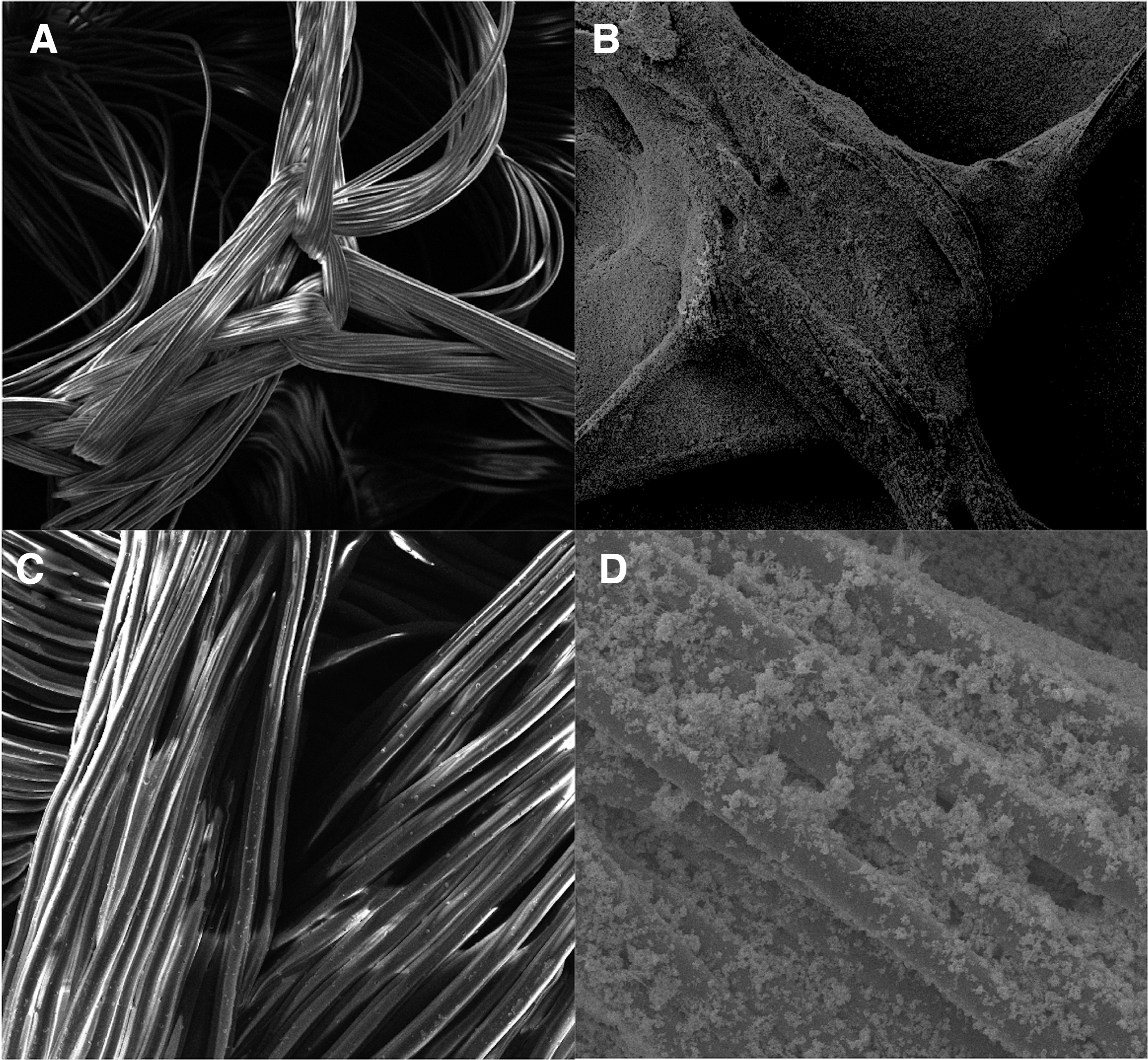
Scanning electron microscope (SEM) of uncoated and coated mesh. Polyester mesh prior to nitric oxide-releasing silica nanoparticle (NOSi) coating seen at 200 × (
Human MSC cytotoxicity
Dose-dependent incremental cytotoxicity for NOSi and chlorhexidine was demonstrated by MTT cytotoxicity assays. At therapeutic concentrations relevant for humans, NOSi demonstrated increased viability compared with chlorhexidine (Fig. 6). At 0.2% (%w/v) chlorhexidine, a concentration found in mouthwash, cell viability was 9%. In comparison, NOSi was consistently found to have a cell viability >35% even at the highest assayed concentrations. At these concentrations, NOSi administration to human MSC is less toxic compared with chlorhexidine.

