
Abstract
Background:
Intra-operative topical vancomycin (VAN) is a strategy used to prevent surgical site infections (SSI). Although evidence supporting efficacy in SSI prevention is evolving, data describing safety, specifically acute kidney injury (AKI), are limited. The purpose of this study was to determine AKI incidence in patients who received intra-operative topical VAN.
Patients and Methods:
This is a retrospective study of adult inpatient encounters in which topical VAN was administered intra-operatively as powder/paste, beads, rods/cement/spacers, or unspecified topical route from February to July 2018. Patients were excluded for AKI or renal replacement therapy (RRT) at baseline or ≤2 serum creatinine (SCr) values post-surgery. The primary outcome was AKI incidence after intra-operative topical VAN, defined as increase in SCr ≥50% or 0.5 mg/dL from baseline or RRT initiation. Secondary outcomes included analysis of AKI risk factors and SSI incidence. Acute kidney injury risk factors were analyzed using multivariable logistic regression.
Results:
Five hundred thirty-four patient encounters met study criteria. Powder/paste were the most common topical VAN formulations (44.8%) with median doses of 2,000 (range, 1,000–26,000) mg. Acute kidney injury incidence was 8.8%. Independent risk factors for AKI were higher Charlson comorbidity index (adjusted odds ratio [aOR], 1.20 [range, 1.06–1.36]), concomitant systemic VAN (aOR, 2.44 [range, 1.29–4.58]), and doubling of total topical VAN dose (aOR, 1.51 [range, 1.13–2.03]).
Conclusions:
The incidence of AKI with intra-operative topical VAN is comparable to reported rates as systemic VAN. Clinicians may consider total topical VAN dose and concomitant systemic VAN to limit AKI incidence with topical VAN use.
Surgical site infections represent a post-operative complication that account for a large disease burden in healthcare [1]. Surgical site infections (SSIs) have been shown to increase hospital length of stay (LOS), re-admission rates, and have an associated cost estimated to exceed $1.6 billion dollars annually in the United States [1]. Historically, administration of systemic antibiotic agents has been the primary strategy to reduce SSIs for surgeries with higher infection risk [2].
The use of intra-operative topical antibiotic agents, specifically vancomycin (VAN), is a strategy that has also been used to reduce SSIs. There are many formulations by which intra-operative topical VAN has been utilized, including being applied as a powder to surgical sites during orthopedic surgeries, as a paste to the sternum during cardiothoracic surgeries, or mixed in antibiotic nails, beads, cement, or spacers during non-spinal orthopedic surgeries [3–5]. The theoretical benefit of topical VAN is achieving high antibiotic concentrations locally with limited systemic exposure and reduced toxicities. Studies showing benefit are limited by retrospective design and heterogeneity of topical VAN dose, application technique, and surgical procedure [6,7]. Because of the lack of evidence demonstrating benefits outweighing harms, to date, the U.S. Centers for Disease Control and Prevention (CDC) guidelines for SSI prevention advises against use of topical VAN [2].
The literature evaluating the safety of intra-operative topical VAN is sparse and conflicting. Reported theoretical concerns of topical VAN include risk of systemic exposure and increased SSI secondary to gram-negative bacteria [8]. Few studies have been published evaluating the risk of acute kidney injury (AKI). Nephrotoxic risk of topical VAN placed in antibiotic spacers for the treatment of prosthetic joint infections (PJI) has been most studied, with AKI incidence ranging between 2% and 17% [9,10]. Independent risk factors that have been associated with AKI in PJI studies in which topical VAN was used include topical VAN dose, topical aminoglycoside dose, concurrent systemic nephrotoxins, obesity, low baseline hemoglobin, and baseline comorbidities [11–13]. This study aimed to evaluate the incidence of AKI associated with the administration of intra-operative topical VAN for inpatients who underwent a surgical procedure(s) at a large academic medical center.
Patients and Methods
Study design
This is a retrospective observational study of patients at the University of Maryland Medical Center, an urban quaternary academic medical center that is equipped with a number of surgical services including orthopedic, cardiothoracic, and trauma. Electronic medical records (EMR) were reviewed for patients with an encounter in which intra-operative topical VAN was administered between February 1, 2018 and July 31, 2018. The study was approved by the University of Maryland, Baltimore Institutional Review Board.
