
Abstract
Background:
Infection is the most frequent complication after severe burns and has a propensity to progress into sepsis then septic shock and multiple organ dysfunction syndrome (MODS). Improving outcomes in acute burn care depends on early detection of infection to allow prompt interventions. Diagnosis of sepsis in severe burns is uniquely challenging because otherwise-typical clinical signs are masked by the hypermetabolic state and systemic inflammation induced by the burn itself. For this reason, burns have historically been excluded from high-impact studies on the diagnosis and treatment of sepsis.
Methods:
This article provides a comprehensive three-fold review of current findings and guidelines pertinent to the early detection of infection and sepsis in severe burns.
Results:
First, evidence-based detection of the most common infections encountered in the burn intensive care unit is reviewed. Second, we analyze the evolution of the diagnostic criteria for sepsis and the evidence regarding their utility in severe burns. Last, we examine the development of biomarkers, from procalcitonin to molecular genomics, for the detection of sepsis.
Conclusions:
Although gold standard methods of early detection of sepsis in burn patients have yet to be identified, improved understanding and appropriate application of the available diagnostic criteria and assays are paramount to providing effective care of patients with severe burns.
Infection leading to sepsis, septic shock, and multiple organ dysfunction syndrome (MODS) is well known as a leading cause of death after severe burns, accounting for 50%–60% of in-patient deaths [1,2]. With the growth of specialized burn units, implementation of fluid resuscitation, and early excision and grafting of burn wounds, the historical trend of early shock-related death after severe burns has transitioned to a trend of death from infection and sepsis after prolonged hospitalization [3,4]. Burned patients are particularly susceptible to wound infections and pneumonia (especially after inhalation injury), which can progress ultimately to sepsis. Establishing a timely diagnosis of sepsis has proved uniquely challenging in the background of the intense hypermetabolic and inflammatory state associated with massive injury, confounding traditional clinical signs of sepsis and greatly hindering the utility of contemporary diagnostic methods. Moreover, frequent fluctuations in the definition of sepsis as well as exclusion of burn patients from landmark studies on sepsis have muddled investigative efforts. In this article, we review the current modalities for the detection of infections and sepsis in severe burns as well as explore why a consensus regarding appropriate diagnostic methods has not yet been achieved.
Detection of Infection
Among patients admitted to the burn intensive care unit (ICU), infection is the most frequent complication. Pneumonia and wound infections are most common and often are nosocomial in origin [5]. For the severely burned, unique considerations must be made during evaluation for possible pneumonia or wound infections.
Pneumonia
Respiratory infections are the most frequently reported infections in burned patients, who have the highest overall rate of ventilator-associated pneumonia (VAP) (7.4%) of all ICU sub-populations. Those with inhalation injury have four times the risk of developing VAP, a state caused by several factors including prolonged mechanical ventilation with endotracheal tubes, systemic immunosuppression, common development of pulmonary edema, and direct pulmonary tissue injury [6]. Specifically, direct tissue injury to the lower respiratory tract predisposes to pneumonia through creation of a pro-infectious microenvironment with massive cytokine secretion and inflammation and subsequent protein-rich fluid secretions, bronchial edema, failure of surfactant production by injured type II pneumocytes, failure of mucous clearance by injured ciliated cells, and formation of bronchial casts from cellular sloughing. These pathophysiologic changes precipitate alveolar collapse, atelectasis, and bacterial growth leading to VAP, which occurs at a rate of 10%–60% after inhalation injury and is the leading cause of death among burn patients with nosocomial infections, who have a VAP mortality rate of 40% [7]. Risk factors for contracting pneumonia include grade 3 (severe) or grade 4 (massive) inhalation injury on fiberoptic bronchoscopy (FOB), increasing burn size (total body surface area [TBSA] burned >20%), PaO2/FiO2 ratio of <300 mm Hg on admission, carboxyhemoglobin concentrations of >10% on admission, and a smoking history [8]. Patients are at highest risk of developing VAP within the first 5 days of mechanical ventilation (estimated at 3% per day) with a steadily declining risk to 2% and 1% per day on days 5-10 and after day 10, respectively [6].
