
Abstract
Background:
Treatment of biliary infection in liver transplant (LT) recipients is a challenge, especially because of ineffectiveness of the antibiotic agents otherwise recommended for non-transplant populations. We aimed to understand the factors underlying the choice of antibiotic therapy.
Patients and Methods:
A total of 373 bile cultures from LT recipients with biliary complications (n = 127; LT group) and from a non-transplant population that underwent cholecystectomy for acute cholecystitis (n = 246; non-transplant group) between January 2009 and December 2018, were investigated.
Results:
Polymicrobial cultures (13.4% vs. 1.6%; p < 0.001), Enterococcus faecium (26.0% vs. 8.5%; p < 0.001), and Pseudomonas (13.4% vs. 4.1%; p = 0.001) in the LT group, and non-faecium enterococci (3.9% vs. 18.3%; p < 0.001) and Enterobacteriales (40.2% vs. 54.9%; p = 0.007), especially Escherichia (11.0% vs. 29.7%; p < 0.001), in the non-transplant group, showed higher abundance. Most of the antibiotic agents recommended as initial antibiotic therapy for the non-transplant population as per previous guidelines were not effective in LT recipients. The incidences of Enterococcus faecium (14.9% vs. 32.5%; p = 0.029) in the LT recipients with model for end-stage liver disease (MELD) score >12 and non-faecium enterococci (8.5% vs. 1.3%; p = 0.042) in those with MELD score ≤12 were higher than those in the other group. The incidence of Enterobacteriales increased over time after LT (p = 0.048) and was similar to that in the non-transplant group after one year of LT. Bile micro-organisms in LT recipients, resistant to most antibiotic agents, especially soon after LT changed over time and became similar to those in the non-transplant group after one year of LT.
Conclusions:
Antibiotic therapy for biliary infection in LT recipients should be different from that in non-transplant populations, considering clinical factors such as the time interval after LT and MELD score.
Biliary complication remains one of the most common challenges after living-donor liver transplant (LT); it often leads to biliary infection, which is a major cause of morbidity and mortality in LT recipients [1,2]. In case of biliary infection, treatment based on disease etiology is important to control the infection effectively [3]. Bile leakage or biliary stricture is treated by percutaneous drainage or endoscopic manipulation with or without stent insertion [4]. In conjunction with these methods, effective antibiotic administration is essential for surgical infection prophylaxis. Antibiotic therapy plays several roles. First, it limits local inflammation and systemic septic response [5] and second, it prevents not only procedure-related surgical site infections from a superficial wound into the organ space, but also intra-hepatic abscess formation [6]. Last, it allows the recipients to undergo an elective rather than an emergency procedure [5,6].
Biliary infection in LT recipients might differ from that in a non-transplant population for several reasons. Bactobilia may occur more frequently in LT recipients than in non-transplant patients, thereby increasing their risk of infection [7]. Signs and symptoms of infection in LT recipients, including abdominal pain and fever, can be subtle because of the administration of immunosuppressive drugs, which may delay diagnosis and increase the risk of disease progression to bacteremia [8]. Bile microbiology and antibiotic resistance in LT recipients might change because of their recurrent exposure to antibiotic agents to avoid complications of cirrhosis, such as spontaneous bacterial peritonitis and peri-operative infection prophylaxis. In fact, multi-drug–resistant (MDR) pathogens, such as extended-spectrum β-lactamase (ESBL)-positive Enterobacteriales, carbapenem-resistant Enterobacteriales (CRE), carbapenemase-producing Enterobacteriales (CPE), and vancomycin-resistant enterococci (VRE), are detected more often in LT recipients than in the non-transplant population [9,10].
Effective antibiotic agents should be administered as early as possible to achieve successful infection control, especially in LT recipients who are vulnerable to severe infections, such as bacteremia [11]. However, accurate identification of the causative organism and analyses of their antibiotic resistances require a long time, because a bile sample is obtained only after biliary intervention and its microbial assessment requires at least 48 hours for cultivation. Bile microbiology and related antibiotic resistance in LT recipients with biliary infection is an understudied area, and antibiotic agents recommended for non-transplant population are currently administered to LT recipients, despite their frequent ineffectiveness in controlling the infection. Therefore, knowledge of the bacteria most likely to cause infection and of the local resistance spectrum of such bacteria would be vital for an appropriate antimicrobial therapy. In this study, we compared bile microbiology and antibiotic resistances between LT recipients and a non-transplant population. Subgroup analysis of the LT group was conducted further to investigate the differences based on several important clinical variables.
Patients and Methods
A total of 373 positive bile cultures, including poly-microbial infection from 352 patients with biliary infection, who were hospitalized from January 2009 to December 2018 at multiple centers were analyzed. The patients from whom bile cultures were collected were divided into the following two groups: the LT group that underwent biliary drainage, including percutaneous drainage (PCD) or percutaneous trans-hepatic biliary drainage (PTBD) after LT because of biliary complications without any vascular problem (n = 127, from 110 patients), and the non-transplant group that underwent cholecystectomy because of acute cholecystitis according to the Tokyo Guidelines 2018 [5] (n = 246, from 242 patients).
