
Abstract
Background:
The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) has been proposed as a diagnostic tool for necrotizing soft tissue infection (NSTI). However, its utility remains underreported, particularly in patients with comorbid conditions. The purpose of this study was to identify the test characteristics of LRINEC for patients with various comorbid conditions.
Patients and Methods:
We conducted a retrospective study including patients with suspected NSTI. Our study patients were then relegated into the subgroups; intravenous drug use (IVDU), end-stage liver disease (ESLD), and diabetes mellitus (DM). Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of a positive LRINEC score (≥ 6 or 8) were calculated in reference to intra-operative findings or results of the pathologic examination. Area under the curve (AUC) using receiver operating characteristic (ROC) plots were compared between each subgroup and the overall study population using DeLong test.
Results:
A total of 220 patients were included for the analysis. Overall, the sensitivity was 76%, specificity of 52%, PPV of 32%, and NPV of 88%. The subgroup analysis showed low PPVs in all subgroups. The DM and ESLD groups had a high NPV (90.5% and 88.0%, respectively), whereas NPV in the IVDU group was 70.6%. The AUC and DeLong test for the subgroups were 0.649 (p = 0.902) for ESLD, 0.699 (p = 0.683) for DM, and 0.565 (p = 0.034) for IVDU.
Conclusions:
The LRINEC can be a useful adjunct to rule out the diagnosis of NSTI with exception of IVDU. In contrast, further diagnostic workup might be still required in those patients with positive LRINEC.
Soft tissue infections are one of the most common complaints in the emergency department and have a wide degree of severity. These can range from more common infections such as impetigo, cellulitis, and abscesses to necrotizing soft tissue infection (NSTI), a rare but life-threatening condition. According to the U.S. Centers for Disease Control and Prevention, there are an estimated 9,000–11,500 cases of NSTI each year in the United States, with approximately 1,000–1,800 of these resulting in death [1].
Because of the relatively low incidence and vague early symptoms related to NSTI, a simple and effective way to differentiate from non-NSTIs is of utmost importance to initiate early therapeutic interventions, including surgical debridement. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) is a clinical tool that was developed to help differentiate those patients with NSTI from those with non-NSTI, primarily using common laboratory values on presentation [2]. Despite the recent development of the LRINEC to aid in achieving diagnostic accuracy, the current literature has not reached a clear consensus regarding its utility in cases with suspected NSTI [3–10]. Reasons for the discrepancies in the result of previous studies that examined the diagnostic utility of the LRINEC can be attributed to population differences in comorbid medical conditions and modifiable risk factors, such as intravenous drug use (IVDU) [11–15]. Furthermore, abnormal laboratory results (e.g., glucose, sodium level) in these patients are often resulted from their comorbid conditions.
Therefore, we believe that the use of the LRINEC should be tailored in each subgroup of patients with different comorbid conditions to be utilized efficiently in the clinical setting. The purpose of this study was to analyze the utility of the LRINEC as an instrument for identifying patients with NSTI in patients with different comorbid conditions. We stratified our study patients by known risk factors associated with NSTI, including end-stage liver disease (ESLD), diabetes mellitus (DM), and IVDU to determine whether there is a greater or lesser value within these subgroups. We hypothesized that patient's associated comorbid conditions would influence the utility of LRINEC as a diagnostic tool for NSTI.
Patients and Methods
We conducted a retrospective cohort study at the Los Angeles County + University of Southern California (LAC+USC) Medical Center from January 1, 2015 to July 30, 2018. The LAC+USC Medical Center is an acute care teaching facility and one of the largest county hospitals in the Unites States with more than 150,000 annual visits to the emergency department. This study was approved by the Institutional Review Board for the University of Southern California.
All patients aged 18 years or older who required a consultation to the acute care surgery service with primary concern for NSTI were included in the study. Preliminary diagnosis or concern for NSTI was made by emergency medicine physicians or internists based on the patient's symptoms and physical findings. We excluded patients who were ultimately diagnosed with diabetic ulcers or gangrene, patients whose tissue debridement was performed at an outside hospital, or those missing any of the six laboratory values required to calculate the LRINEC score at the time of consultation (C-reactive protein [CRP], hemoglobin, white blood cell count [WBC], sodium, creatinine, and glucose) [16,17]. Diagnosis of NSTI was confirmed with either intra-operative findings of soft tissue necrosis or pathology report indicating the presence of tissue necrosis in the surgical specimen. All operative and pathology reports were reviewed independently by two investigators (R.H. and K.M.) to verify the diagnosis of NSTI.