Traditional clinical signs of pneumonia including pulmonary infiltrates on radiographic imaging, fever, leukocytosis, and purulent tracheobronchial secretions have notoriously poor specificity in the diagnosis of VAP. Studies correlating clinical diagnosis of VAP with post-mortem histologic examination and cultures demonstrate a sensitivity and specificity of clinical criteria as only 69% and 75%, respectively [9]. Outside of autopsy, no gold standard exists for the diagnosis of VAP, complicating both treatment and meaningful research.
To address this deficiency, the American Burn Association (ABA) released guidelines for the diagnosis and treatment of VAP in 2009, supporting a microbiologic approach to diagnosis via FOB with sampling of pulmonary flora by bronchioalveolar lavage (BAL), mini-BAL, or protected specimen brush sampling as the recommended diagnostic pathway in patients who have VAP suspected on the basis of clinical findings [10]. Then, in 2018, the International Society for Burn Injuries (ISBI) released practice guidelines (part 2) wherein the clinical and microbiologic diagnoses of pneumonia were defined as noted in Table 1. They affirmed that BAL and subglottic sampling demonstrated equivalency to protected specimen brush sampling in intubated burn patients and are the preferred sampling methods [8].
International Society for Burn Injuries (ISBI) 2018 Diagnostic Criteria for Pneumonia and Wound Infection
Tracheal aspirate with ≥105 organisms, or bronchoalveolar lavage with ≥104 organisms, or protected specimen brush with ≥103 organisms.
Abnormal chest radiograph with uncertain cause and low or moderate clinical suspicion.
Adjacent unburned skin is warm, indurated, erythematous, tender.
+ = present, - = absent, CFU = colony-forming units; T = deep tissues; W = wound.
Bronchoscopic microbiologic diagnosis of pneumonia in burn patients has a sensitivity of 73% ± 18% with a specificity of 82% ± 19%, and direct sampling is postulated also to have therapeutic benefits through mechanical relief of bronchial obstruction by suction of exudates [6]. In fact, patients with inhalation injury who develop pneumonia and undergo FOB have a shorter duration of mechanical ventilation (21 versus 28 days), decreased length of ICU stay (35 versus 39 days) and hospital stay (45 versus 49 days), and a lower total cost of care ($370,572 versus $473,654). However, no statistically significant mortality benefit has yet been demonstrated [7]. It is emphasized that treatment for pneumonia in patients meeting the clinical criteria for diagnosis should not be delayed while awaiting microbiologic confirmation of infection. In the interim, initial antibiotic therapy may be guided by Gram stain results as well as wound culture findings, as the causative organism of pneumonia is found to be identical to organisms isolated from wound cultures in approximately 50% of cases [8].
Wound infection
Immediately after a severe burn the affected skin surface becomes sterilized and remains free of flora for approximately 2 days until flora from adjacent unaffected skin, the naso-oropharyngeal tract, lower gastrointestinal tract, and the environment proliferate over the wound [11]. Burn eschars allow colonization of microorganisms through abundant coagulated protein, elemental co-factors, and protein-rich exudates. The absence of leukocytes in eschar and loss of skin barrier function sets the stage for proliferation of virulent pathogens such as Staphylococcus aureus (both methicillin-resistant and methicillin-sensitive), Pseudomonas aeruginosa, Klebsiella spp., and Acinetobacter baumannii that outcompete other organisms and develop as soon as 5–7 days after injury [12].
Between the 1950s and early 1980s, initial therapy for burn wounds included repetitive submersion hydrotherapy aimed at breaking down eschars and promoting underlying wound bed granulation prior to autografting while simultaneously suppressing infection through application of topical antiseptic agents such as silver sulfadiazine, mafenide acetate, and silver nitrate. In addition to clinical signs of infection such as rapid separation of eschar, foci of eschar discoloration, suppurative secretions, and hematogenous spread of organisms (i.e., ecthyma gangrenosum), the gold standard for wound infection diagnosis during this era was tissue biopsy with histopathologic analysis and quantitative culture; bacterial loads of >105 organisms/g signaled invasive infection best treated with wound excision (Table 1). In 1981, a landmark paper by Woolfrey et al. [13] demonstrated marked discordance of quantitative cultures (44% with a log10 difference of 2 or greater) when specimens were divided into two separate cultures, casting doubt on their utility. Subsequently, early excision and grafting of burn eschars was shown to improve outcomes dramatically in part by preventing wound infections through removal of the nutrient-rich eschar and restoration of skin barrier function. Early excision and grafting have since become widely implemented as standard of care throughout the world.