Study population
Patient encounters were included if the patient received topical VAN intra-operatively and were more than 18 years of age. Patients with multiple encounters were included as long as there was a period longer than seven days between the last topical VAN dose and subsequent admission date. The following topical VAN formulations were included in the study: powder, beads, rods, paste, cement, spacers, or an unspecified topical route. Topical formulations were further characterized in categories based on surface area, which has been shown to correlate to topical VAN exposure based on elution time: high surface area (powder, paste), medium surface area (beads - cement or Stimulan®, Biocomposites, Inc., Wilmington, NC), low surface area (cement, spacers and rods - cement or Stimulan®, and unspecified topical route [14,15]. A combination category was included to encompass patients who received more than one type of topical VAN during the encounter. Patients were excluded for the following reasons: (1) topical VAN given as irrigation monotherapy, (2) non-topical route of intra-operative VAN administration, (3) no baseline serum creatinine (SCr) value, (4) AKI at baseline, (5) renal replacement therapy (RRT) at baseline, and (6) fewer than two serum creatinine (SCr) values drawn after surgery. A baseline SCr value was defined as having at least one SCr drawn within 48 hours before or 12 hours after surgery in which topical VAN was given. Where applicable, the baseline SCr was calculated by taking the average of the peak SCr three days before surgery. Baseline AKI was defined as having AKI before surgery comparing SCr values one month before or one week after surgery. Baseline RRT was defined as receiving intermittent hemodialysis (iHD), continuous renal replacement therapy (CRRT), or peritoneal dialysis (PD) before surgery in which intra-operative topical VAN was given.
Study objectives
The primary outcome was the percentage of patients who developed AKI within seven days after intra-operative topical VAN. Acute kidney injury was defined as a new increase in SCr greater than 50% or 0.5 mg/dL from baseline or if RRT initiation. These definitions were adapted from the Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease (RIFLE) criteria and the American Society of Health-System Pharmacists/Infectious Diseases Society of America/Society of Infectious Diseases Pharmacists (ASHP/IDSA/SIDP) vancomycin guidelines [16,17]. Secondary outcomes included analysis of independent AKI risk factors, including concomitant systemic nephrotoxins, intra-operative topical aminoglycosides, number of surgeries, intra-operative blood loss, and number of intra-operative hypotensive episodes. Systemic nephrotoxins included piperacillin/tazobactam, aminoglycosides, loop diuretics, non-steroidal anti-inflammatory drugs (NSAIDs), amphotericin B, polymyxin antibiotics, tacrolimus, cyclosporine, and intravenous contrast. Systemic vancomycin was documented separately from other nephrotoxins and was defined as patients who received a dose of intravenous vancomycin within three days before or seven days after surgery as well as intra-operatively. An intra-operative hypotensive episode was defined as a systolic blood pressure less than 90 mm Hg documented in the anesthesia report. Surgical site infection incidence as per the CDC National Healthcare Safety Network SSI definitions was considered if documented in the EMR within 30 days after the last surgery [18].
Statistical analysis
Patient characteristics were analyzed using descriptive statistics for frequencies, means, and medians. A logistic regression model was performed to measure the association of AKI incidence after adjusting for patient characteristics and known independent risk factors for AKI. Patient characteristics and AKI risk factors were entered as independent variables in the model. Adjusted odds ratios (aOR) with 95% confidence intervals (CIs) were calculated to measure the association of outcomes and effects. Analyses were performed with SAS 9.4 (SAS Institute, Cary, NC).
Results
Study population
A total of 1,165 patients encounters were identified to receive intra-operative topical VAN within the study period. Of these encounters, 534 patients met study criteria (Fig. 1). The mean age of the study population was 59 years (standard deviation (SD) ±16) (Table 1). Thirteen percent of patients were documented to be colonized with methicillin-resistant Staphylococcus aureus (MRSA) at baseline. The median Charlson comorbidity index (CCI) score was two (interquartile range (IQR), 1–4). The most common type of surgery was non-spinal orthopedic surgery (46%) followed by spinal orthopedic surgery (28%). The median total dose of topical VAN given during patient encounters was 2,000 mg (range, 1,000–26,000). Twenty-nine percent of patients (n = 154) received concomitant systemic vancomycin. Twenty-five percent of patients received concomitant intra-operative topical tobramycin at a median dose of 1,200 mg (IQR, 1,200–3,600). The most common formulation of topical VAN administered was high surface area (45%), followed by unspecified topical route (32%).