Subsequently, our study patients were divided into two groups: NSTI group and non-NSTI group. We calculated a LRINEC score ranging from 0–13 for each patient in both groups. Two common cutoff values were evaluated for the diagnostic accuracy: LRINEC scores ≥6 or 8 fell into the test positive group, and those <6 or 8 were considered test negative [6]. Patients' demographic data, vital signs on surgical consultation, LRINEC laboratory values, and patient outcomes including in-hospital mortality and hospital length of stay (LOS) were collected for the analysis. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of a positive LRINEC score (≥ 6 or 8) were calculated in reference to intra-operative findings or results of the pathological examination in the total study population, as well as each subgroup of patients with ESLD, DM, IVDU, and no comorbidities.
Statistical analysis
Descriptive statistics were reported as medians and interquartile ranges for continuous variables and as frequencies and proportions for categorical variables. Between comorbid subgroups, variables were compared using univariable analysis. Either χ2 or Fisher exact test was used for categorical variables and analysis of variance (ANOVA) was used for continuous variables as appropriate. For each subgroup, sensitivity and specificity estimates were plotted on a receiver operating characteristic (ROC) space for all cutoff values (0–13 points), and calculation of the area under the curve (AUC) were performed. The AUC values were compared between each subgroup and the total sample using DeLong test for two ROC curves [16]. We considered p values <0.05 to be significant. Analysis was performed using SAS Studio Software for Windows version 3.6 (Cary, NC) and R version 4.0.0 (R Foundation).
Results
After 113 patients were excluded because of missing components of the LRINEC score, a total of 220 patients were included for the analysis. The diagnosis of NSTI was confirmed in 50 patients (22.7%), whereas the other 170 patients did not meet the diagnostic criteria. Of the 113 patients who were excluded from the analysis, 21 (18.6%) were found to have NSTI. Most consultations were received from the emergency department (84.1%), followed by the internal medicine services (12.2%), and the remainder from a variety of other services (orthopedics, urology, gynecology, and otolaryngology). The majority were male (72.7%), and the median age was 51 years (interquartile range, 38–57). Further stratification noted 43 patients with ESLD (19.5%), 72 patients with DM (32.7%), 43 patients with IVDU (19.5%), and 72 patients with no comorbidities (32.7%). Of the 50 patients with NSTI, 35 (70.0%) had admission or emergency physician notes that denoted a strong concern for NSTI based on physical findings, such as crepitus, rapid progression of erythema, pain out of proportion to examination, or hemorrhagic bullae. For the patients with confirmed NSTI, the median LOS was seven days, and the overall in-hospital mortality rate was 26.0%. Of the 170 patients who were found not to have NSTI, the vast majority were noted to have cellulitis (82.9%). Associated abscesses were identified in 58 patients (34.1%) and 37 patients (21.8%) required operative or bedside drainage of these abscesses. In addition, 15 (8.8%) patients required operative exploration to rule out NSTI. Of these 15 patients, four had LRINEC scores suggestive of NSTI (≥6 points) but were ultimately ruled out in the operating room. None of these patients were noted to have radiographic findings pathognomonic for NSTI, but were noted to have physical findings, such as bulla formation.
Table 1 compares the results of LRINEC score between each study group. Overall, of the values used in the LRINEC score, white blood cell count (WBC), and hemoglobin were the most likely to be positive (54.6% and 76.8%, respectively). Of note, the sodium level was more likely to meet the positive criteria in patients with ESLD and DM (67.4% and 50.0%, respectively). Similarly, 44% of patients with DM were positive for the glucose criteria. Overall, when using a cutoff of LRINEC score ≥6, the LRINEC was considered positive in 119 patients (54.1%), whereas 50.5% were positive with a cutoff of LRINEC score ≥8 (Fig. 1A and 1B). The sensitivity and specificity for LRINEC score ≥6 in our total study population was 76.0% and 52.4%, respectively, and the PPV was 31.9% and the NPV was 88.1% (Table 2). For LRINEC score ≥8, the sensitivity was 70.0%, specificity of 55.3%, PPV of 31.9%, and NPV of 86.2% (Table 3). In Supplementary Tables S1–S3, 2 × 2 tables for evaluation of patients with ESLD, DM, and IVDU are shown. At a cutoff of LRINEC score ≥6, the DM group demonstrated the highest sensitivity (91.3%) and lowest specificity (38.8%) with a high NPV (90.5%). Similarly, the NPV was approximately 90% in the patients with ESLD and no comorbid conditions, whereas the IVDU group had a lower NPV (70.6%). At a cutoff of LRINEC score ≥8, the group with DM had a decreased NPV of 69.4%. Overall, at both cutoffs of LRINEC score ≥6 and 8, all subgroups showed a low PPV from 16.1% to 42.3%. Figure 2 shows ROC curves for total patients and each subgroup. The area under the ROC curve (AUC) was 0.665 for the total population. The AUC and DeLong test for the subgroups were 0.649 (p = 0.902) for ESLD, 0.699 (p = 0.683) for DM, 0.565 (p = 0.034), and 0.653 (p = 0.875) for no comorbidities. The results of DeLong test showed that the AUC of the IVDU group was lower compared with the one for our total study population.