Of late, wound cultures serve for surveillance of wounds and to acquire qualitative and semi-quantitative data when infection is suspected. In the ISBI 2018 guidelines, wound surfaces should be cleansed with alcohol-based solutions prior to sampling, and sampling should be guided by clinical signs such as formation of exudates, widespread graft loss, or systemic signs of infection. Importantly, surveillance swabs should not guide initiation of antimicrobial therapy; however, they provide useful information about organism susceptibilities that guide decisions regarding antibiotic coverage. Tissue biopsy with quantitative culture and histopathologic analysis retain utility in assessing fungal infections and should be strongly considered when such infection is suspected, as invasive fungal infections can progress rapidly with high rates of death [8].
Detection of Sepsis
The progression of infection to sepsis, septic shock, and MODS remains the leading cause of death in both adult (50%–84%) and pediatric (55%) burn patients [14]. In 2016, the Sepsis-3 criteria defined sepsis as “a life-threatening organ dysfunction caused by a dysregulated host response to infection” [15]. Unlike many other causes of sepsis, its clinical diagnosis in severe burns is nuanced and elusive, clouded by a storm of inflammatory cytokines known as damage-associated molecular patterns (DAMPs) and the pathophysiologic hypermetabolic response they create. This confounding hypermetabolic response mimics systemic inflammatory response syndrome (SIRS) patterns with tachycardia, tachypnea, elevated body temperatures, and leukocytosis, which develop reliably as a pathophysiologic response to large (>40%) TBSA burns and persist for more than a year after injury [16]. The development of diagnostic criteria and assays for the accurate and timely diagnosis of sepsis has been a subject of tremendous investigative effort for more than three decades.
Evolution in sepsis definitions and diagnostic criteria
Prior to 1991, no formal or rigid diagnostic criteria for sepsis existed. To improve the quality of epidemiologic and investigative research, the Society of Critical Care Medicine and the American College of Chest Physicians developed a definition now known as Sepsis-1 (Table 2) [17]. Ten years later, Sepsis-2 expanded SIRS to include a vast array of possible parameters with infection only documented or suspected, with the openly stated aim of improving bedside diagnosis rather than facilitating precise parameters amenable to investigative efforts [18,19].
Evolution of Adult Sepsis Diagnostic Criteria and Definitions
aPTT = activated partial thromboplastin time; AMS = altered mental status; BG = blood glucose; CI = cardiac index; CNS = central nervous system; Cr = creatinine; CRP = C-reactive protein; FiO2 = fraction of inspired oxygen; GCS = Glasgow Coma Scale; HR = heart rate; INR = International Normalized Ratio; MAP = mean arterial pressure; PCT = procalcitonin; PaO2 = arterial partial pressure of oxygen; PLT = platelets; SBP = systolic blood pressure; SIRS = systemic inflammatory response syndrome; SOFA = Sequential Organ Failure Assessment; SVO2= mixed venous oxygen saturation; T = temperature; TBSA = total body surface area; UOP = urine output; VR = ventilatory rate; WBC = white blood cell count.
Either documented or suspected.
No discrete number of symptoms was published; the stated goal was to facilitate bedside diagnosis instead of creating standardized diagnostic criteria [19].
Defined as SBP <90 mm Hg or reduction in SBP ≥40 mm Hg.
Although MODS and the Sequential Organ Failure Assessment (SOFA) score were referenced directly by Sepsis-2, the focus of the definition rested on SIRS and identification of infection. Importantly, the clinical studies of sepsis on which these definitions and criteria were constructed excluded burned patients [1,8].
In 2007, the ABA convened 23 experts to devise consensus definitions specific to burn sepsis, arguing that the Sepsis-2 criteria were too inclusive to be applicable to severe burns and did not account for the hypermetabolic state. It made several changes as defined in Table 2, notably the presence of a large burn (>20% TBSA), establishment of higher thresholds of SIRS parameters, abandonment of severe sepsis, and addition of thrombocytopenia, hyperglycemia, and intolerance of enteral feeding as triggers for concern [20]. Furthermore, emphasis was placed on burn sepsis being defined as a change in patient status.