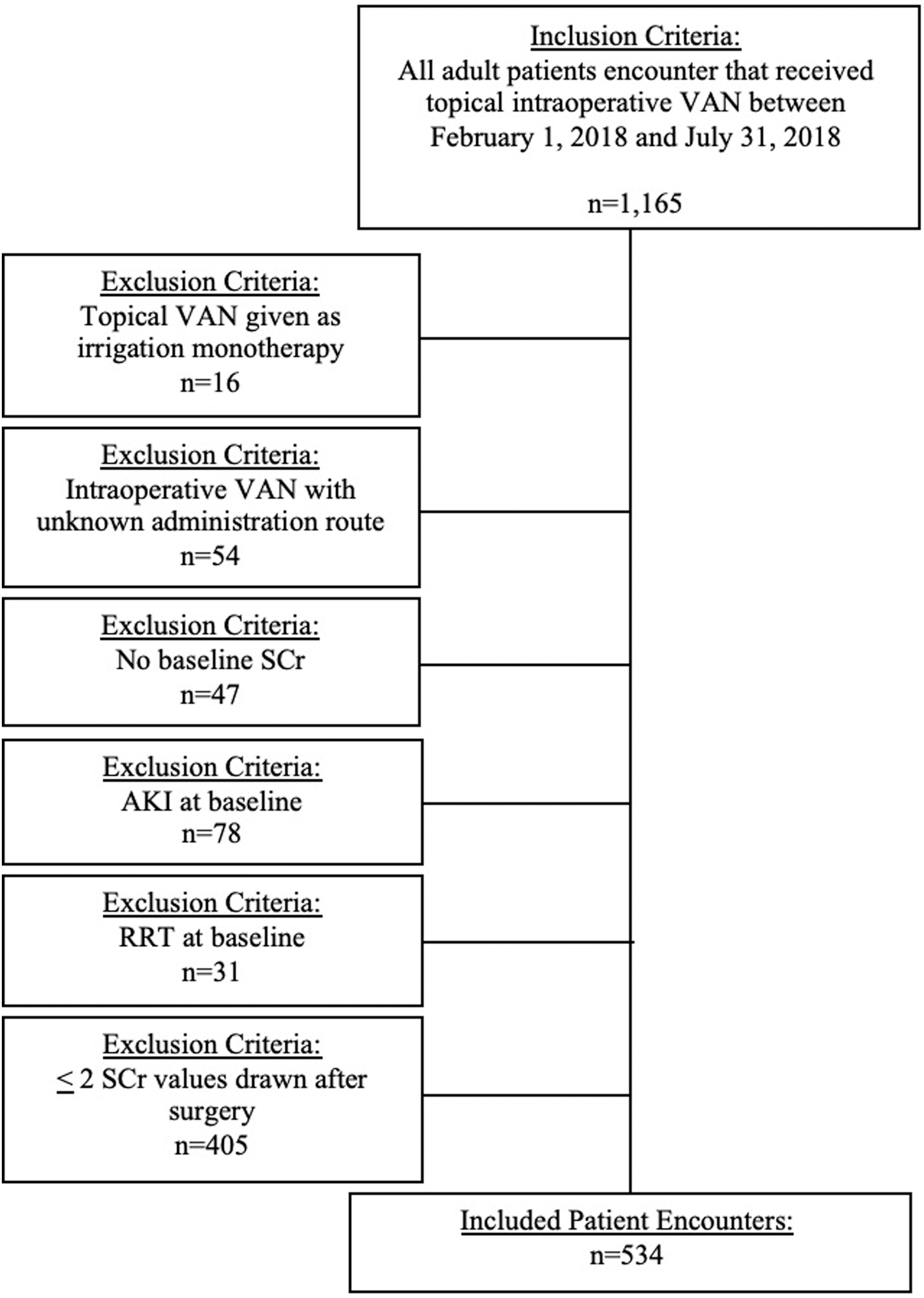
Patient inclusion and exclusion criteria. VAN = vancomycin; SCr = serum creatinine; AKI = acute kidney injury; RRT = renal replacement therapy.
