
Abstract
Background:
Mycotic aneurysms (MAs) are relatively rare but life-threatening. Some recent reports have described the use of endovascular therapy for their treatment; however, this still is a controversial treatment, and a definite target population has not been determined.
Methods:
We performed surgery on 34 patients with MAs from March 2005 to March 2019. Twenty patients who underwent open surgery (OS) first comprised the OS group, and 14 patients who underwent endovascular therapy first comprised the stent-graft (SG) group. We analyzed between-group differences, long-term outcomes, and risk factors for death retrospectively. Patients in the OS group had a higher initial white blood cell count than those in the SG group (p = 0.047). The SG group had more patients with a low albumin concentration (≤2.0 mg/dL) than did the OS group (p = 0.026).
Results:
There were no significant differences in the operative mortality rates between the groups (p = 0.773). Additional procedures were required more often in the SG than the OS group (p = 0.0013). The overall survival rate as estimated by the Kaplan–Meier method was 88% at 1 month, 67% at 1 year, 57% at 3 years, and 45% at 10 years. In the univariable analysis, chronic obstructive pulmonary disease (COPD) was a risk factor for death (p = 0.003).
Conclusions:
Endovascular therapy for MAs produced reasonable outcomes when patient selection was based on the activity level, nutritional condition, and degree of inflammation. Endovascular therapy may become an option for patients with a low albumin concentration or COPD despite the fact that additional procedures may be needed.
Mycotic aneurysms (MAs) are relatively rare but have an associated hospital mortality rate ranging from 11% to 36% [1–9]. Various methods to improve outcomes have been described, including debridement of the infection focus; omentum wrapping; use of stent-grafts (SGs), rifampicin-soaked grafts, and homografts; and extra-anatomic bypass. Nevertheless, the optimum strategy remains a matter of debate [1,6,10–12]. Even when open surgery (OS) for MA is successful, some patients die of post-operative complications or experience long-term debilitation. Our mission as cardiovascular surgeons is to save more patients with this challenging disease. If patients who are potentially suitable for endovascular therapy can be identified, the total number of survivors can be expected to increase even if the number of survivors of OS decreases (Fig. 1).

Concept of improved outcome by surgical treatment for mycotic aneurysms. Outer squares show all patients with mycotic aneurysms. Solid-line circles show survivors of open surgery. Dotted-line circles show survivors of endovascular treatment. The area outside the circles within squares shows nonsurvivors. A larger total area of the circles indicates a higher number of survivors.
We utilize SGs in our hospital, especially for patients of advanced age and patients with low activities of daily living. Moreover, our surgical approaches even for MA involve a combination of OS and endovascular therapy, including thoracic endovascular aortic repair (TEVAR) and endovascular aortic repair (EVAR), and we have obtained good results using these approaches.
Previous studies of similar endovascular therapies have not reported suitable target patients for surgical intervention. Therefore, this retrospective study was performed not only to assess the outcomes of surgical treatment (including endovascular therapy) for MA but also to examine the features of selected patients and the validity of choosing endovascular therapy.
Patients and Methods
Patients
We identified 34 patients with MAs who underwent surgery in our hospital from March 2005 to March 2019. An MA was defined according to the following criteria: Clinical presentation (pain, fever, or concomitant infection), laboratory test results (elevation of inflammatory markers such as the white blood cell count and C-reactive protein concentration or positive blood culture), and computed tomography (CT) findings (rapid expansion of aneurysm, saccular aneurysm, eccentric aneurysm, peri-aortic gas, or peri-aortic soft tissue mass) (Fig. 2) [13]. We included patients with aneurysms accompanied by aorto-tracheal, aorto-esophageal, and aorto-enteric fistulas.