A subsequent retrospective study by Mann-Salinas et al. evaluated the effectiveness of the ABA criteria in adult burn patients and found that they were predictive of sepsis one day prior to the drawing of blood for culture with an area under the receiver operator curve (AUROC) of 0.619. Using a statistical regression model, they were able to define six sepsis predictors that improved the AUROC to 0.775 but which did not prove to be accurate in prospective studies [21,22].
Again in 2016 as a product of the Surviving Sepsis Campaign, Sepsis-3 guidelines revised the definitions, abolishing SIRS and severe sepsis and incorporating host organ response into the definition. The SOFA was formally incorporated, with a score of 2 or greater requisite for diagnosis [15]. Despite Sepsis-3, the ISBI practice guidelines published in 2018 afterward re-affirmed the previously instituted ABA consensus definitions as standard of care in burn patients [8]. Ironically, a prospective study by Yan et al. [22] published the same year compared the predictive value of ABA criteria, the aforementioned Mann-Salinas criteria, and Sepsis-3 in adult burn patients, discovering that they correctly predicted sepsis in 59%, 28%, and 85% of patients, respectively, at 48 hours prior to clinical diagnosis of sepsis. Although at this time the evidence most supports Sepsis-3 for the reliable diagnosis of burn sepsis, this has not been formally embraced in treatment guidelines and remains to be corroborated.
Serum biomarkers investigated for early detection of sepsis
The lack of robust clinical criteria capable of timely and specific diagnosis of burn sepsis as well as the magnitude of clinical impact imparted by early treatment has triggered a massive undertaking to search for methods for the early detection and diagnosis of sepsis. A wide spectrum of inflammatory and molecular serum biomarkers identifiable early in the course of infection has already undergone investigation (Fig. 1) [23]. The following are notable examples of candidate serum biomarkers.
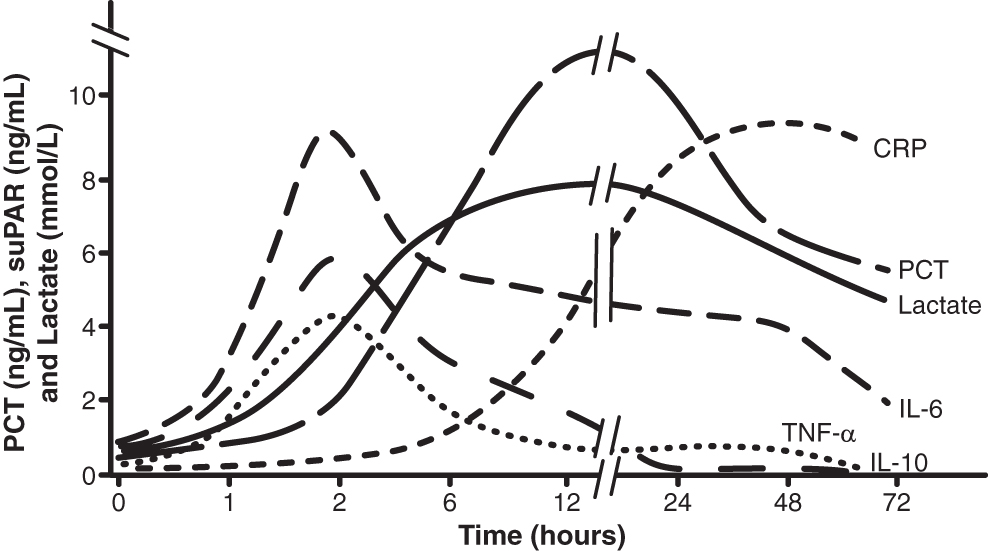
Time course of sepsis biomarker elevation after pathogen exposure. Borrowed and modified with permission from University of California Davis Department of Pathology [23]. CRP = C-reactive protein, IL-6 = interleukin 6, IL-10 = interleukin 10, PCT = procalcitonin, TNF-α = tissue necrosis factor alpha.
