
Abstract
Background:
Infections with multi-drug–resistant organisms (MDROs) may be difficult to treat and prolong patient hospitalization and recovery. Multiple MDRO coinfections may increase the complexity of clinical management. However, association between multiple MDROs and outcomes of patients who undergo surgery is unknown.
Patients and Methods:
We performed a retrospective, cross-sectional analysis of the 2016 National Inpatient Sample for identified by International Classification of Disease, 10th Revision Clinical Modification (ICD-10-CM) diagnosis codes associated with multi-drug-resistant organisms: methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), multi-drug–resistant gram-negative bacilli, and Clostridioides difficile infection (CDI). Admitted patients with diagnosis codes for MDROs were cross-matched with codes for common general surgery procedures. Outcomes of interest included length of stay and mortality. Weighted univariable and multivariable analyses accounting for the survey methodology were performed.
Results:
Of 1,550,224 patients undergoing surgery in 2016, 39,065 (3%) admissions were diagnosed with an MDRO and 1,176 (0.1%) were associated with dual MDROs diagnoses. Patients diagnosed with one MDRO were hospitalized three times longer (17.3 days; 95% confidence interval [CI], 16.8–17.7) and patients diagnosed with two MDROs five times longer (31.6 days; 95% CI, 27.0–36.2; p < 0.0001) than undiagnosed patients (6.1 days; 95% CI, 6.1–6.1; all p < 0.0001). On multivariable analysis, the strongest predictor of mortality was a diagnosis of two MDRO infections (odds ratio [OR], 4.8; 95% CI, 3.16–7.21; p < 0.0001). The second strongest predictor was diagnosis of single MDRO infection (OR, 2.9; 95% CI, 2.64–3.20; p < 0.0001).
Conclusion:
Presence of an MDRO was associated with increased odds of mortality and length of stay in admitted surgical patients. Interventions to reduce MDRO infection among surgical patients may reduce hospital length of stay and mortality.
Multi-drug–resistant organisms (MDROs) are encountered commonly in hospitalized patients. In 2019, 2.8 million antibiotic-resistant infections and 35,000 MDRO-infection related fatalities were reported by the U.S. Centers for Disease Control and Prevention (CDC) [1]. Common examples of MDROs include methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus spp. (VRE), Clostridioides difficile infection (CDI), and multi-drug–resistant gram-negative bacilli. Acquisition of a single MDRO infection increases hospital length of stay, morbidity, and mortality [2,3]. Analysis of the Medical Expenditure Panel Survey concluded antibiotic resistance added $1,383 to the total cost of each patient's care and cumulatively, cost healthcare payers more than $2 billion annually [4,5].
Surgical procedures inherently violate or weaken natural protective barriers preventing infection and can predispose patients to bacterial infections. Although pre-operative administration of antibiotic agents provides protective coverage against surgical site infection [6], antibiotic use also predisposes patients to develop drug-resistant infections through selection of resistant bacteria [7,8]. This double-hit of impaired immune response and increased selective pressure puts surgical patients at risk for development of multiple types of MDRO infections. Most existing studies assessing impact of MDROs on patient outcomes, particularly among patients undergoing surgery, only focus on single-organism MDRO infections. This study sought to characterize patients co-diagnosed with more than one MDRO better, a rare population, and address knowledge gaps through analysis of a nationally representative dataset.
Patients and Methods
In this cross-sectional, retrospective study, we used data from the Agency for Healthcare and Quality (AHRQ), Healthcare Cost and Utilization Project's (HCUP) National Inpatient Sample (NIS) from 2016 [9]. When analyzed, NIS is weighted to provide national estimates for inpatient utilization, charges, quality, and outcomes for more than 97% of the U.S. population. This sample is built from approximately 20% of all discharges from 4,573 U.S. community hospitals [10].
Inclusion criteria were any patients ≥18 years undergoing a general surgery procedure as defined by the CDC National Healthcare Safety Network (NHSN) [11]. Procedures were identified by International Classification of Disease, 10th Revision Procedure Coding System (ICD-10-PCS) coding [12]. These procedures included appendectomy, bile duct, liver, or pancreatic surgery, colon surgery, exploratory abdominal surgery, gallbladder surgery, gastric surgery, herniorrhaphy, rectal surgery, small bowel surgery, and spleen surgery (Supplementary Table S1). Infection with an MDRO class was defined by International Classification of Disease, 10th Revision, Clinical Modification (ICD-10-CM) diagnosis codes [13]: methicillin-resistant Staphylococcus aureus (MRSA; A41.02, A49.02, B 95.62, J15.212, Z22.322, Z86.14); vancomycin-resistant Enterococcus (VRE; Z16.21, Z16.22); multi-drug–resistant gram-negative bacilli (A41.5, A41.59, B96.2, Z16.1, Z16.3); and Clostridioides difficile infection (A047). Multi-drug–resistant organisms were grouped into composite codes by pathogen for analysis. Procedure codes were cross-matched with infection diagnosis codes.