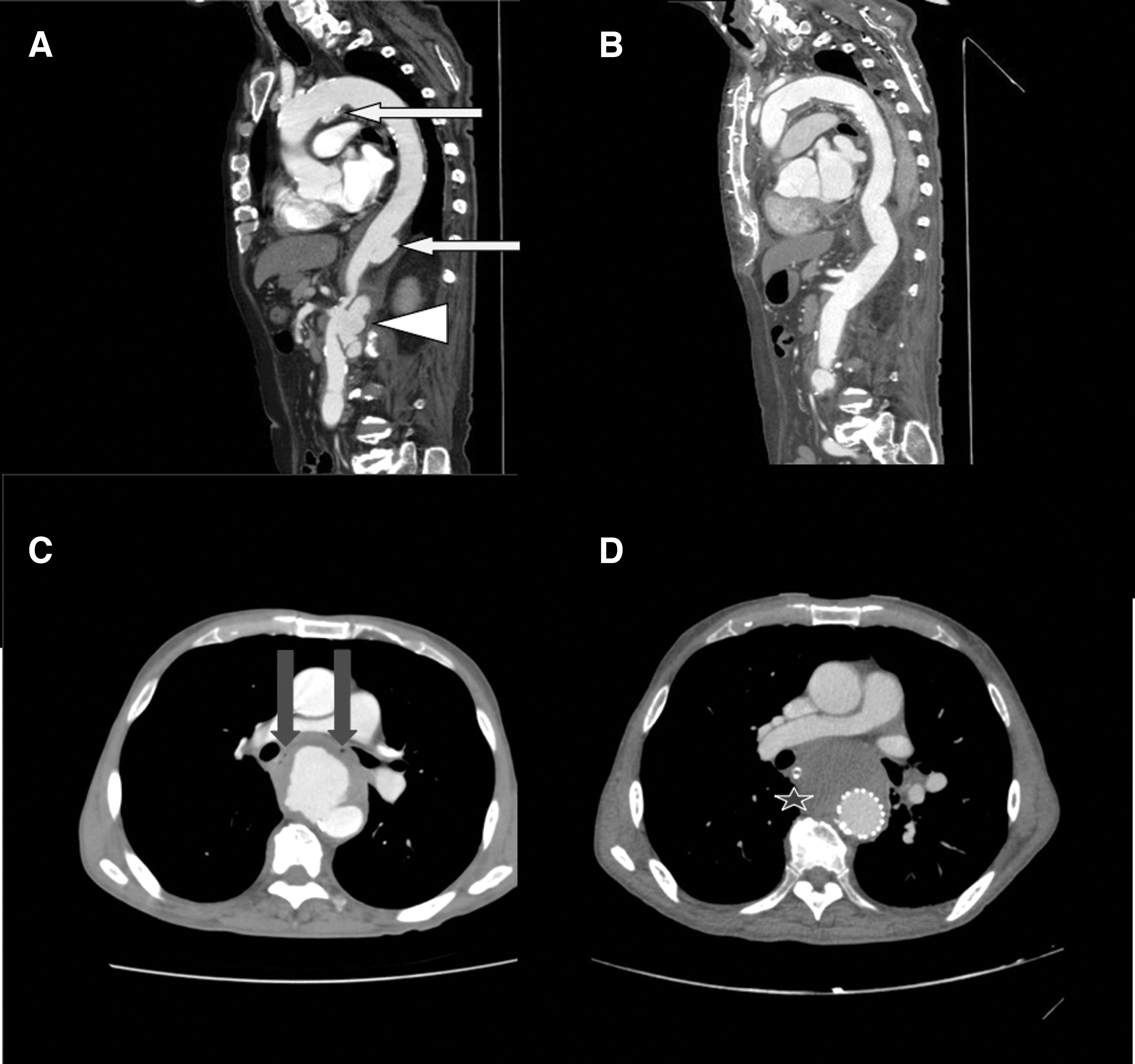
Computed tomography (CT) images showing examples of mycotic aneurysms. (
Strategy
The surgical indications were rupture, including penetration of the digestive tract or trachea; fistula formation; rapid enlargement; deformity of the aneurysm; and uncontrollable infection.
Surgery was performed on an emergency basis. However, it was considered elective if the inflammatory marker concentrations had improved and the patients were stable and pain free.
Our treatment strategy was either: (1) OS by graft replacement plus omental filling or (2) SG placement. We chose OS first when CT showed peri-aortic gas or an abscess. In other cases, we chose SG placement first, especially in patients with a poor general condition without elevated inflammatory markers such as the white blood cell count and C-reactive protein concentration; we subsequently added debridement, abscess drainage, or omental filling if needed [14]. We decided whether to perform OS or SG during a cardiovascular surgery conference in our hospital.
We compared the pre-operative status and surgical outcomes of the OS and SG groups retrospectively. The patients in the SG group underwent endovascular therapy such as TEVAR or EVAR first. All patients were followed up for 2 weeks to 14 years (from April 2005 to March 2019; mean 45 ± 42 months), and CT examinations were performed four times in the first year and twice yearly thereafter. Oral antibiotics were administered for 3 months after confirmation of a negative inflammatory marker status.
This study was approved by the ethics committee of our hospital (Approval No. 1905-01). The requirement for individual informed consent was waived because of the retrospective nature of this study.