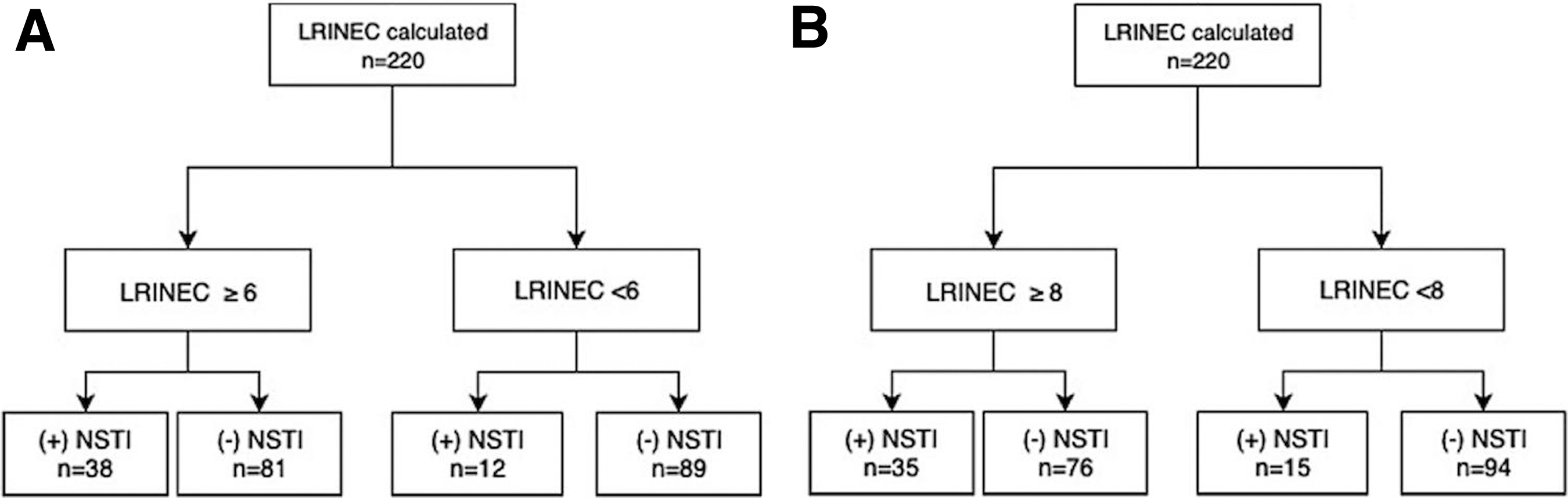
Standards for reporting of diagnostic accuracy studies (STARD) flow diagram. (
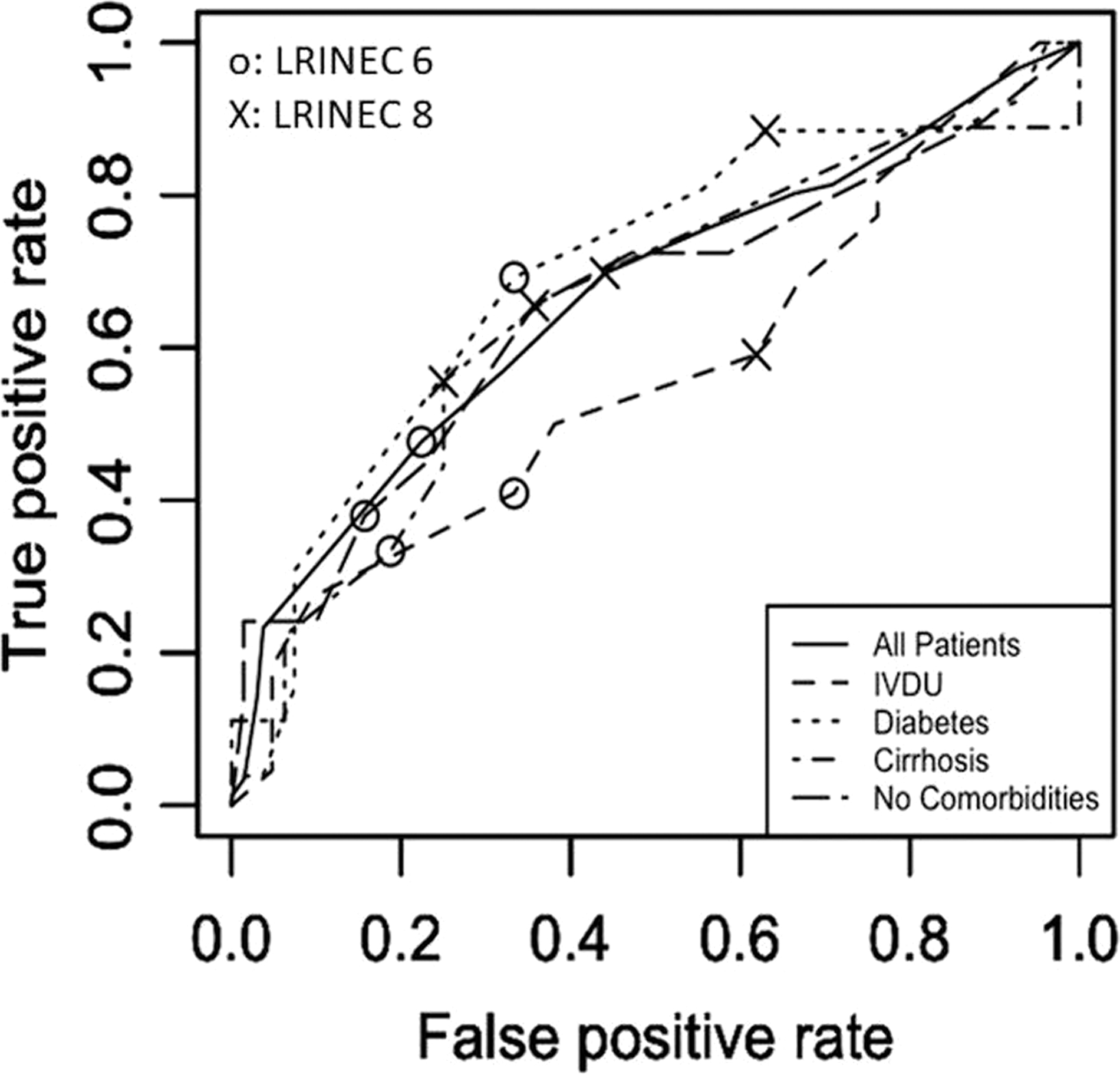
Receiver operator characteristic curve for the LRINEC to predict NSTI. LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis; NSTI = necrotizing soft tissue infection; IVDU = intravenous drug use
Patient Characteristics and Outcomes
ESLD = end-stage liver disease; DM = diabetes mellitus; IVDU = intravenous drug use; IQR = interquartile range;
LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis; HLOS = hospital length of stay.
Summary of LRINEC Score ≥6 Sensitivity, Specificity, PPV, and NPV
ESLD = end-stage liver disease; DM = diabetes mellitus; IVDU = intravenous drug use; PPV = positive predictive value; NPV = negative predictive value.
Summary of LRINEC Score ≥8 Sensitivity, Specificity, PPV, and NPV
ESLD = end-stage liver disease; DM = diabetes mellitus; IVDU = intravenous drug use; PPV = positive predictive value; NPV = negative predictive value.
Discussion
The results of this study, including patients with high prevalence of ESLD, DM, and IVDU, suggest that the LRINEC scoring system carries a nearly 70% false-positive rate. On the other hand, whereas the diagnosis of NSTI can only be definitively excluded through clinical judgement, a negative LRINEC score in patients with ESLD or DM may be a useful adjunct for the provider. Compared with the original study by Wong et al. [2], which demonstrated a PPV of 92.0%, our study showed an extremely low PPV in total study patients (31.9%) and across subgroups. These discrepancies in the results may be caused by a different mix of patients with pre-existing conditions in the two studies. We believe that these findings are important for care providers to consider when evaluating the patients with suspected NSTI. In other words, the LRINEC should be treated simply as another imperfect tool in the provider's armament, such as laboratory and imaging findings, rather than a definitive diagnostic modality. Ultimately, the judgment of the experienced provider should be considered the gold standard.
To date, multiple studies have reported inadequate sensitivity of the LRINEC score, which was supported by our study finding of an overall sensitivity of 76.0% [3,17]. The inadequacy of the test characteristics is particularly pronounced in the subgroups of patients with IVDU, which is known to be associated with an increased risk of NSTI. Although the incidence of NSTI in IVDU patients has been studied extensively, the utility of LRINEC in their diagnosis remains unknown [18–20]. Our results suggest that the LRINEC is of little value overall for these patients, likely because of local infection/abscesses that cause a proinflammatory state, as well as direct system effects of drug use, such as increase in WBC and CRP [18,21,22]. Thus, the diagnosis should be made primarily with clinical findings and imaging adjuncts such as computed tomography [23,24].