Demographic parameters assessed included age, gender, presence of comorbidities, and race/ethnicity. Comorbidities were defined by Elixhauser Elixhauser Comorbidity Software, version 2016.2 [14]. A single composite comorbidity score was calculated for each patient. Univariable and multivariable analyses were performed to assess associations between independent risk factors and primary outcomes of mortality and hospital length of stay.
Bonferroni correction was applied to the priori p value to determine significance for univariable and multivariable analyses (p < 0.0025). Non-normally distributed continuous variables were analyzed using Wilcoxon rank sum and categorical parameters were analyzed using χ2. Odds ratios with 95% confidence intervals are reported.
All significant parameters from the univariable analysis were included in the multivariable logistic regression with death as the dependent variable. Covariables were added and subtracted to find the model with the lowest Akaike information criterion (AIC)/Bayesian information criterion (BIC). This model was validated by graphing a receiver operating characteristic (ROC) and calculating the area under the curve. Ordered logistic regression was performed to assess stepwise increases in length of stay. Weighted values are reported unless otherwise specified. All analyses were performed using Stata, version 16 (StataCorp, College Station, TX). Cell contents with 10 cases or less are reported as <11 in accordance with the HCUP user agreement [15]. Figures were generated using GraphPad Prism version 8.2.1 (GraphPad Software, Inc, San Diego, CA). This study was classified exempt by the Stanford Institutional Review Board because of a lack of identifiable patient information.
Results
In 2016, there were 1,550,224 patients ≥18 years admitted to a hospital who underwent a general surgery procedure (Table 1). Of these admissions, 39,065 (3%) were associated with a diagnosis of an MDRO. A total of 17,518 (47%) admissions had a diagnosis of CDI, 16,742 (45%) had diagnosis of MRSA infection, 3,100 (8%) had diagnosis of a multi-drug–resistant gram-negative bacillus (GNR), and 1,705 (4%) had a diagnosis of VRE. 1,176 patients (0.1% of total patient population and 3% of patients with one MDRO) were diagnosed with two MDRO diagnoses. Triple MDRO co-diagnoses were excluded from analysis given low cell count in accordance with the HCUP user agreement.
Epidemiology of Infections by Multi-Drug–Resistant Organisms During Hospitalization after General Surgery Procedures in the United States, 2016
After Bonferroni correction, a significant p < 0.0025.
Values are reported as: frequency (percentage of subpopulation).
Values <11 are not reported in accordance with HCUP data use agreement.
HCUP = Healthcare Cost and Utilization Project; C. difficile = Clostridioides difficile; MRSA = methicillin-resistant Staphylococcus aureus; GNR = multi-drug–resistant gram-negative bacilli; VRE = vancomycin resistant Enterococcus spp.
In comparison with all surgical patients, patients diagnosed with any MDRO were older. Fifty-nine percent (n = 510,912) of patients who underwent surgery were female. Female gender was associated with a decrease in the proportion of patients with an MDRO for all evaluated organisms except VRE. The proportion of patients with congestive heart failure, diabetes mellitus with chronic conditions, and renal failure at time of admission was higher in all MDRO infection groups than among total surgical patients. Peripheral vascular disease was more prevalent among patients with co-diagnosis of CDI (8% vs. 4%; p < 0.001) or MRSA (6% vs. 4%; p < 0.0001). Metastatic cancer was a more common diagnosis in patients with CDI (6%; p < 0.0001) and GNR (7%; p = 0.0025). Mean Elixhauser comorbidity scores for all four MDRO infection groups were higher than for surgical patients without a MDRO diagnosis (p < 0.0001).
Although diagnosis of infection during hospitalization with a concomitant general surgery procedure was low, associated mortality with infection diagnosis was high. In comparison with the mortality rate of 2% (31,470) for surgical patients with no MDRO diagnosis, 11% (1,860) patients with CDI diagnosis died, 6% (963) with MRSA died, 11% (338) with GNR died, and 6% (94) with VRE died (all p < 0.0001). With combined infection groups, patients that had any one MDRO had a mortality rate of 8% (3,125) and patients that had any two MDROs had a mortality rate of 13% (153; all p < 0.0001).
There were 1,176 patients with two MDRO diagnoses reported. The most common type of dual MDRO co-diagnoses was MRSA and CDI, occurring in 622 patients and representing 53% of all dual co-diagnoses. Clostridioides difficile infection and GNR were co-diagnosed in 182 patients (15% of dual diagnoses) and CDI and VRE were co-diagnosed in 140 patients (12% of dual diagnoses). Methicillin-resistant Staphylococcus aureus and GNR were co-diagnosed in 114 patients (10% of dual diagnoses) and MRSA and VRE were co-diagnosed in 99 patients (8% of dual diagnoses). Vancomycin-resistant Enterococcus and GNR were co-diagnosed in only 20 patients (1% of dual diagnoses).