Surgical procedures
Open Surgery
Basically, OS was performed by debridement of the infected area, including the aneurysm, and in situ revascularization with a woven Dacron graft under general anesthesia. Especially for thoracic or thoraco-abdominal aneurysms, grafting was performed using cardio-pulmonary bypass with or without deep hypothermic circulatory arrest. Autogenous grafts are difficult to obtain in Japan, and we could not prepare rifampicin-soaked Dacron grafts in advance. Therefore, when possible, the graft was wrapped by omentum or latissimus dorsi muscle [15]. For safety, we selected extra-anatomic bypass for MAs in the iliac area because of doubts regarding the ability to achieve complete debridement and in consideration of the patients' poor condition [16,17]. If the patient had an apparent fistula to the digestive tract, the fistula was resected; and the digestive tract was reconstructed by digestive surgeons [12,18].
Endovascular therapy
First, SGs usually were placed to protect any sites of potential rupture, such as a fistula or worsening aneurysm, under local and intravenous anesthesia [19]. If the patient had an apparent fistula to the digestive tract, the fistula was resected; and the digestive tract was reconstructed.
If the patients did not recover, we considered additional debridement and drainage or graft replacement and omental wrapping (Fig. 3).

Computed tomography (CT) images showing successful outcome by additional drainage in patient in stent-graft group. (
Statistical analysis
Categorical variables are expressed as a proportion and continuous variables as mean ± standard deviation. Univariable logistical regression analysis of risk factors for 30-day and long-term hospital death was performed. The long-term survival rate was calculated using the Kaplan–Meier method. The survival rates in the OS and SG groups were compared using the log-rank method. The χ2 test and the Mann–Whitney U test were used for other statistical analyses. All analyses were performed using JMP 9.0 software (SAS Institute, Cary, NC, USA). Differences were considered significant at p < 0.05.
Results
Table 1 shows the patients' clinical characteristics. The patients in the OS group had a higher white blood cell count (p = 0.047), and the SG group had more patients with a low albumin concentration (≤ 2.0 mg/dL) (p = 0.026).
Pre-Operative Clinical Features
p < 0.05.
COPD = chronic obstructive pulmonary disease, Cr = creatinine, OS = open surgery, SD = standard deviation, SG = stent-graft.
Table 2 summarizes the culture results of the pathologic lesions. The positive rate of blood or infectious organism culture was 94%. In two patients, the pathogen was not identified because antibiotic treatment had already been introduced at the hospital of origin. These two patients showed eccentric and multi-lobular aneurysms with rapid expansion; therefore, we were able to diagnose all cases as MAs because we had already excluded other infections such as urinary tract infection, cholecystitis, and pneumonia.
Bacterial Species in Each Aneurysm Location
Others were anaerobic gram-positive bacilli in the thoracic region, Peptostreptococcus asaccharolyticus in the thoraco-abdominal region, anaerobic gram-negative bacilli and Aeromonas hydrophila in the abdominal region, and Edwardsiella tarda in the iliac region.
MRSA = methicillin-resistant Staphylococcus aureus; MSSA = methicillin-sensitive S. aureus.
The details of the surgical treatment and comparison of post-operative complications and deaths are presented in Tables 3 and 4, respectively. Although there was no significant difference in the operative mortality rate (p = 0.773) or hospital mortality rate (p = 0.447) between the two groups, more additional procedures were needed in the SG than the OS group (p = 0.0013). The causes of long-term in-hospital death were re-rupture (n = 3), sepsis (n = 1), and pneumonia (n = 1) in the OS group and re-rupture (n = 1) and pneumonia (n = 1) in the SG group. Additional procedures needed were graft replacement or bypass with debridement and drainage (n = 3) and debridement and drainage with or without an omental flap (n = 3).
Surgical Treatments and Outcomes of Mycotic Aneurysms Treated by Open Surgery (n = 20)
Digestive tracts with fistulas were resected simultaneously by general surgeons for patients with aorto-esophageal or aorto-duodenal fistulas.
Latissimus dorsi muscle wrapping.
CPB = cardiopulmonary bypass, DD = debridement and drainage, DHCA = deep hypothermic circulatory arrest, OS = open surgery, SG = stent-graft;
Post-Operative Major Aorta-Related Complications and Deaths
One graft replacement with omental flap, one axillo-femoral bypass, and one femoro-femoral bypass.
Two omental flaps with debridement and one ligation of tracheal artery for type II endoleak with drainage.
All causes were re-rupture.
DD = debridement and drainage, OS = open surgery, SG = stent graft.