Procalcitonin
Procalcitonin (PCT) is a serum protein with considerable potential for use in the detection of sepsis in patients with severe burn injuries. Measurement of PCT has gained attention in the critical care setting because of its notably consistent correlation with the course of bacterial infection. It is an endocrine hormone of the thyroid gland and precursor to calcitonin that plays an indirect role in calcium metabolism and has undetectable serum concentrations under normal conditions. However, during a systemic inflammatory response and in the presence of microbial endotoxin, it is released into the circulation by non-endocrine tissues including the lung, kidney, and omentum [24]. Unlike other serum biomarkers, the utility of PCT lies in its responsiveness to both inflammatory mediators and bacterial lipopolysaccharide (LPS) [24,25]. Similarly, fungal toxins elicit an increase in PCT, but to a lesser extent than bacterial LPS because of activation of an alternative cytokine response involving interferon (IFN)-γ [26]. Although PCT is useful in the detection of bacterial and fungal infections, its measurement is limited in detecting viruses, likely because of the highly potent viral inhibition of tumor necrosis factor (TNF)-α by IFN-γ, effectively suppressing measurable PCT.
With regard to bacterial sepsis, a meta-analysis in 2019 by Kondo et al. [27] showed an AUROC of 0.84 with a pooled sensitivity of 80% and specificity of 75% (Table 3). Although a sizable proportion of the literature acknowledges PCT's diagnostic accuracy in early detection of bacterial sepsis in the critically ill, its clinical utility has been called into question. Notably, Jensen et al. [28] in 2011 published the results of the Procalcitonin and Survival Study (PASS) randomized clinical trial, which recruited 1,200 critically ill patients to evaluate the effectiveness of PCT-guided early antibiotic therapy in improving sepsis survival. This strategy yielded an absolute risk reduction of 0.6% contrasted with the standard of care, which was not statistically significant.
Accuracy of Serum Biomarkers for Detection of Sepsis in Burn Injury
CRP = C-reactive protein; IL = interleukin; mRNA = messenger RNA; N = no; NR = not reported; PCT = procalcitonin; RT-PCR = reverse transcriptase polymerase chain reaction; TNF-α = tumor necrosis factor; Y = yes.
Nonetheless, mounting evidence exists for the diagnostic value of PCT in the care of burned patients. The relation between PCT and sepsis has been explored throughout the past three decades, and studies continue to report evidence in favor of PCT's diagnostic utility in burn patients. One such investigation assessed the diagnostic capabilities of PCT compared with C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and white blood cell (WBC) count. Not only was PCT found to have excellent diagnostic accuracy in the prediction of infection, but it also was the only serum marker that displayed an observable difference between septic and non-septic cases [29]. Two recently completed meta-analyses demonstrated findings in burn sepsis largely consistent with each other and earlier works, with an AUROC of 0.92 [30] and 0.83 [31]. Furthermore, a later study determined that elevated serial measurements of PCT during the first five days after burn injury were strongly associated with the development of sepsis [32]. In addition to its diagnostic ability, contrasting concentrations of PCT may be able to help distinguish gram-negative from gram-positive bacterial infection, with significantly higher concentrations indicating gram-negative infections [33].
C-Reactive Protein
C-reactive protein (CRP) is a thoroughly studied acute-phase reactant and serum biomarker of inflammation that is produced primarily in the liver and upregulated by interleukin-6 (IL-6) [34]. Its concentration correlates strongly with burn size, and higher concentrations tend to be found in women and non-survivors [35]. Beyond these findings, its utility for the detection of sepsis is not supported, as demonstrated in a meta-analysis of nine studies published in 2018 by Tan et al. [36], reporting a sensitivity of 0.80 and specificity of 0.61. Jeschke et al. [35] carried out the largest cohort study to date specifically for sepsis detection in burned patients, with a total of 918 pediatric enrollees included in the analysis. The investigation confirmed that CRP was unable to predict sepsis at any change in threshold between 0 and 20 mg/dL. Although widely available, its use is not recommended in routine burn critical care.
Interleukins 6, 8, and 10
Interleukin (IL)-6 is a major acute-phase reactant released by T cells and macrophages at the site of injury, and its utility in the diagnosis of infection has been well studied [37,38]. In a meta-analysis of 20 studies on adults with SIRS, IL-6 was determined to be of diagnostic value comparable to that of PCT in its ability to detect sepsis, with IL-6 having a pooled sensitivity of 0.68 and specificity of 0.73 [38]. In burned patients, patterns of elevated concentrations are biphasic, peaking at both early and late time points after severe burns. Monitoring for persistently high concentrations of IL-6 may raise suspicion of upcoming sepsis in patients with burns [39]. However, IL-6 remains questionable in its clinical utility for the detection of sepsis. Tsalik et al. [40] studied a cohort of 336 adults with suspected sepsis, and IL-6 was demonstrated to have an insignificant value in discriminating between severity of infection compared with PCT and CRP.