All positive bile cultures were reviewed, and the incidence of each micro-organism and its antibiotic resistance was compared between the groups. Furthermore, subgroup analysis of the LT group was performed such that differences in biliary flora and antibiotic resistances, based on peri-operative antibiotic regimen and its duration, the model for end-stage liver disease (MELD) score that represents acuity of the patient, time interval after LT, transplant centers, history of spontaneous bacterial peritonitis (SBP), method of biliary reconstruction, type of biliary complication including bile leakage or biliary stricture, and patients presenting with or without infectious symptoms, could be analyzed.
This study was approved by the Institutional Review Boards of three hospitals (Chung-Ang University Hospital [CAU 1911-016-16289], Seoul National University Bundang Hospital [B-2001-586-102], and Soonchunhyang University Bucheon Hospital [SCHBC 2019-11-017-002]) and was exempted from the requirement of obtaining informed consent from participants because of its retrospective nature and because no identifiable patient data were used. No organs from executed prisoners were used in this study.
Liver transplant group
The peri-operative antibiotic regimens at the transplant centers were similar, with ampicillin-sulbactam being used mainly for seven days after LT, based on the condition of patients. Immunosuppressive therapy after LT was similar across the transplant centers, being based on the combination of calcineurin inhibitors (cyclosporine or tacrolimus), mycophenolate mofetil (MMF), and a corticosteroid. The corticosteroid was tapered to zero within six months of LT. All patients had prolonged prophylaxis for Pneumocystis jiroveci pneumonia (PJP) with trimethoprim-sulfamethoxazole (TMP-SMX) over six months after LT. None had prophylaxis for nocardiosis in this study. All bile samples were collected after the administration of antibiotic agents, such as carbapenem (43.3%), piperacillin-tazobactam (35.4%), ciprofloxacin (9.4%), ceftriaxone (7.1%), and others (4.7%) for less than one day (89.8%), mostly before biliary intervention. Patients who underwent biliary manipulation or surgical revisions before sample collection were excluded from this study.
Non-transplant group
Pre-operative antibiotic agents, including ceftriaxone (56.5%), ciprofloxacin (40.7%), carbapenem (1.6%), and piperacillin-tazobactam (1.2%) were administered before collection of bile samples for 0 to 15 days (within three days, 67.6%), considering liver function suitable for general anesthesia. Patients who had undergone endoscopic retrograde cholangiopancreatography (ERCP) or biliary surgery prior to sample collection were excluded from this study.
Cultures and antibiotic susceptibility tests
Bile juice was swabbed in an aseptic manner immediately after percutaneous surgical procedures in the LT group or retrieval of gallbladder specimens during operation in the non-transplant group, for microbial assessment. The specimens were then inoculated onto blood agar, chocolate agar, and MacConkey agar. The specimens were cultivated at 37°C in a 5% carbon dioxide aerobic chamber, and then inoculated in phenylethanol blood agar and cultivated for 48 hours in a Forma Anaerobic Chamber (MACS-MG-500 Anaerobic Workstation; Don Whitley Scientific, West Yorkshire, UK). All colonies that formed after 48 hours were identified and tested for antibiotic susceptibility using the VITEK2 system (bioMerieux Vitek Inc, Durham, NC). Antibiotic susceptibilities were reported as three classes: susceptible (S), when poor bacterial growth was detected, indicating the use of correct antibiotic agents; indeterminate (I), when bacterial growth was partially inhibited, indicating the use of potentially inappropriate antibiotics; and resistant (R), when bacterial colonies continued to grow despite the presence of otherwise effective antibiotic agents.
Statistical analysis
For intergroup comparisons, the distribution of data was first evaluated for normality using the Shapiro-Wilk test. Normally distributed data are presented as mean ± standard deviation; inter-group comparisons were conducted using the Student t-test or Kruskal-Wallis test. Inter-group comparisons of descriptive data were conducted using the χ2 test or Fisher exact test. Test for trends was performed using linear-by-linear association. Statistical analyses were conducted using SPSS 19.0 (IBM Corp, Armonk, NY).
Results
Demographics
On average, the patients were younger in the LT group (56.4 ± 8.5 years) than in the non-transplant group (65.3 ± 14.5 years; p < 0.001). Most were male in both groups (75.5% vs. 55.8%; p = 0.001). Initial laboratory findings showed total bilirubin (TB; 4.1 ± 4.6 vs. 1.9 ± 1.8 mg/dL; p < 0.001), direct bilirubin (DB; 2.9 ± 3.3 vs. 1.1 ± 1.4 mg/dL; p < 0.001), and alkaline phosphatase (ALP; 411.1 ± 306.1 vs. 238.0 ± 221.5 IU/L; p < 0.001) in LT group, and white blood cell (WBC) count (6,323 ± 4,220 vs. 12,930 ± 4,713 per microliter; p < 0.001), aspartate aminotransferase (AST; 62.3 ± 84.4 vs. 166.4 ± 302.1 IU/L; p < 0.001), and alanine aminotransferase (ALT; 73.1 ± 161.7 vs. 133.9 ± 219.9 IU/L; p = 0.005) in non-transplant group to be elevated substantially. Hepatitis B virus-related liver cirrhosis (36.4%) was the most common indication in the LT group, followed by alcoholic liver cirrhosis (19.1%) and hepatocellular carcinoma (15.5%). In the non-transplant group, most patients had acute cholecystitis grade II (81.7%). Most LT recipients had received a living-donor right hemi-liver graft (90.0%) with a single bile duct (75.5%), mean size of the graft bile duct (minimum) being 4.9 ± 2.5 mm. Biliary stricture (79.1%) was more common than bile leakage (20.9%) and most of the bile cultures were obtained from percutaneous trans-hepatic biliary drainage; (PTBD; 94.5%). The median duration to bile culture after LT was 7.9 (0.9–92.2) months. Initial laboratory findings for LT recipients showed elevated serum levels of TB, DB, AST, ALT, and ALP, with a normal range of WBC counts (Table 1).