Patient Baseline Demographics and Surgical Characteristics
SD = standard deviation; BMI = body mass index; IQR = interquartile range; MRSA = methicillin-resistant Staphylococcus aureus; CCI = Charlson comorbidity index; MSSA = methicillin-susceptible Staphylococcus aureus; CoNS – coagulase-negative staphylococci; VAN = vancomycin.
Other: Streptococcus spp. (n = 4), anaerobes (n = 3), Enterococcus spp. (n = 3), Candida spp. (n = 2), non-tuberculous mycobacterium spp. (n = 1).
Primary outcome
Forty-seven patient encounters (8.8%) developed AKI after receiving intra-operative topical VAN based on the study definition.
Secondary outcomes
Charlson comorbidity index score, concomitant systemic VAN, and total topic VAN dose appeared to be independent risk factors for AKI in a multivariable logistic regression model (Table 2). Specifically, after adjustment, a one-unit increase in the CCI score increased risk of AKI by 20% (aOR, 1.20 [95% CI, 1.06–1.36]). A patient who received more than one dose of systemic VAN was 2.44 times more likely to develop AKI (aOR, 2.44 [95% CI 1.29–4.58]. In addition, each doubling of the topical VAN dose was associated with an 51% increased risk for developing AKI (odds ratio [OR], 1.51 [1.13 – 2.03] (Fig. 2).
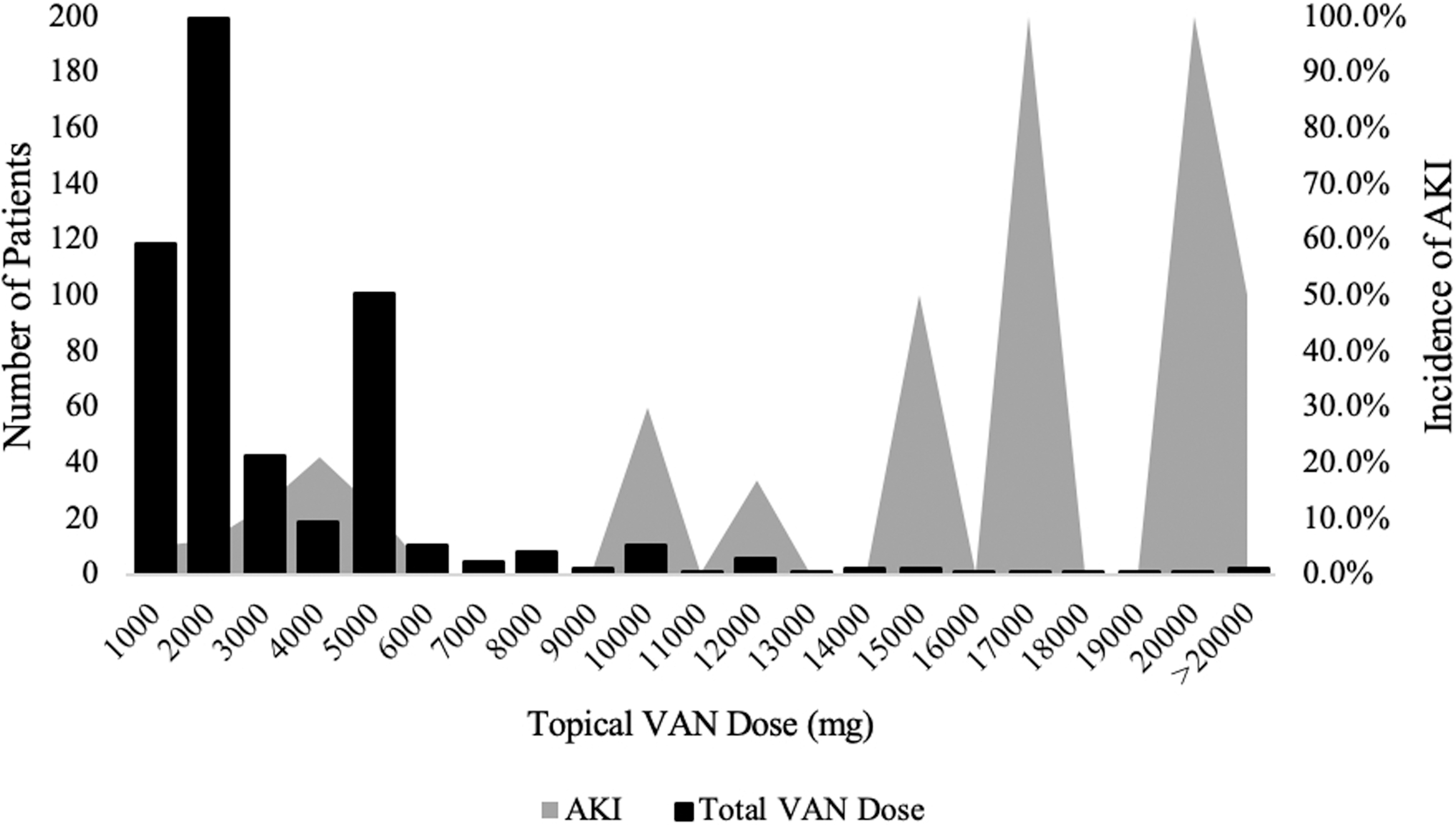
Incidence of acute kidney injury (AKI) based on topical vancomycin (VAN) dose.
Patient Characteristics Associated with Incidence of AKI
Variables entered in the model include: systemic vancomycin administration, dose (mg) topical vancomycin, Charlson comorbidity index.
AKI = acute kidney injury; OR = odds ratio; aOR adjusted odds ratio; CI = confidence interval; VAN = vancomycin; CCI = Charlson comorbidity index; BMI = body mass index; Ref = reference.
High surface area: powder, paste; medium surface area: Stimulan® and cement beads; low surface area: Stimulan® and cement rods, spacers, cement.
The incidence of SSI 30 days post-surgery was 4.1%, with gram-negative organisms being the most common to be isolated from the surgical site (Table 3). The mean length of hospital stay was 11.6 days (SD ±12.8), with the mean intensive care unit (ICU) LOS being 8.2 days (SD ±17.0). The majority of the patients were discharged to a facility at the end of the hospital admission (58.8%).
