
Abstract

To the Editor:
D
In this article, we report the case of a patient with acute RAT caused by acute rejection after pulmonary infection who succumbed to the systemic inflammatory response syndrome after PTA was performed.
A 38-year-old woman had undergone kidney transplantation from a deceased donor. Seven months later, on January 17, 2019, she was admitted to the hospital because of pulmonary infection. Computed tomography (CT) scans showed imaging features of acute severe interstitial pneumonia (Fig. 1A). Blood-RT showed normal white blood cell (WBC) counts and neutrophilic granulocyte percentage. The blood urea nitrogen (BUN) was 11.99 mmol/L and creatinine (CR) was 202.2 μmol/L.

Computed tomography (CT) imaging features of the pneumonia in different times. (
Detection of (1,3)-β-D-glucan indicated a fungal infection. Respiratory viruses, Mycoplasma pneumoniae (MP), and Chlamydia pneumoniae (CP) were negative. Therapeutic strategy included immunosuppressant withdrawal, use of antifungal (voriconazole) and antibacterial (imipenem and linezolid) agents, low dose methylprednisolone, as well as respiratory support, nutrition support (2500 Kcal/d), and prescription of a diuretic.
Her respiratory symptoms were improved, and the CT scan showed obviously improved imaging features on January 30 (Fig. 1B). The results of the CT scan on February 6 (Fig. 1C) revealed a much better situation in the lungs, (1,3)-β-D-glucan detection was negative on February 7, BUN was 22.8 mmol/L and CR was 167 μmol/L on February 8.
On February 10, the patient complained of severe oliguria and hematuresis for about four hours; renal duplex ultrasonography detected an absence of blood flow to the allograft kidney. Renal artery angiography revealed complete occlusion in the artery and no distal perfusion (Fig. 2A). Thrombectomy and thrombolysis were performed within six hours from the onset of symptoms, and distal flow was subsequently detected after PTA (Fig. 2B).
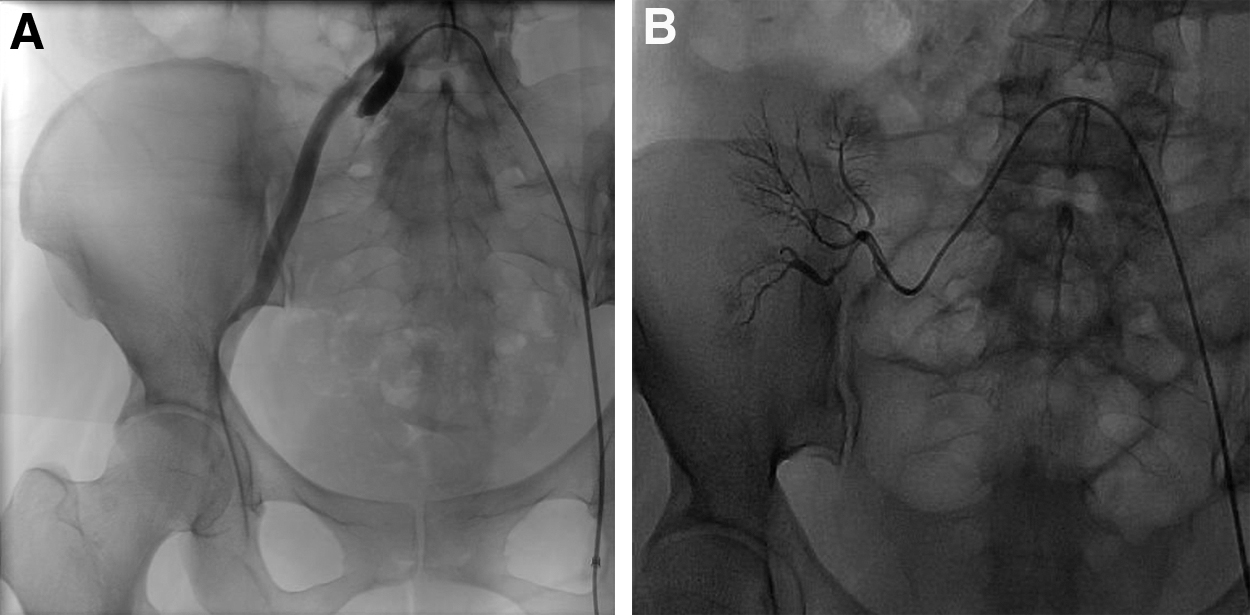
Imaging features of percutaneous transluminal angioplasty (PTA). (
The patient had prolonged high fever from February 11; WBC, red blood cells (RBC), and platelets (PLT) decreased sharply, with the counts of 1.97 × 10^9/L, 2.21 × 10^12/L and 92.00 × 10^9/L, respectively, and presented no response to stimulating factors. The BUN was 81 mmol/L and CR was 830.5 μmol/L on February 12. The WBC count decreased to 0.34 × 10^9/L and procalcitonin (PCT) increased to 200.00 ng/mL on February 14.
On February18, WBC decreased to 0.03 × 10^9/L and PLT decreased to 4 × 10^9/L. On February 23, PCT was 39.21 ng/mL, and interleukin (IL)-6 was 750.4 pg/mL. The patient succumbed to systemic inflammatory response syndrome (SIRS). The results of pathogen culture, including blood, urine, and catheters, were all negative.
This report describes the case of a patient with acute RAT caused by acute rejection after pulmonary infection. The treatment of pulmonary infection was successful, but acute rejection happened because of immunosuppressant withdrawal for 23 days, which had proved to be relatively safe in our experience of the treatment of acute severe interstitial pneumonia.
This was the first death case of artery recanalization in the transplantation RAT population. Compared with the relatively optimistic outcomes of artery stenosis in the transplanted kidney, arterial thrombosis in a transplanted kidney is rarely described, and it is a more serious complication that usually leads to graft loss [6]. A PTA with or without stent placement is a potential treatment option for renal artery stenosis [7], but there were no satisfactory results of artery recanalization in RAT patients [3,4,8,9].
We report a case of acute RAT caused by acute rejection after pulmonary infection. The patient succumbed to SIRS after PTA was performed, which was the worst possible outcome of artery recanalization in these patients.
Most of the data presented and our case report suggest that artery recanalization in transplant RAT patients should be re-evaluated, treatments by PTA or system thrombolysis proved to be invalid and even life-threatening. We suggest that the graft should be removed immediately when complete artery thrombosis is confirmed, especially for the cases caused by acute rejection.
Footnotes
Acknowledgments
We thank the patients and the nurses and clinical staff who provided care for the patients.
The transplantations were performed according to the Declaration of Istanbul, and no executed prisoners were used as donors.
Funding Information
This research was supported by the National Natural Science Foundation of China, Grant No. 81600587 to Zhiping Xia.