Clinical Characteristics of Liver Transplant Recipients and Non-Transplant Population
LT = liver transplant; WBC = white blood cell count; TB = total bilirubin; DB = direct bilirubin; AST = aspartate aminotransferase; ALP = alkaline phosphatase; ALT = alanine aminotransferase; GGT = γ-glutamyltransferase; HBV = hepatitis B virus; HCV = hepatitis C virus; PTBD = percutaneous transhepatic biliary drainage; PCD = percutaneous drainage.
Bile microbiology between the groups
The incidence of micro-organisms comprising poly-microbial cultures was increased substantially in the LT group than in the non-transplant group (13.4% vs. 1.6%; p < 0.001). There was no difference in the incidences of gram-positive micro-organisms (37.8% vs. 35.8%; p = 0.701), gram-negative micro-organisms (60.6% vs. 63.8%; p = 0.546), and fungi (1.6% vs. 1.2%; p = 0.777) between the groups (Fig. 1A). Among the gram-positive micro-organisms, enterococci were mostly isolated from both the groups, with no difference in their incidence between the LT and non-transplant groups (29.9% vs. 26.8%; p = 0.528). Among gram-negative micro-organisms, Enterobacteriales in the non-transplant group (40.2% vs. 54.9%; p = 0.007), and non-fermentative gram-negative bacilli in the LT group (20.5% vs. 8.9%; p = 0.002) were more common than in the other group (Fig. 1B). Among enterococci, the incidence of Enterococcus faecium in the LT group (26.0% vs. 8.5%; p < 0.001) and non-faecium enterococci in the non-transplant group (3.9% vs. 18.3%; p < 0.001) was more common. Among Enterobacteriales, the incidence of Escherichia was higher in the non-transplant group than in the LT group (11.0% vs. 29.7%; p < 0.001). Klebsiella in the LT group (18.1% vs. 11.8%; p = 0.095) and Enterobacter in the non-transplant group were more frequent (5.5% vs. 8.9%; p = 0.241), although the difference was not significant. Among the non-fermentative gram-negative bacilli, members from the genus Pseudomonas were mostly isolated and were more common in the LT group than in the non-transplant group (13.4% vs. 4.1%; p = 0.001) (Fig. 1C).