All patients were followed up for 2 weeks to 14 years (mean 45 ± 42 months). The OS group tended to have a longer follow-up period than the SG group; however, there was no significant difference between the groups (OS 55.7 ± 48.1 months; SG 25.6 ± 22.4 months; p = 0.113). One patient in the SG group (7%) required an additional procedure on re-admission after discharge. Figure 4A shows the overall survival curves as estimated by the Kaplan–Meier method; the survival rate was 88% at 1 month, 76% at 5 months, 67% at 1 year, 57% at 3 years, and 45% at 10 years. Figure 4B compares the survival rates in the OS and SG groups. Although there were no significant differences between the groups, the SG group showed a tendency toward better survival.
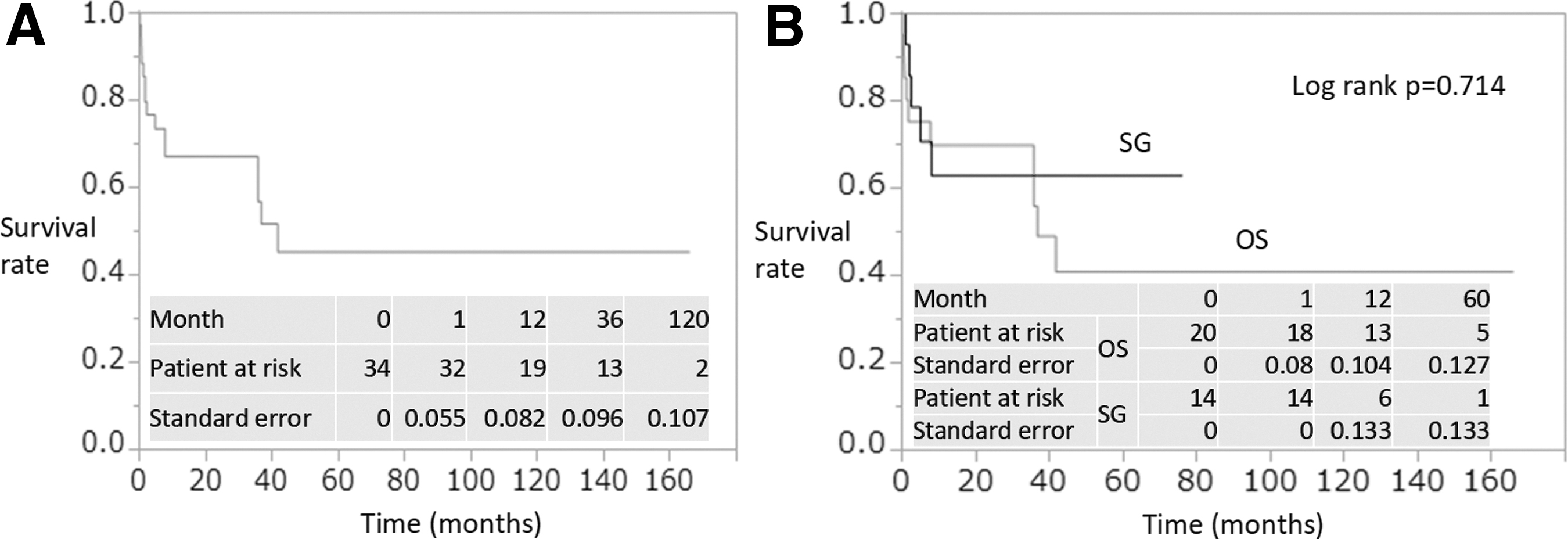
Kaplan–Meier long-term survival curves. (
Risk factors for death were compared between the groups (Table 5). The univariable analysis showed that fever and chronic obstructive pulmonary disease (COPD) were risk factors for death within 30 days (p = 0.030 and p = 0.003, respectively) and that age, diabetes mellitus, COPD, and tracheotomy were risk factors for long-term in-hospital death (p = 0.024, p = 0.028, p = 0.003, and p = 0.040, respectively).
Risk Factors for In-Hospital Death
CI = confidential interval, Cr = creatinine, COPD = chronic obstructive pulmonary disease; OR = odds ratio.
Discussion
There are many factors to consider when treating patients with MAs, some of which depend on the location, presentation (rupture, fistula, expanding aneurysm), potential organism, and cause of infection [1–6,10–12]. If the vessel is to be replaced, there are options including extra-anatomic bypass, rifampin-soaked grafts, or homografts. On the other hand, because endovascular therapy has become more widely used, the employment of SGs for treatment of MAs has been described in many reports (1–7,9,13). The Japanese guidelines for diagnosis and treatment of aortic MAs classify SG therapy as class III, and some authors have stated that EVAR should be a “bridge” treatment to delay open repair (9,20–22). In other studies, EVAR was combined with abscess drainage (1,23). However, these studies excluded patients with aorto-enteric fistulas, and most MAs with fistulas were severe, making the treatment more challenging (3,6,18). We used SGs for treatment of MAs, including fistulas, on a case-by-case basis and obtained good results. Thus, it is clinically meaningful to examine how patients are treated successfully by endovascular therapy because these patients have various factors that must be considered, including co-morbidities, their inflammatory level, and their nutritional condition.