Nitric oxide-releasing silica nanoparticle (NOSi) treatment has less cytotoxicity than chlorhexidine. 3-(4,5-dimethylthiazol-2-yl)-2, 5-diphenyltetrazolium bromide (MTT) assay performed and human viability quantified for (
Microbial assays under static conditions
To test the hypothesis that NOSi confers antimicrobial activity against MRSA in vitro, standard TSB assays were performed. Consistent with our hypothesis, NOSi demonstrated dose-dependent activity against three concentrations of MRSA (Fig. 7A). At the highest NOSi doses tested, approximately 70%, 99%, and 99% of bacteria were killed in the 108, 106, 104 inocula, respectively.
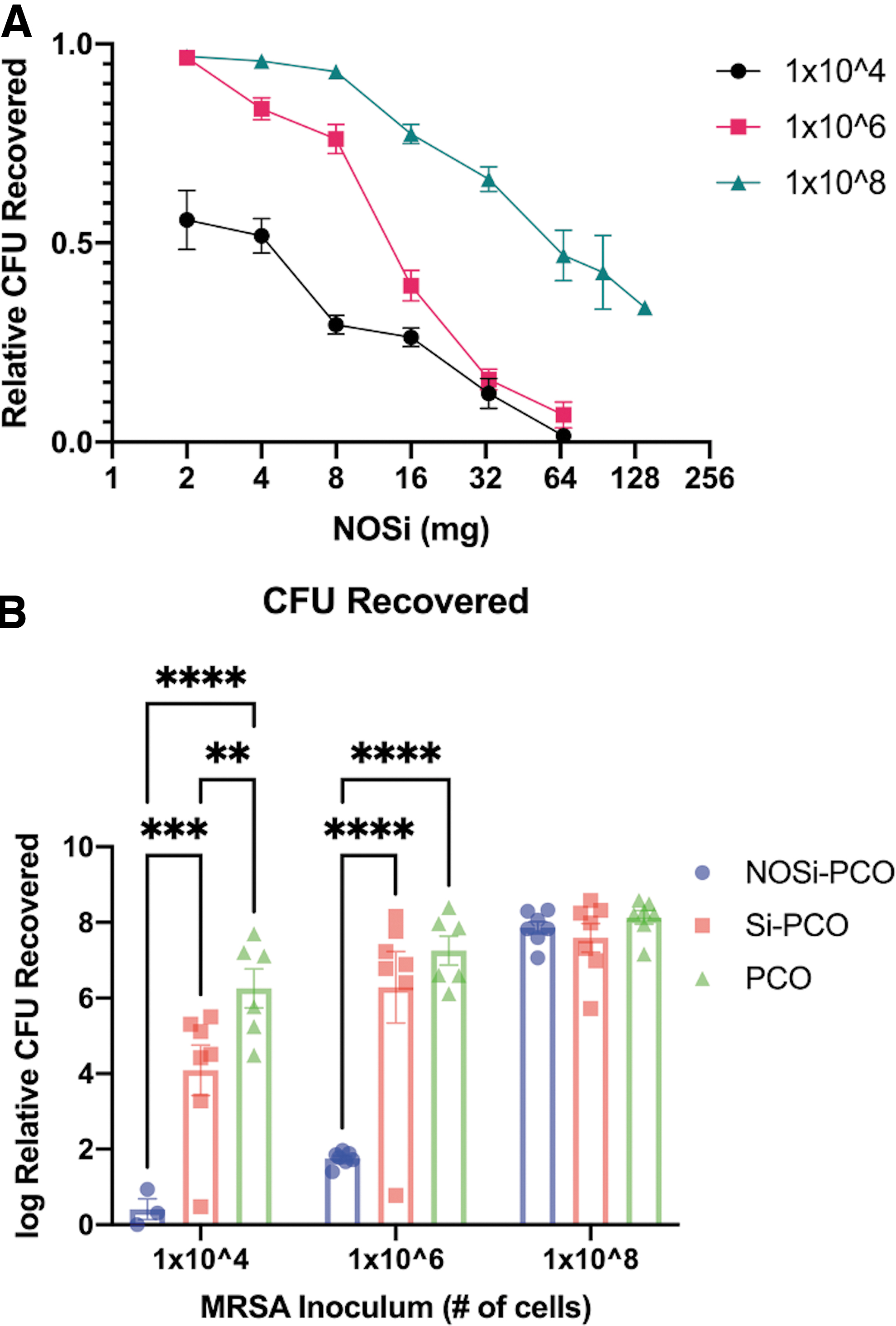
Nitric oxide-releasing silica nanoparticle (NOSi) reduces bacterial inoculum in vitro and in vivo. (
Localized NO release reduces bacterial burden in vivo
To test the hypothesis that NOSi reduces bacterial burden in infected mesh, a rat model of MRSA-contaminated hernia repair was used. Consistent with our hypothesis, compared with control treatments, NOSi-PCO reduced the number of CFUs recovered from mesh inoculated with MRSA at 106 or 104 CFUs (Fig. 7B). No difference in CFU count was noted at 108 and Si-PCO showed no antibacterial properties, comparable to negative controls.