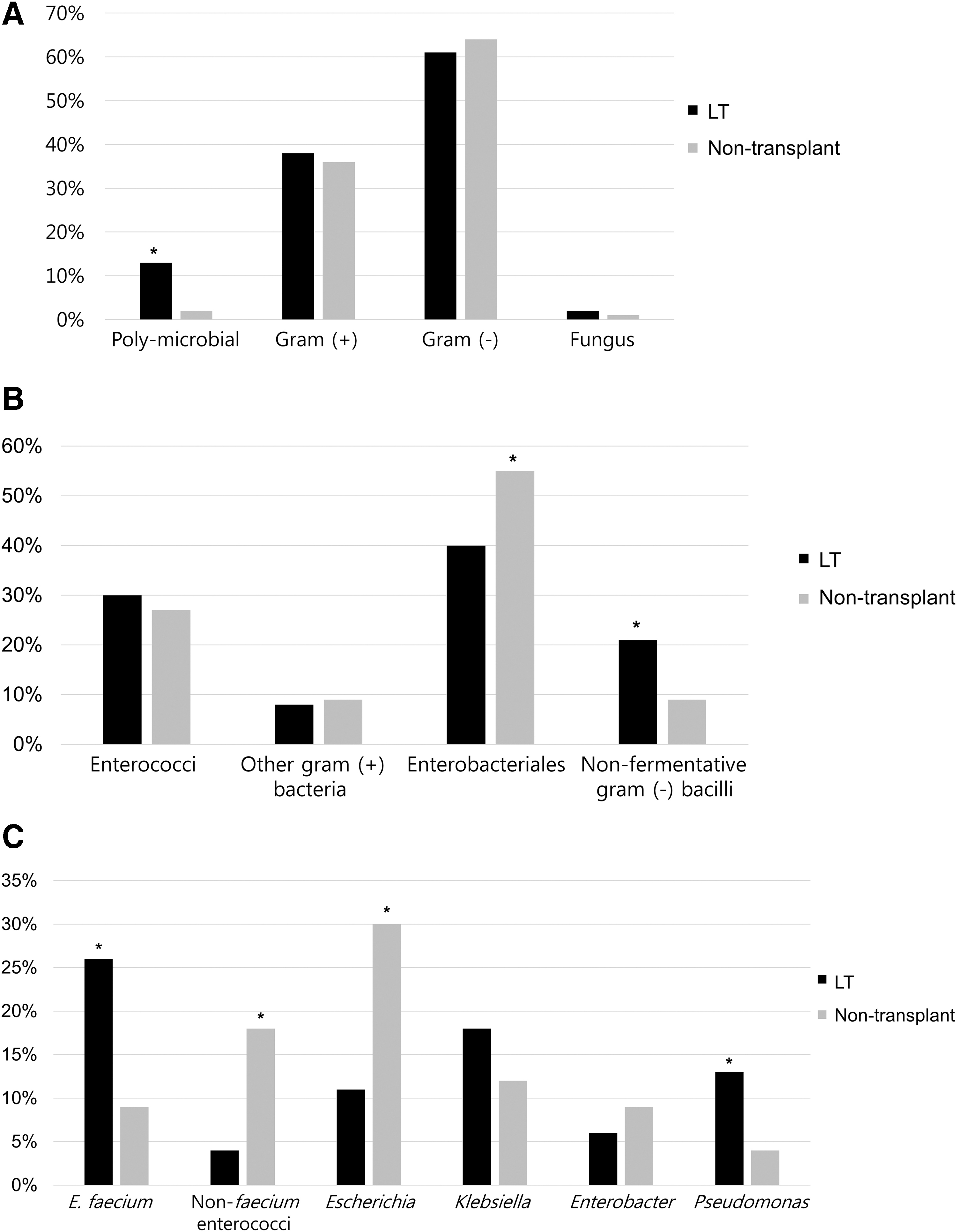
Differences of bile micro-organisms between the liver transplant (LT) group and non-transplant group. (
Poly-microbial cultures between the groups
The micro-organisms comprising poly-microbial cultures are summarized in Table 2; the most common ones being enterococci and Enterobacteriales in the LT group (47.1%) and non-transplant group (50.0%). In the LT group, combination of Enterococcus faecium and Enterobacteriales (35.3%) was most commonly isolated, followed by combinations of Pseudomonas and Enterobacteriales (17.6%) and Enterococcus faecium, Pseudomonas, and Enterobacteriales (17.6%). In the non-transplant group, combinations of non-faecium enterococci and Enterobacteriales (25.0%) or Pseudomonas (25.0%), Enterococcus faecium, and Enterobacteriales (25.0%), and Enterobacteriales (25.0%) were equally isolated (Table 2).
Poly-Microbial Isolates in the Liver Transplant and Non-Transplant Groups
LT = liver transplant.
Antibiotic resistances between the groups
Antibiotic resistance of each micro-organism was increased in the LT group than in the non-transplant group. Vancomycin-resistant Enterococcus faecium (VREFM; 23.1% vs. 6.7%; p = 0.216) and penicillin-resistant non-faecium enterococci (PRNEFM; 25.0% vs. 15.8%; p = 0.638) were more abundant in the LT group than in the non-transplant group; however, the increase was not significant (Fig. 2A). Resistance of Enterobacteriales to ceftriaxone (61.3% vs. 19.5%; p < 0.001), cefepime (71.4% vs. 10.2%; p < 0.000), piperacillin-tazobactam (37.9% vs. 6.4%; p < 0.001), and carbapenem (14.9% vs. 2.2%; p = 0.001) was increased in the LT group than in the non-transplant group. The abundances of ESBL-producing Enterobacteriales (21.6% vs. 0.7%; p < 0.001) and CPE (3.9% vs. 0%; p = 0.021) were also substantially higher in the LT group than in the non-transplant group (Fig. 2B). Ceftazidime-resistant Pseudomonas (50.0% vs. 18.2%; p = 0.041) and cefepime-resistant Pseudomonas (58.3% vs. 22.2%; p = 0.044) were substantially more abundant in the LT group than in the non-transplant group (Fig. 2C).