Interleukin-8 is a pro-inflammatory cytokine that is notably released during the acute period of injury and acts as a potent attractant for neutrophils, promoting their migration into the affected area [41]. Investigations have highlighted a clinical value in IL-8 that is primarily prognostic rather than diagnostic, in which a relation exists between its serum concentration and the likelihood of sepsis and survival. In a large cohort study by Kraft et al., IL-8 was measured in 468 pediatric burn patients with TBSA of >30%, in which concentrations above a threshold of 234 pg/mL indicated a higher likelihood of multiorgan dysfunction, sepsis, and death [42]. Persistently elevated IL-8 correlates with a poorer prognosis and high possibility of infection in burn patients [39].
Interleukin-10 mediates the immune response to infection, primarily inhibiting inflammatory activities of macrophages and Th1, NK, and B cells in an attempt to downregulate the pro-inflammatory state [43]. Assessment of IL-10 in isolation from other serum biomarkers has limited utility, yet it may provide further insight into the prognostic trajectory of burn injury and sepsis. Similar to findings in IL-8, burn patients who develop sepsis tend to have remarkably higher concentrations of IL-10, which remain elevated for as long as 14 days after injury and into the development of infection [44,45].
Tumor Necrosis Factor-α
During the acute period after a severe burn, macrophages on location participate in the immune response by secreting tumor necrosis factor (TNF)-α which upregulates the activity of pro-inflammatory cytokines [46]. Because TNF-α also is released after infection, studies have explored its value in the recognition of sepsis. Significantly elevated concentrations of TNF-α were measured in burned patients at the time of admission, with a second elevation of TNF-α occurring later in the hospital course [44,46]. Subsequent studies reported that lower ratios of TNF-α to IL-10 were highly predictive of repeated episodes of infection and were correlated inversely with burn size [47]. However, the utility of TNFα in the detection of sepsis still is limited because of conflicting data in some populations. For example, TNF-α concentrations do not become elevated in elderly patients regardless of sepsis development during the first 30 days after the burn, which may be related to a latent or impaired host immune response [48].
Molecular Markers
In recent years, emerging interest has developed for cellular and molecular laboratory techniques in the detection of sepsis in burned patients based on encouraging findings in the fields of genomics and transcriptomics. By using widely available genomics assays to identify sets of relevant genetic markers, these tools may provide highly accurate and reliable means of early recognition of sepsis. For example, carriers of particular alleles relating to expression of interleukins, TNF-α, and Toll-like receptor 4 have a higher risk of sepsis and death after severe burns [49–51].
Epigenetic processes, such as DNA methylation and histone modification, may also be useful in early detection of sepsis and can specify the bacterial etiology [52]. Studies on transcribed mRNA and smaller, non-coding microRNA that are involved in the pro-inflammatory state indicate the potential of a diagnostic pattern for identifying sepsis. One study measured expression of a panel of seven cytokine genes using real-time reverse transcriptase polymerase chain reaction together with non-linear neural network analysis and demonstrated that they could predict sepsis accurately as early as four days prior to onset with a sensitivity and specificity of 91.4% and 80.2%, respectively [53]. Proteomics and metabolomics are two additional fields of analysis where pattern recognition and molecular expression can be utilized for sepsis recognition.
Conclusions
Early intervention is critical to improve outcomes of sepsis, but early treatment necessitates early detection. Despite the existence of criteria specific for burn sepsis published by the American Burn Association, they have not been reliable in prospective studies beyond the contemporary Sepsis-3 criteria. Investigation of serum biomarkers of sepsis also has yet to produce a gold standard or widely implemented assay. Hope persists that reliable criteria and assays will be identified for the early detection of burn sepsis. Meanwhile, a thorough understanding and appropriate application of the available diagnostic criteria and assays are paramount in providing care of severe burns.
Footnotes
Acknowledgments
We thank Dr. Nam K. Tran and the University of California Davis Department of Pathology for allowing us to reproduce a modified version of Figure 1 [![]() ].
].
Author Disclosure Statement
The authors have no disclosures related to this article.