Reduced bacterial burden leads to improved clinical metrics
To assess clinical parameters of infection, the MISI scoring system was created to quantify and stratify the outcomes of mesh contamination and infection better. Hernias repaired with NOSi-PCO mesh had fewer severe adhesions, reduced adhesion area, and overall lower MISI scores (Fig. 8). As the concentration of MRSA was increased, the adhesion severity score, adhesion surface area, and MISI scores were noted to increase in all groups.
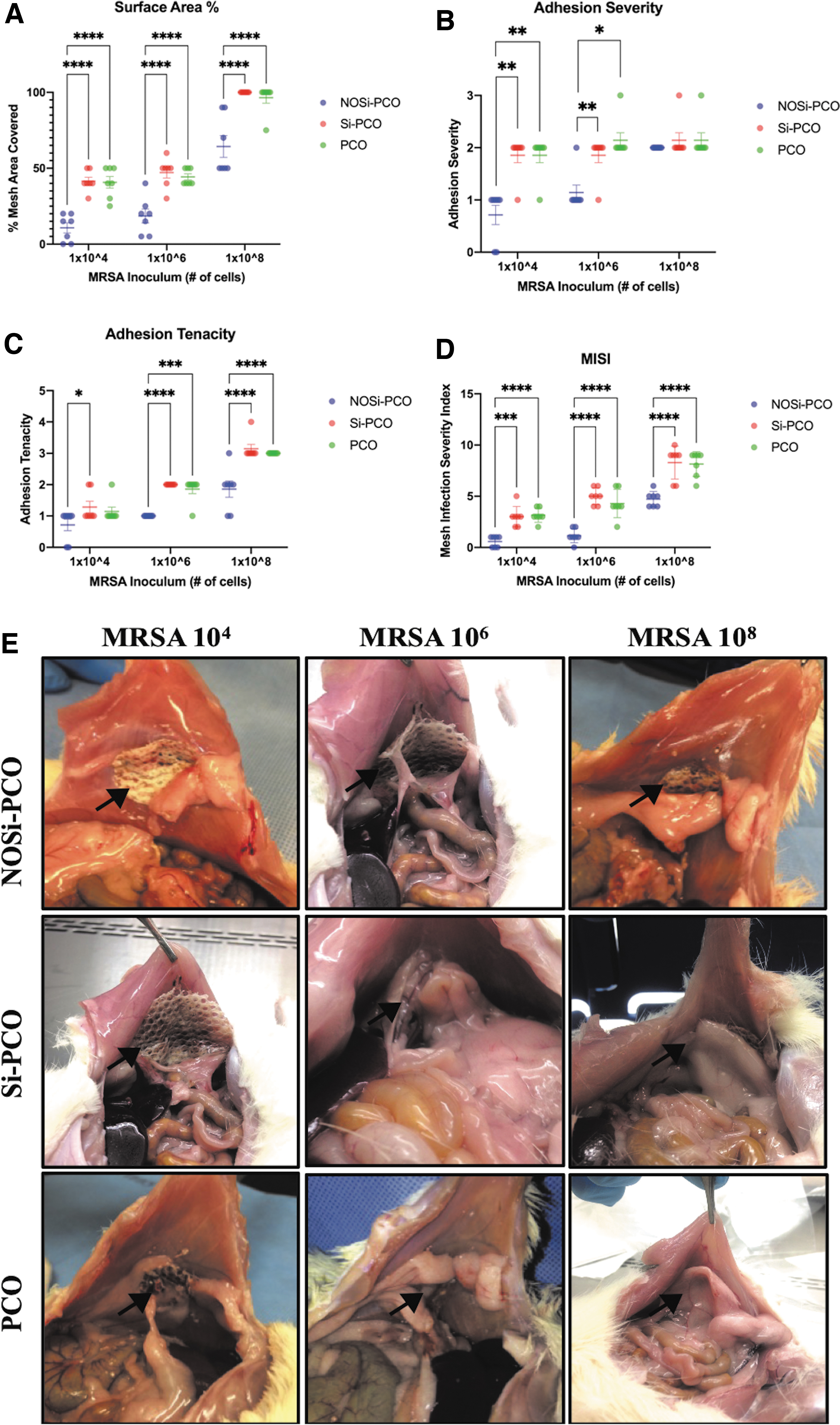
Nitric oxide-releasing silica nanoparticle (NOSi)-treated mesh reduces adhesion severity.
Discussion
Contamination and biofilm formation plague the use of synthetic mesh in the repair of hernias with known (and unknown) contamination [45,46]. Mesh contamination can lead to chronic inflammation, repair breakdown, fistula formation, sepsis, and death [1]. In this study, we describe the utility of localized NO release in decreasing bacterial burden in contaminated synthetic mesh repair of a ventral hernia. Compared with chlorhexidine, NO-releasing silica nanoparticles at therapeutic amounts demonstrated decreased cytotoxicity of model human MSCs. Functionalization of the composite polyester mesh imparted antibacterial properties in vitro and in vivo. In addition, improved clinical metrics in a rat model of contaminated ventral hernia repair were observed. This study indicates that localized NO may be used as a potential agent in the development of next-generation hernia prosthetics for contaminated hernia repair.
Nanomaterial-based NO delivery enables the localized and controlled release of NO necessary to maintain bactericidal concentrations. Although antibacterial efficacy has been demonstrated in vitro as well as in simple small animal models, none has shown utility in addressing a relevant surgical problem, namely synthetic mesh infection in ventral hernia. We sought to investigate the ability of NO functionalization on MRSA infection in a rat model of contaminated ventral hernia repair. Although limited to 24 hours, reductions in bacterial bioburden were noted. In addition to demonstrating the ability of NO functionalization to reduce MRSA colonization, this study also provides insight into clinical features associated with mesh infection and their correlation with bacterial bioburden.
The risk of mesh infection after ventral hernia repair ranges from 10%–25% [47]. Treatment of the contaminated hernia or prevention of mesh infection in high-risk patients is challenging, and limited options are available for surgical repair [45,48].