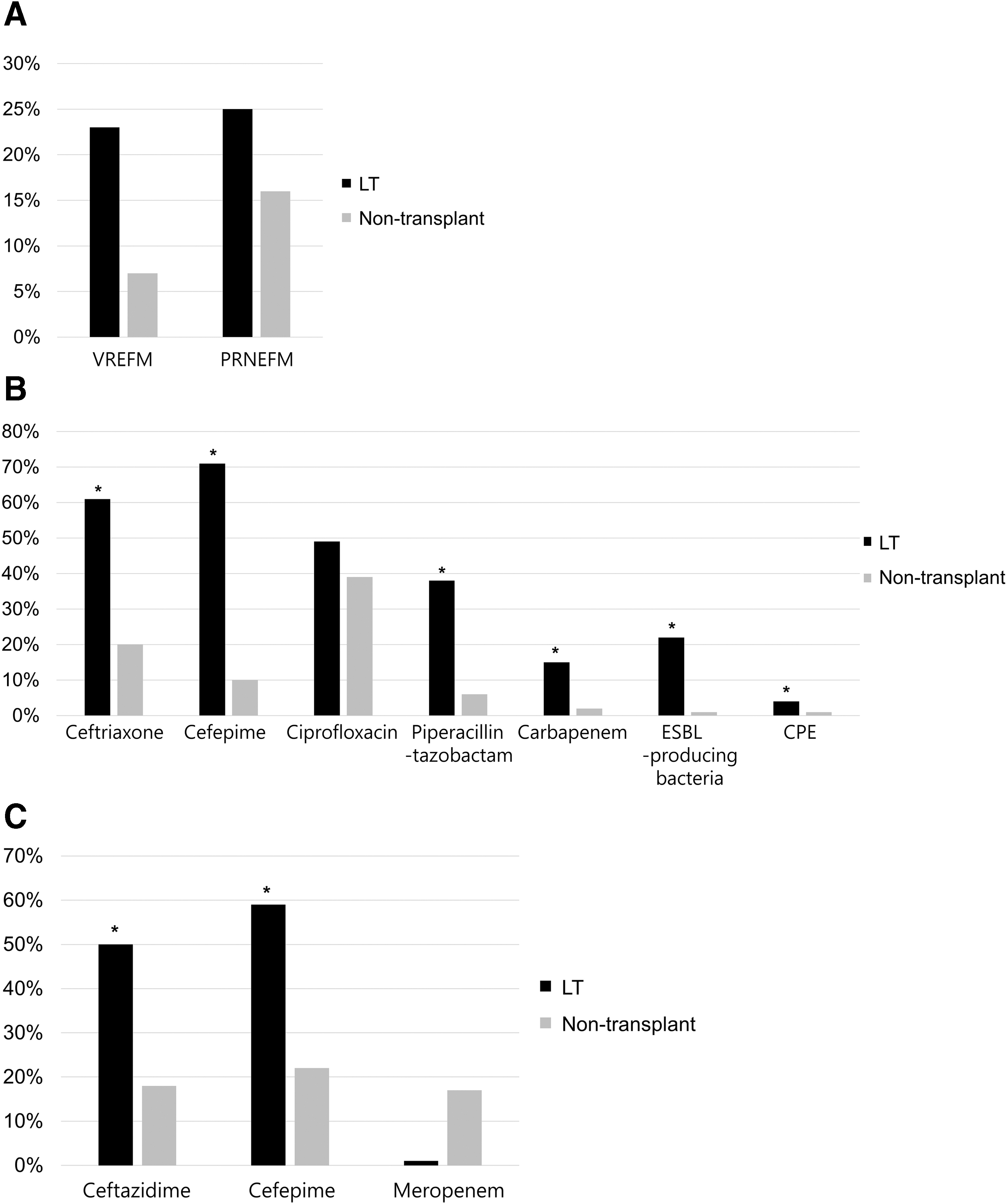
Differences between the antibiotic resistances of bile microorganisms between the liver transplant (LT) group and non-transplant group. (
Influence of several clinical situations in the LT recipients
Peri-operative antibiotic regimen and duration
The most common antibiotic regimen at the transplant centers was ampicillin-sulbactam (81.9%), followed by carbapenem (14.2%) and others (3.9%). There was no difference in biliary flora caused by peri-operative antibiotic regimen and antibiotic resistances between the groups. The mean duration of peri-operative antibiotics was 7.2 ± 4.7 days, mostly administered for fewer than 7 days (71.7%) after LT. There was no difference in biliary flora and antibiotic resistances between peri-operative antibiotic agents administered for more or less than 7 days after LT.
MELD score
The median MELD score of LT recipients was 15 (6–40). The incidences of Enterococcus faecium (14.9% vs. 32.5%; p = 0.029) in the MELD >12 group and non-faecium enterococci (8.5% vs. 1.3%; p = 0.042) in the MELD ≤12 group were higher than in the other group. Vancomycin-resistant Enterococcus faecium (0% vs. 24.0%; p = 0.338) and PRNEFM (25.0% vs. 100%; p = 0.171) were more abundant in the MELD >12 group than in the MELD ≤12 group; however, the increase was not significant. There was no difference in resistances of Enterobacteriales and Pseudomonas to the antibiotic agents commonly used between the groups.
Time interval after LT
Bile microbiology and antibiotic resistances across the patients within three months, three to 12 months, and after 12 months of LT were compared. Gram-positive and gram-negative micro-organisms grew in parallel over 12 months after LT and their growth diverged thereafter; gram-positive micro-organisms showed a significantly decreasing trend in growth (p = 0.047), whereas gram-negative micro-organisms showed a significant increase (p = 0.023; Fig. 3A). Enterococci isolated were most commonly at three months after LT, followed by a decrease in their incidence, although not significant (p = 0.238). The incidence of Enterobacteriales showed a significant increase over time (p = 0.048) and were the most frequently found micro-organisms after 12 months of LT (Fig. 3B). Among the enterococci, Enterococcus faecium showed a decreasing trend over time after LT, although the decrease was not significant (p = 0.078; Fig. 3C). Among the Enterobacteriales, Klebsiella was isolated most commonly, soon after LT, although its incidence showed a significant decrease over time (p = 0.025); Escherichia was isolated most commonly at 12 months after LT (p = 0.098), although it was not significant (Fig. 3D).