Patient Outcomes
SSI = surgical site infection; ICU = intensive care unit. MRSA = methicillin-resistant Staphylococcus aureus; MSSA = methicillin-sensitive Staphylococcus aureus; CoNS = coagulase-negative staphylococci.
Staphylococcus spp: MRSA (n = 3), MSSA (n = 1), CoNS (n = 1).
Discussion
For patient encounters that met inclusion criteria in which intra-operative topical VAN was administered, the AKI incidence was 8.8%. This is similar to prior studies reporting AKI incidence with VAN in antibiotic spacers ranging between 2% and 17% [9,10]. This also falls within range of AKI incidence reported in literature for systemic VAN, ranging between 0% and 40% for a variety of patient populations, with higher incidence associated with risk factors such as higher systemic doses and concomitant nephrotoxins [19–22]. Independent patient characteristics associated with AKI with intra-operative topical VAN administration were baseline comorbidities based on CCI score, concomitant systemic VAN, and increased topical VAN doses, which is in line with systemic VAN studies [17]. These findings were observed regardless of the topical VAN formulation or surgical procedure performed.
Clinical studies assessing AKI risk with topical VAN are limited and conflicting. Most literature assessing renal toxicity is because of antibiotic spacers and cement for TKA or THA for treatment of PJIs. A retrospective study of patients (n = 85) that received an antibiotic spacer for TKA reported a 14% AKI incidence. Acute kidney injury was defined as a 50% increase in SCr from baseline within 90 days after surgery. The median time to peak SCr was 30 days. Combined topical VAN (>4,000 mg; OR, 5.97 [1.33–26.72]) and tobramycin doses (>4,800 mg; OR, 5.87 [1.43–24.19]) were associated with increased AKI risk. Unlike the present study, receipt of topical VAN alone or with systemic VAN were not associated risk factors [11]. Conversely, a prospective study in patients who received an antibiotic spacer for a TKA or THA (n = 37) found a 27% AKI incidence. Acute kidney injury was defined by the RIFLE criteria and evaluated up to eight weeks after spacer placement.