Antimicrobial meshes have emerged as one option for repair of the hernia that is found in a contaminated space [46]. Several investigational meshes have been constructed using antiseptics (chlorhexidine), traditional antibiotic agents (rifampin, vancomycin, minocycline), metallic nanoparticles (silver and gold), or antimicrobial peptides (lysozymes). Each of these modified meshes have been explored with inconsistent success and none in an animal model of abdominal wall reconstruction [37,43]. However, NO-functionalized silica nanoparticles have demonstrated polymicrobial bactericidal properties [25,49–53]. Previous in vitro and in vivo reports have demonstrated the capability of NO to eradicate both gram-negative bacteria and anaerobes. There have been no studies assessing the effect of NO functionalization of a synthetic implant in vivo or, more specifically, the NO functionalization of a composite polyester mesh for repair of a contaminated hernia. We demonstrate that functionalization of a composite multifilament synthetic mesh with NO-releasing silica nanoparticles can impart antibacterial properties in both an in vitro and in vivo model of abdominal wall reconstruction. Only DualMesh Plus (Gore, Flagstaff, AZ) and XenMatrix AB Surgical Graft (Bard, Warwick, RI) are commercially available meshes specifically modified to slow primary implantation-associated infection. XenMatrix AB is an acellular dermal matrix coated in minocycline and rifampin. A potential advantage of the use of NO over traditional antibiotics such as those in Xenmatrix AB is the lack of resistance development to NO after non-lethal exposure [26]. DualMesh Plus mesh, on the other hand, relies on the controlled release of chlorhexidine coupled with the antibiofilm properties of silver carbonate. Neither has shown a clear benefit in preventing mesh infection after elective implantation [54,55].
In this study, we demonstrated that a composite multifilament polyester mesh could be functionalized with NO-releasing capabilities without affecting the release characteristics of the delivery system or altering the structure of the mesh. Cytotoxicity of human MSCs was also studied in comparison with chlorhexidine, which is found in commercially available prosthetics. We found that NOSi showed decreased human MSC cytotoxicity compared with clinically relevant doses of chlorhexidine. Chlorhexidine 0.2% w/v is currently utilized in antimicrobial mouthwash deployed as part of a ventilator-associated pneumonia prevention bundle and is present on the product label. Surprisingly, the amount of chlorhexidine present in commercially available mesh is not reported. This is particularly relevant given the adverse reactions reported following implantation of DualMesh Plus and the increased stem cell cytotoxicity demonstrated in this model [54].
Controlled release of NO can be achieved from a surgical mesh for up to 24 hours. Increasing the mass of NOSi and, consequently, the dose of NO resulted in a dose-dependent antimicrobial response. In vitro, 104 and 106 concentrations of MRSA, which is the number of bacteria present in the saliva of colonized humans and represents a clinically relevant inoculum, were eradicated with 66 mg and 95 mg of NOSi, respectively. Although even the highest assayed doses of NOSi (140 mg) were unable to fully eradicate the 108 MRSA inoculum, the observed dose-dependent relationship suggests that a higher concentration of NOSi could result in successful killing. In vivo, a fixed dose of NOSi was used and rats inoculated with 104 MRSA achieved near-complete eradication of the inoculum. This is similar to previously published reports [49–51]. In the groups inoculated with 106 and 108 MRSA, reductions in CFU counts seen in vivo were less than those seen in vitro. In the 106 MRSA group, a fourfold reduction was seen in vivo compared with near-complete eradication seen in vitro. This discrepancy is likely because of the nature of the soy broth assay compared with our in vivo test. The TSB assay occurs over six hours whereas mesh is left in place for 24 hours. Given the dose-dependent, yet incomplete, killing of in vitro bacteria in the meshes inoculated with 106 and 108 bacteria, if there was no further antibacterial activity, log replication could result in near restoration of the incompletely eradicated inoculum after 24 hours. Given this is not observed, there is likely ongoing antibacterial activity provided by the NOSi-PCOs.
Understanding clinical variables is critical for the translation of pre-clinical studies into the clinical arena. Although scoring systems exist to predict surgical site infection (SSI) after ventral hernia repair or inguinal hernia repair, none assesses the severity of the infection even when reporting the depth of SSI [56,57]. The MISI provides a holistic analysis of the impact of mesh infection on clinically relevant variables (mesh adhesion severity, adhesion surface area, abscess formation, skin erythema, and mesh contracture). The MISI scores were lowest in the low and moderate bacterial count groups in which bacterial counts were lower than controls. This suggests that the antimicrobial properties of NO strongly correlate with clinical features. Although the bacterial counts were seemingly unaffected in the high bacterial count group, the MISI score was lower because of the absence of mesh contracture and abscess formation. The apparent discrepancy in the data in Figure 7B and that in Figure 8 could potentially be explained by the inflammatory process itself leading to adhesions even when CFUs are decreased by the antimicrobial effect. That is, the inflammation resulting from CFUs is dose-dependent itself, and the inflammation results in increased MISI scores. Future studies could certainly seek to decouple this effect, culturing mesh with soluble inflammatory mediators without CFUs to measure MISI as a result of inflammation alone.