Changes of bile micro-organisms over time after liver transplant (LT). (
The abundances of VREFM (40.0% vs. 14.3% vs. 0%; p = 0.261) and PRNEFM (80.0% vs. 71.4% vs. 0%; p = 0.098) decreased over time after LT (Fig. 4A), and resistances of the members of Enterobacteriales to cefepime (100% vs. 66.7% vs. 66.7%; p = 0.436), piperacillin-tazobactam (40.0% vs. 44.4% vs. 33.3%; p = 0.693), and carbapenem (22.2% vs. 15.4% vs. 12.0%; p = 0.472) decreased after 12 months of LT compared with those within three months of LT (Fig. 4B), however, the changes were not significant. The abundances of ceftazidime-resistant Pseudomonas (50.0% vs. 50.0% vs. 50.0%; p = 0.223) and meropenem-resistant Pseudomonas (0% vs. 0% vs. 0%; p = NS) remained unchanged after LT (Fig. 4C).
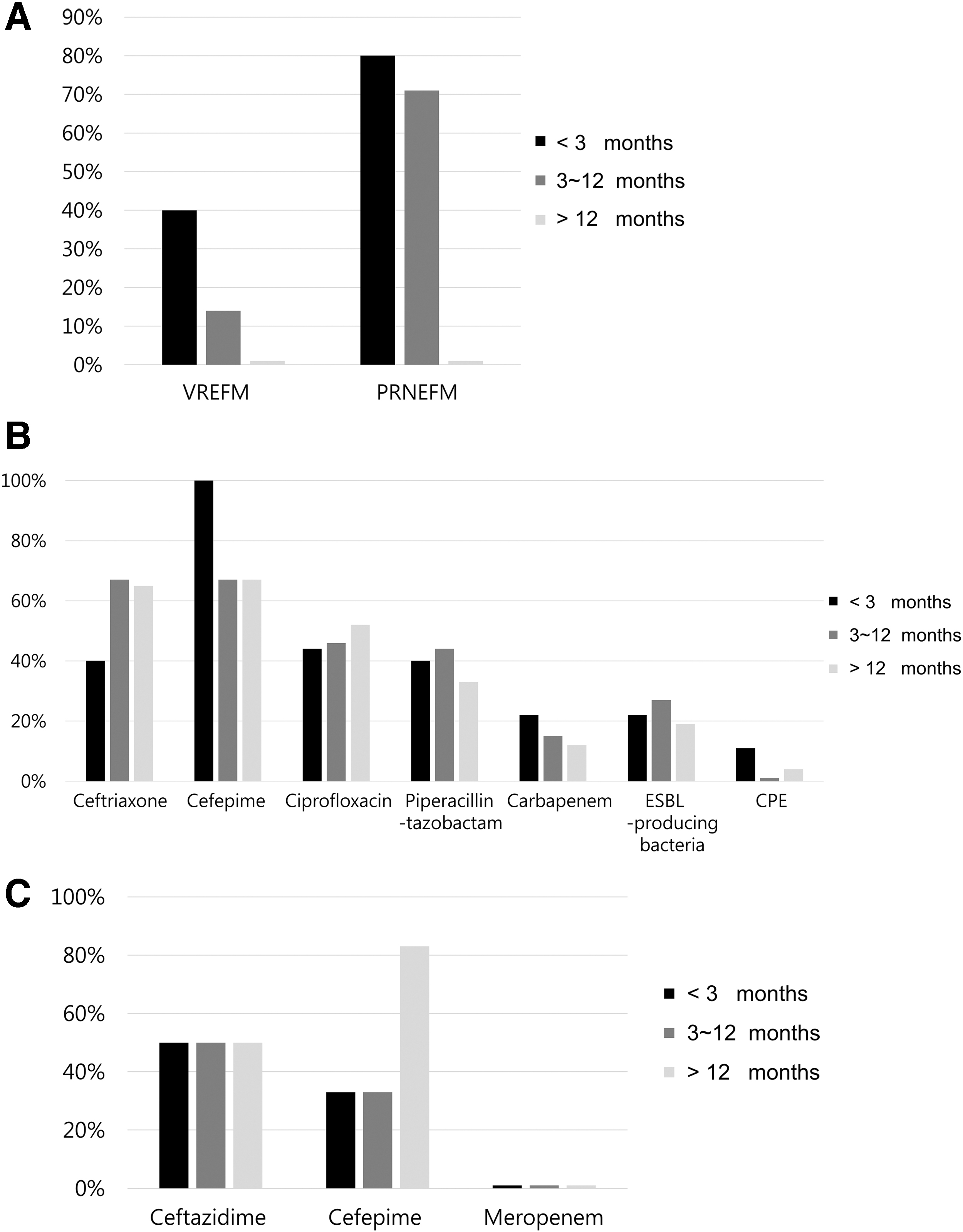
Changes of antibiotic resistances of bile micro-organisms over time after liver transplant (LT). (
Transplant centers
Three centers (36 cultures in A center, 75 cultures in B center, and 16 cultures in C center) were involved in this study. However, there was no difference in the isolated micro-organisms and their antibiotic resistances across the centers.