Topical or systemic VAN was not associated with AKI risk. Topical VAN doses were not reported in this study [10]. The largest retrospective study (n = 247) evaluating nephrotoxicity associated with spacers for a TKA or THA found an AKI incidence of 26%, as defined by the RIFLE criteria. The mean antibiotic doses used in the spacers were VAN 5,300 g (range, 6,000–18,000 mg) and tobramycin 5,200 g (range, 500–16,400 mg), which are much higher than the present study. A total of 44.9% of patients received concomitant systemic VAN. Topical VAN, topical tobramycin, or systemic VAN were not associated with increased AKI. The only risk factors associated with AKI in this study were obesity, low baseline hemoglobin, and baseline comorbidities [13]. A number of other observational studies and case reports have been published assessing AKI risk with antibiotic spacers, all limited by small population size and heterogeneity among cement type, surgical procedure type, topical VAN doses, and AKI definition [9,23,24].
Risk of AKI has rarely been assessed in other types of topical VAN. Lazar et al. [4] prospectively found that 2,500 mg of topical VAN paste applied to the sternum (n = 36) during cardiac surgery did not lead to persistently elevated serum VAN levels or renal toxicity in conjunction with systemic VAN given for 48 hours. Sweet et al. [7] retrospectively evaluated systemic VAN levels as a secondary outcome for 2,000 mg of topical VAN powder given for various thoracolumbar spinal fusions. Pertinently, unlike the present study, no patients received systemic VAN. Of patients with post-operative VAN levels (n = 178), 20% had a detectable level (mean, 1.6 mcg/mL; range, 0.7–5.9 mcg/mL) on day one after surgery, whereas 6% had a detectable level on post-operative days two and three [7]. A retrospective study of pediatric patients (n = 87) that received 500 mg of prophylactic topical VAN for thoracic and lumbar spine surgery concluded that topical VAN did not increase risk for nephrotoxicity given an insignificant change in SCr between post-operative day one and four. Post-operative vancomycin levels also remained undetectable [25]. Owens et al. [26] retrospectively evaluated use of topical VAN 1,000 mg and tobramycin 1,200 mg for patients with pelvic and acetabular fractures undergoing open reduction internal fixation (n = 140) for SSI prevention. Nephrotoxic risk was evaluated as a secondary outcome. The study found no statistically significant increase in blood urea nitrogen or SCr, however, this was only evaluated 48 hours post-surgery. It is unclear if patients received systemic intravenous vancomycin pre-operatively [26]. Each of these studies had a smaller population size, used lower topical VAN doses, variably received concomitant systemic VAN, and did not include robust definitions of AKI compared with the present study. In addition, these studies do not represent all types of surgery or type of topical VAN.
With topical VAN doses being observed as a substantial AKI risk factor in the present study, it should be noted that there is heterogeneity in the literature regarding optimal doses for SSI prevention. For orthopedic spinal procedures, 1,000–2,000 mg of topical VAN powder has been studied, however, some protocols recommend covering the incision with as high as 6,000 mg reported [8]. Reports of VAN paste dosing ranges between 250 and 2,500 mg [4,27]. In the present study, the mean dose of topical VAN paste was documented to be higher at 5,000 mg. Vancomycin doses placed in spacers have been reported up to 18,000 mg in the literature [13]. Compared with these studies, the mean cumulative dose of topical VAN in the present study was 2,000 mg with a wide range between 1,000 and 26,000 mg, the upper range surpassing the maximum reported in literature.
Surgery alone has been shown to be a risk factor for AKI. Incidence of post-operative AKI ranges between 0.8% and 15.1% [28,29]. Similarly, studies are limited by heterogeneity in type of surgery and AKI definition. Cardiac surgery has particularly been associated with higher risk of post-operative AKI [30]. There are many proposed mechanisms by which surgical patients are at risk for AKI including intra-operative hypotension, dysfunction of microvascular circulation, systemic inflammation, blood loss, and tubular obstruction [29]. The AKI incidence of 8.8% in the present study falls within range of post-operative AKI rates. The present study attempted to capture this through collection of intra-operative blood loss and number of systolic blood pressure decline less than 90 mm Hg. Characteristics, number of surgeries, and surgery types were not associated with increased AKI incidence in the present study. Validity of intra-operative hypotensive episodes and blood loss could be limited by EMR documentation accuracy.