In this study, the emergency surgery rate was high at 79% (27 patients) (see Table 1). However, the ideal treatment strategy often is suggested to be elective after improvement of inflammatory markers using antibiotic therapy, and some studies have indicated that pre-operative antibiotic administration must range from several days to a few months to be effective (1,3,5–9,14,23,24). Nevertheless, delaying surgical intervention sometimes can worsen the condition as long as the infectious focus remains. Therefore, we believe that early surgery is better if the inflammatory values do not improve or signs of peri-aortic gas remain on CT after antibiotic administration. Moreover, we believe that this policy is one of the reasons for our favorable results. The inflammatory marker values improved in only seven patients (four in the OS group and three in the SG group), and these patients were subsequently treated electively. Conversely, we decided to perform emergency surgical intervention in the remaining patients because antibiotic therapy alone was not effective, and 26 patients had ruptured aneurysms.
Regarding our treatment policy, we chose endovascular therapy for patients with low activity or poor nutrition who would not have been able to endure invasive OS. Compared with those in the SG group, the patients in the OS group had higher white blood cell counts, which might have represented severe disease. However, the SG group had only a few patients with high white blood cell counts and had more malnourished patients as judged by the prevalence of low albumin concentrations (see Table 1). Thus, we suggest that overtly moribund patients can escape death by undergoing SG placement to protect the aneurysm, even if temporarily. If necessary, they subsequently can undergo additional operations such as graft replacement or debridement and drainage to accelerate healing by removing the infected fluid.
Endovascular therapy stabilizes patients with aneurysms hemodynamically. However, artificial devices, namely the SGs, are left in situ. We assume that patients who respond well to endovascular therapy have lower degrees of inflammation. However, SGs were able to be used first as protection against rupture or high degrees of inflammation, allowing a combination of drainage, debridement, or omental filling or conversion to OS to be considered after improvement of their nutritional and general condition. Additionally, the outcome in the SG group was good among the selected patients. Therefore, improving the outcomes of patients undergoing OS and taking measures to manage risk factors will lead to better results.
In this study, the univariable risk factor analysis of 30-day and long-term in-hospital death identified COPD as a risk factor. Of all causes of in-hospital death, pneumonia occurred in two patients (28.6%); once patients with COPD develop pneumonia, their condition tends to become critical. With respect to other risk factors, we cannot change pre-operative factors such as age, fever, or co-morbidities; but we can adjust the timing or choice of invasive surgery for patients in poor condition. The present study showed that tracheotomy is a risk factor for long-term in-hospital survival. Therefore, it is important for us to select the optimal treatment policy that will help to prevent post-operative tracheotomy or pneumonia. Endovascular therapy may be more desirable for patients with poor respiratory function, including patients with COPD, if allowed by the laboratory data and aneurysm findings.
We evaluated each treatment option in the present study comprehensively, placing importance on the patient's activity ability, nutritional condition, degree of inflammation, and co-morbidities such as COPD as discussed at our cardiovascular surgery conferences. Focusing on these criteria during patient selection will be required to ensure better outcomes. Overall, our study has shown that the appropriate use of endovascular therapy based on proper patient selection may lead to good early results with an acceptable operative mortality rate.
This study has some limitations that must be acknowledged. It was performed at a single center and had a retrospective design and limited sample size. Moreover, we did not examine the outcomes according to the aneurysm location or timing of surgical treatment; this should be performed after sampling more patients. We do not believe that endovascular therapy will replace OS completely for treatment of MAs. However, a larger sample and longer follow-up data regarding endovascular therapy are required to increase the possibility of good treatment selection and make further improvements.
In conclusion, the SG group had more patients with an albumin concentration of ≤2.0 g/dL than did the OS group. Our aggressive approach in which we performed prudent patient selection and did not hesitate to perform an emergency operation may have led to our reasonable outcomes, although the patients in the SG group needed more additional procedures than those in the OS group. We thus believe that endovascular therapy may be an effective treatment option that can be combined with debridement and drainage or additional graft replacement with an omental flap in carefully selected patients with MAs.
Footnotes
Acknowledgment
Funding Information
The authors received no funding for the preparation of this manuscript.
Author Disclosure Statement
The authors have no conflicts of interest or financial relations to declare.