History of spontaneous bacterial peritonitis
Twenty-nine positive bile cultures (22.8%) were from 25 patients with history of spontaneous bacterial peritonitis (SBP), who mostly received ceftriaxone (72.0%) or meropenem (20.7%) considering the condition of patients. However, there was no difference in the isolated micro-organisms and their antibiotic resistances between patients with and without a history of SBP.
Method of biliary reconstruction
Most bile cultures (91.3%) were obtained from patients who had duct-to-duct biliary anastomosis whereas only 11 positive bile cultures (8.7%) were from patients with hepaticojejunostomy. There was no difference in biliary flora or antibiotic resistance as per the method of biliary reconstruction.
Biliary stricture versus bile leakage
Bile samples were obtained from patients with biliary stricture (82.7%) and bile leakage (17.3%). There was no difference in the isolated micro-organisms and their antibiotic resistances between patients with biliary stricture and bile leakage.
Presence and absence of infectious symptoms
Twenty-five of 127 bile cultures (19.7%) were obtained from patients with infectious symptoms associated with biliary complication. Among the commonly isolated micro-organisms, only Pseudomonas was more common in patients with infectious symptoms than others (28.0% vs. 9.8%; p = 0.017). However, there was no difference in antibiotic resistance between the groups.
Discussion
The current study suggested that poly-microbial infection is more common in LT recipients than in non-transplant population with acute cholecystitis, hence implying that to be effective for patients with severe biliary infection after LT, the initial antibiotic therapy should comprise two or more agents. There are many potential reasons for this result. First, LT recipients receive immunosuppressive agents to prevent graft rejection after transplantation, which may provide a favorable environment for bacterial growth. Second, relatively long-term use of antibiotic agents, because of repeated hospitalizations before transplant, in conjunction with invasive devices during the peri-operative period of LT, might change the bile bacterial flora and increase their antibiotic resistance. Third, LT recipients with biliary complications require biliary intervention, such as PTBD or ERCP, which increases the possibility of combined infection from micro-organisms of the skin, gastrointestinal tract, or the catheter itself.
Previous studies had demonstrated increased biliary enterococcal isolations from patients with PTBD [12], however, there was no difference between the groups in this study. We found a higher proportion of Enterococcus faecium in the LT recipients and non-faecium enterococci in the non-transplant group. In a previous study describing bile colonization and intestinal flora of LT recipients, similar results were obtained, implying enterococci, predominantly Enterococcus faecium, as the most common gram-positive microorganisms [13]. The reason for this difference between LT recipients and the non-transplant population could be the recurrent usage of antibiotics in LT recipients. Non-faecium enterococci, including Enterococcus faecalis, Enterococcus gallinarum, Enterococcus casseliflavus, and Enterococcus avium showed high susceptibility to commonly used antibiotics; however, Enterococcus faecium showed more antibiotic resistance than non-faecium enterococci [14].
Enterococci in bile do not usually cause bacteremia, because most are colonizers; routine use of antibiotic agents against enterococci can lead to their resistance to antibiotic agents, and hence, is not recommended [15]. However, because LT recipients receive immunosuppressive drugs, which make them vulnerable to infection, they require treatment with antibiotic agents. To highlight this issue, a previous report had shown that enterococci account for 24.4% of bacteremia cases and are the most common cause of sepsis among LT recipients [16]. Broad-spectrum β-lactam/β-lactamase inhibitors, such as ampicillin-sulbactam, had been recommended as the first-line treatment against enterococci in previous guidelines for non-transplant populations [5]. In fact, penicillin and ampicillin provided good protection against non-faecium enterococci, which are found to be predominant in the non-transplant population. However, Enterococcus faecium, mostly isolated from LT recipients, has been reported to show increased antibiotic resistance to commonly recommended drugs, specifically, ampicillin-sulbactam; hence, vancomycin had been used for an initial antibiotic therapy instead [14]. The abundance of VREFM was also found to be increased in LT recipients in this study; thus, other antibiotic agents, including daptomycin, linezolid, and tigecycline, which offer good protection against VREFM, should be considered in patients with severe biliary infection. Tigecycline has shown limited efficacy in patients with septic shock [17]. However, it is still recommended for other cases, because it has the added advantage of being a wide-spectrum drug that is effective for various gram-negative micro-organisms, including ESBL-producers.
Previous studies had shown bile acids to have antimicrobial properties, which keep the biliary tract sterile under non-pathogenic conditions [18]. However, gram-negative micro-organisms commonly found in the intestinal tract, namely Enterobacteriales, were frequently isolated from patients with biliary infection [19]. Enterobacteriales, especially Escherichia, became more resistant to bile by developing defense mechanisms, than gram-positive micro-organisms and were sensitive to the deleterious effects of bile that they frequently colonized in the gallbladder, which in turn is an important reservoir for biliary infections [20,21]. Recurrent usage of antibiotic agents mainly targeting Enterobacteriales in LT recipients caused substantial difference in their incidence between the groups in this study. The influence of different immune responses related to immunosuppression on chronic bacterial colonization and their antibiotic resistances in this study was unclear that further experimental study would be required. Members of Pseudomonas, which are non-fermentative gram-negative bacilli, are majorly responsible for bacteremia in hospitalized and immunocompromised patients [22]. Most infections caused by Pseudomonas develop within a few months after LT, possibly because of high immunosuppression during this period [23]. Compared withto that in non-transplant population, Pseudomonas in LT recipients with recurrent hospitalization and immunocompromised status was shown to be substantially more frequent in this study.