There are multiple limitations of this pilot study. First, the short length of the in vivo study limited relevant investigation as to the long-term effects of NO delivery in a healing wound. Any mesh used in abdominal wall reconstruction must maintain a durable repair through incorporation. The short in vivo assay also limited our ability to analyze the fate of the NOSi-PCO in terms of excretion or absorption. Future studies could focus on this critical clinical question. Second, the short burst release of NO may be more relevant for gastrointestinal pathogens encountered during contaminated cases but may not be as relevant for MRSA infection that may occur at later time points. Hernia infection is most often polymicrobial. It is rare for MRSA to be the only isolate. Given the pilot nature of this study, we did not investigate a polymicrobial infection or other microbes commonly seen such as gram-negative bacteria or anaerobes. A gram-negative enteric such as Escherichia coli, for example, would be more representative of a gut flora microbe that could feasibly cause an infection in a hernia mesh. Future investigations could study whether different inoculum concentrations elicit similar responses in these gram-negative enteric populations compared with the MRSA inoculum used here. Our study also did not use systemic antibiotics, which would have been more representative of standard of care for post-operative infection. Third, the high NO load released may impair healing because cytotoxicity to human MSCs was observed in vitro. Previous data, however, have demonstrated that low-level NO release can actually promote collagen deposition, fibroblast recruitment, and maintain and anti-inflammatory microenvironment [58–60]. Further long-term studies looking more closely at the inflammatory mediators and cellular function in response to NO are needed. Last, lack of histologic analysis of the surrounding tissue is another limitation to the study. Given the need to obtain accurate quantification of the mesh bacterial counts without disrupting the tissue, the whole abdominal wall was used. The available number of animals did not allow for the use of additional animals for histological analysis of the surrounding tissues in this pilot study. Subsequent studies will involve an analysis of the cellular infiltration and local tissue damage. Additionally, a more thorough histologic evaluation of biofilm formation and disruption would add insight to this pathologic mechanism of bacterial self-preservation.
Conclusions
Treatment of a hernia in a contaminated space is a difficult surgical problem. Hernia repair may be complicated by recurrent infection when prosthetic mesh is used to reconstruct the abdominal wall. Antimicrobial meshes are one option to help slow infection during reconstruction of a contaminated space, as well as during elective implantation to prevent infection. The few commercially available antimicrobial meshes have limited efficacy, which may be related to their use of conventional antimicrobials and cytotoxic chemicals. Novel solutions such as antibiotic molecules using a nanoparticle delivery vehicle may provide a viable solution. This study demonstrates that an approach utilizing biologically relevant antimicrobial molecules devoid of identified resistance mechanisms, such as NO, merit specific investigation.
Footnotes
Acknowledgment
This work was presented at the 2014 American College of Surgeons Clinical Congress in San Francisco, California. We would like to thank the American College of Surgeons for graciously allowing us to present our work.
Authors' Contributions
Conceptualization: Fernandez-Moure. Data curation: Fernandez-Moure, Von Eps, Haddix, Livingston, Bryan, Cantu, Valson, Taraballi, Olsen. Formal analysis: Fernandez-Moure, Von Eps, Haddix, Livingston, Bryan, Cantu, Valson, Taraballi, Olsen. Funding acquisition: Fernandez-Moure. Investigation: Fernandez-Moure. Methodology: Fernandez-Moure, Bryan, Olsen, Tasciotti. Project administration: Fernandez-Moure, Tasciotti. Writing—Original draft: Fernandez-Moure, Livingston, Taraballi, Olsen. Writing—Revisions and subsequent drafts: Scherba, Kaplan. Supervision: Olsen, Tasciotti.
Data Availability
Materials, data, and associated protocols are promptly available to readers without undue qualifications in material transfer agreements.
Funding Information
This work was supported by the Americas Hernia Society (Grant# 18200001) as part of the 2011 Research Resident Grant.
Author Disclosure Statement
The authors declare no competing interests.