In contrast, the sensitivity was found to be high at 91.3% in the DM group, whereas also carrying a poor specificity of 38.8%. The tendency for patients with diabetes to be disproportionately positive on the LRINEC is likely because of poor glucose control, leading to elevated serum glucose levels and higher baseline inflammatory markers, a sequela of diabetic disease. These findings are corroborated in other studies, which similarly found the specificity of the LRINEC to be low in patients with diabetes [25]. Furthermore, it is common for these patients to have a baseline elevated creatinine level from diabetic nephropathy. Thus, our study suggests that although the LRINEC score has a higher sensitivity for detecting NSTI among patients with diabetes, the elevated false-positive rate may skew differential diagnoses and lead to more resource intensive clinical workup.
Although ESLD is a well-described risk factor for NSTI, we believe this study is the first to analyze the validity of LRINEC for use for diagnosis in patients with cirrhosis [26,27]. Huang et al. [28] have described LRINEC as an adjunct to predict mortality in specific patients with Vibrio vulnificus NSTI, but did not find it useful compared with the model of end-stage liver disease (MELD) and did not study its potential for diagnosis. In our study, we noted that the subgroup with ESLD had moderate sensitivity and specificity at a cutoff of LRINEC ≥6, with generally low PPV and high NPV. The low PPV (27.8%) is likely caused by elevated creatinine in these patients (secondary to underlying hepatorenal syndrome) and hyponatremia [29]. Our results suggest that though LRINEC may be a useful adjunct in patients with ESLD, particularly as a screening modality to rule out the diagnosis, it should be used cautiously when it is positive given its low PPV.
There are several limitations to this study. First, although the results of microbiology studies were available for our study patients, microbiology subtypes of NSTI could not be determined because of the retrospective nature of our study [30]. It is well described that patients with type 2 NSTI are more likely to present with signs of organ failure. The accuracy of LRINEC in these patients might be different from patients with type 1 NSTI.
Second, other high-risk groups of patients, such as immunocompromised either through neoplastic processes, autoimmune disorders, steroid use, or recipients of chemotherapy or radiotherapy, were not stratified or analyzed as a subgroup, because only a small number of our study patients were reported to have these conditions. These patients have been found to be at generally higher risk, most likely because of delayed presentation [31]. In addition, other comorbid conditions, such as obesity and smoking history could not reliably be controlled for in this study, because not all patients had body mass index or smoking history recorded. Similarly, conditions that artificially increase the value of individual LRINEC laboratory data, such as renal failure or metabolic disease, including alcohol abuse without liver disease, were not individually controlled, producing another possibly source of confounding.
Third, although most of the consultations were from the emergency department (84%), some did come from other inpatient services where antibiotic therapy may have already been initiated. Although delays in surgical consultation were unlikely because of our institutional protocol in which acute care surgery service receives all emergent surgical consultations, this may act as a confounding variable because of partial treatment and delay of symptom presentation. Of the 35 patients who were admitted to another inpatient service, only three patients were notable for a delay in surgical consultation more than six hours after admission.
Finally, beyond pathologic analysis, there is no gold standard for the diagnosis of NSTI. Many of the positive diagnoses of NSTI used for analysis in this study were based on surgeon's assessments in the operating room. Although intra-operative findings are often conclusive, particularly if the classic “dishwater” discharge and compromised tissue is encountered, these findings are ultimately subjective [32].
Conclusions
The LRINEC score may not be used as a sole decision-making tool with regards to NSTI diagnosis in a group of patients with known risk factors. A negative LRINEC score could be used as an adjunct to rule out NSTI given its high NPV, whereas a comprehensive evaluation including detailed history taking, physical examination, and adjunctive radiographic images, such as computed tomography, will be still required in the patients with a positive LRINEC score. Further studies are warranted to develop a novel prediction model tailored by different patient comorbid conditions.
Footnotes
Acknowledgments
This study was approved by the Institutional Review Board of University of Southern California (#HS-18-005537). A waiver of consent was granted as the research involved no more than minimal risk to study subjects.
Presented at the Southern California Chapter of the American College of Surgeons Annual Scientific Meeting, Santa Barbara, California, January 2019.
Funding Information
Neither internal nor external financial support was used for this study.
Author Disclosure Statement
None of the authors have any conflicts of interest to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.