For gram-negative infections, third- or fourth-generation cephalosporins, or piperacillin-tazobactam are recommended as the first-choice drugs, whereas fluoroquinolones and carbapenems are second choice, depending on the condition of patients and their individual susceptibility patterns [5]. In this study, the antibiotic resistance of Enterobacteriales members to ceftriaxone and ciprofloxacin and that of Pseudomonas to cefepime increased by more than 20% in both groups, reflecting the extensive use of these antibiotic agents. Cefepime, piperacillin-tazobactam, and ceftazidime showed good activity against Enterobacteriales in the non-transplant population (as did ceftazidime against Pseudomonas), although resistance to all these substances was increased in LT recipients. These antibiotic agents, therefore, may not be recommended for empirical antimicrobial therapy in LT recipients; carbapenems, specifically meropenem against Pseudomonas, or tigecycline, could be recommended as an alternative, especially considering the threat of ESBL-producing gram-negative microorganisms. In particular, CRE have emerged as important health-care–associated pathogens because of instances of extensive drug resistance and high morbidity and mortality [24]. In this study, ESBL-producing gram-negative micro-organisms and CRE were more frequent in the LT group than in the non-transplant population, although their incidences decreased later on, compared to that in the early period after LT, thus recommending continuous monitoring of these micro-organisms.
Influence of several clinical variables on biliary flora and their antibiotic resistances was analyzed in the LT group. Patients with MELD >12 had more complications of portal hypertension, such as ascites, varix bleeding, and hepatic encephalopathy, which require recurrent hospitalization and antibiotics usage, compared with those with MELD ≤12. It might be the cause of difference in prevalent enterococcal species across patients with MELD >12, Enterococcus faecium and MELD ≤12, and non-faecium enterococci similar to LT recipients and non-transplant population. Different time intervals after LT showed differences in isolated micro-organisms and antibiotic resistances. Because of the usage of peri-operative antibiotic agents in LT recipients, Enterococcus faecium was only isolated within three months of LT, whereas non-faecium enterococci, significantly more common in the non-transplant population, were increasingly isolated beyond three months of LT in this study. The abundance of VREFM was also found to be increased in LT recipients, especially within three months of LT, although VREFM and PRNEFM were remarkably reduced after 12 months of LT, thereby suggesting the transition from hospital- to community-acquired infection. Among Enterobacteriales, Klebsiella is a major concern in patients hospitalized with chronic liver diseases, for dialysis, cancers, and solid organ transplantation [25]. In this study, Klebsiella was mostly isolated early after LT, although its incidence decreased over time, and Escherichia, prevalent in the non-transplant population, was most commonly isolated at 12 months after LT. These changes might have been caused by the transition from hospital- to community-acquired infection over time after LT, indicating the time interval after LT to be a useful measure for the selection of effective antibiotic agents for LT recipients with biliary infection. Liver transplant recipients who had infectious symptoms because of biliary complications had increased incidence of Pseudomonas, one of the main micro-organisms responsible for bacteremia in hospitalized and immunocompromised patients, therefore, it should also be considered before selecting antibiotic agents.
This study had several limitations, including its retrospective design. The assumed accuracy of the data relies on the completeness of medical records. Moreover, there were some differences between the antibiotic susceptibility tests performed at each hospital. Furthermore, the results presented here are limited to a specific area and should be extended in future to take geographical variation into account. Finally, the study population was relatively small; future studies should involve a larger number of patients to confirm the results.
Conclusions
There were differences in the compositions of bile micro-organisms and their antibiotic resistance profiles between LT recipients and the non-transplant population. Isolation of poly-microbial cultures was higher in the LT group than in the non-transplant group. Enterococcus faecium and Pseudomonas were more frequent in the LT group, whereas non-faecium enterococci and members from Enterobacteriales, especially, Escherichia, were predominant in the non-transplant group. Most of the antibiotic agents recommended as initial antibiotic therapy for the non-transplant population as per previous guidelines were not effective in LT recipients. The incidences of Enterococcus faecium in the LT recipients with MELD score >12 and non-faecium enterococci in those with MELD score ≤12 were significantly higher than those in the other group. The incidence of members from Enterobacteriales, commonly isolated in the non-transplant group, showed an increase over time after LT; they were mostly isolated after 12 months of LT. Differences in micro-organisms and their antibiotic resistances between the LT group and non-transplant group decreased over time after LT, probably suggesting that a community-acquired infection occurred during the transition from hospital to home. The incidence of Pseudomonas was more common in the LT recipients with infectious symptom than others. Antibiotic therapy for biliary infection in LT recipients should be different from that in the non-transplant population, considering clinical factors such as the time interval after LT, MELD score, and presence of infectious symptoms.
Footnotes
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.