Another controversial safety concern with the use of topical VAN, particularly VAN powder, is the association of SSI incidence with subsequent gram-negative infections [31,32]. Theoretical associations of this are alterations in microbial flora at the surgical site similar to observations with systemic antibiotics. Ghobrial et al. [8] reviewed 981 patients who received VAN powder for spinal surgeries. The SSI incidence with culture growth was 5.2% with 59% of isolates being polymicrobial or gram-negative organisms. The 30-day SSI incidence in the present study was 4.1% with 45% of the cultured isolates being gram-negative organisms or polymicrobial. The number of infections is small, therefore, it is difficult to attribute association of gram-negative infections with topical vancomycin use. The effect of topical VAN on subsequent gram-negative–associated SSI needs to be evaluated in prospective, well-powered studies.
Limitations to the present study include the retrospective design, which relies on accurate and comprehensive medical record documentation. This is applicable regarding formulation and dose of topical VAN administered given that a number of patients did not have these characteristics charted leading to their exclusion from the study. There is heterogeneity in the study for including patients regardless of type of surgical procedure or topical VAN administered. Given the wide acceptance of topical VAN use in the current institution, a comparator group with patients who did not receive topical VAN could not be included. Urine output was decided to not be considered when defining AKI given inconsistencies in documentation across clinical services. Also, many patients were excluded for omission of the minimal SCr laboratory values needed to assess incidence of AKI. Given that this functionally excluded ambulatory and same-day surgical patients, it is likely that the patients in this study represented a group with an inherently higher risk of AKI. In addition, the AKI definition only extended to seven days post-operatively during the admission. It is unknown if patients who received topical VAN with slower elution times could have developed AKI outside of this time frame, as suggested in other studies. In the present study, 38 patients that received either topical VAN beads or rods were noted to have the antibiotic-laden device removed within seven days post-application. It is unclear how much topical VAN these patients were exposed to.
As a result of these uncertainties, the study investigators opted to assume patients were exposed to the full amount. In addition, total systemic VAN doses were not reported. A sub-group analysis was conducted and found that intra-operative VAN only (p = 0.50) and duration of systemic VAN (p = 0.98) was not associated with occurrence of AKI. The majority of patients (n = 95/154) received sustained VAN doses for more than 48 hours. Twenty-eight of these 95 patients received sustained VAN after the procedure, within seven days of the first topical VAN exposure. Per the institution's area under the curve (AUC)-based protocol for vancomycin, patients are typically empirically initiated on 10–15 mg/kg doses with a dosing frequency based on patient renal function. Depending on acuity, patients may receive a one-time 20–25 mg/kg loading dose. Two random VAN levels are obtained within the same dosing interval once patients are at steady state and doses are adjusted to target an AUC of 400 to 600. Because of complexities with reporting systemic VAN doses and inconsistency in collecting levels, the authors opted to report whether patients were exposed to systemic VAN. Further studies investigating systemic VAN exposure from beads and rods over time need to be conducted to better address this.
When utilizing topical VAN intra-operatively, providers may consider concomitant systemic VAN and the topical VAN dose being administered because of potential risk of AKI. Further studies are needed for each type of topical VAN and surgery to evaluate prospectively systemic exposures of intra-operative topical VAN, dose, and effects on accumulation if the patient is already receiving systemic VAN. In addition, although concomitant use was not found to be associated with AKI in this study, the role of topical aminoglycosides should be evaluated further given similar theoretical risk of nephrotoxicity.
Footnotes
Acknowledgments
We thank Dr. Sabeen Ali, PharmD, Xin Gao, PharmD, Rosina Mesumbe, PharmD, and Carly Cheng, PharmD for assistance with data collection and patient chart review.
This study was presented as a poster at ID Week 2019 in Washington, D.C.
Funding Information
The study investigators do not have funding to disclose.
Author Disclosure Statement
The authors do not have any conflicts of interest to disclose.