Patients with MDRO diagnosis had substantially increased length of stay than did patients without an MDRO diagnosis (6.1; 95% confidence interval [CI], 6.1–6.1 days). Mean length of stay for patients with an MDRO diagnosis (17.3; 95% CI, 16.8–17.7) was three-fold longer than patients without an MDRO diagnosis (Fig. 1). Mean length of stay for patients with two MDRO diagnoses (31.7; 95% CI, 27.2–36.3) was five-fold longer than patients without an MDRO diagnosis. Mean length of stay was longest for patients with CDI and GNR co-diagnoses (36.7; 95% CI, 26.2–47.2 days). This is six times longer than the mean length of hospitalization of patients without MDRO). The shortest mean length of stay of a dual MDRO co-diagnoses combination was observed in CDI and VRE (22.4; 95% CI: 17.9–26.8 days) and was still 3.6 times longer hospitalization than patients without MDRO diagnosis.
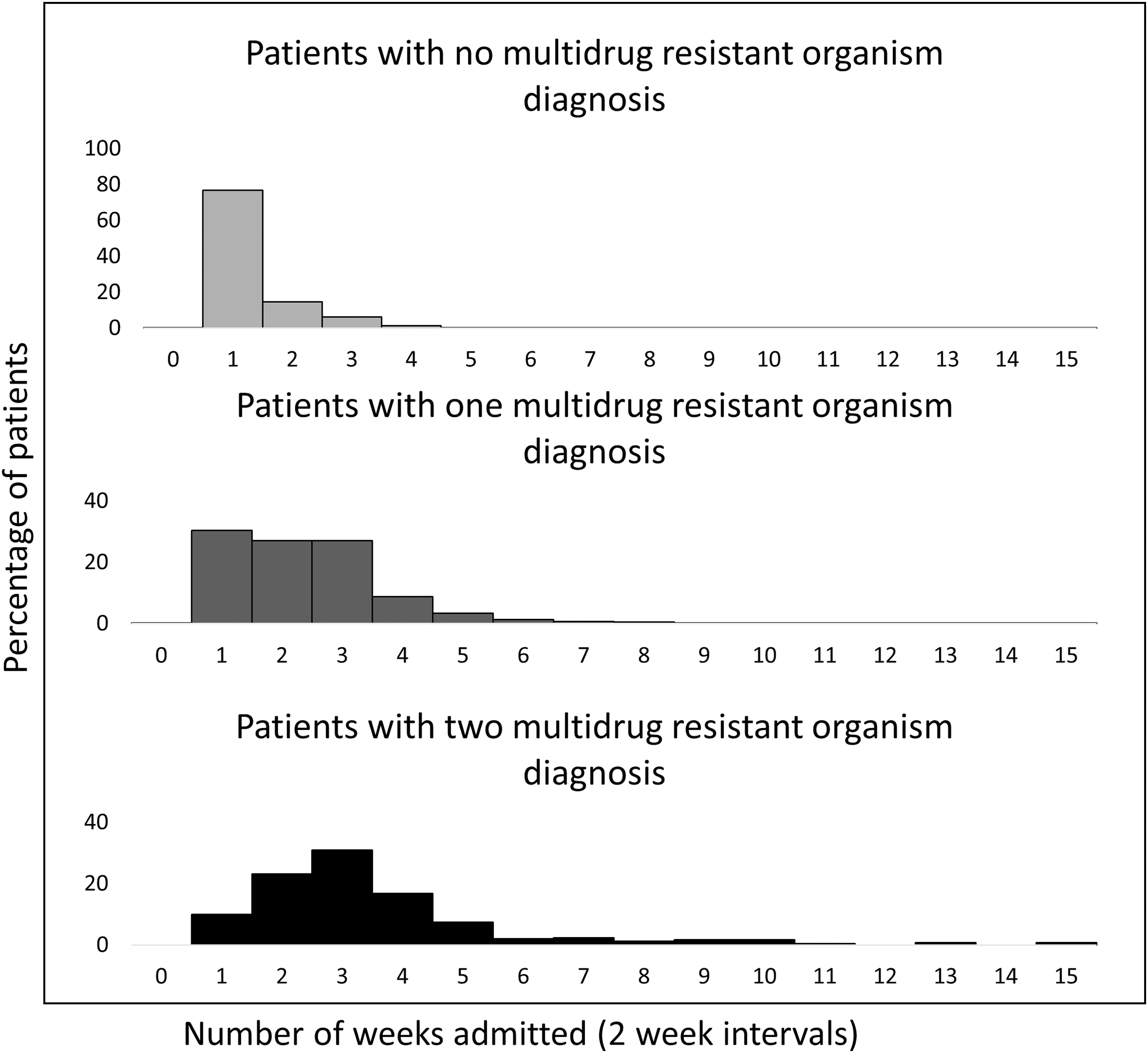
Length of stay among admitted patients undergoing general surgery procedures by co-diagnosis of one or more multi-drug–resistant organisms—United States, 2016.
Prevalence of MDRO infections and mortality associated with general surgery during a hospitalization is recorded in Table 2. Compared with patients without an MDRO diagnoses, patients with a diagnosis of an MDRO had higher mortality with every surgery. Surgical procedures with particularly pronounced increases in mortality included bile duct, liver, and pancreatic surgery (2%–8%), colon surgery (3%–12%), exploratory abdominal surgery (3%–9%), gastric surgery (2%–8%), and spleen surgery (6%–13%; all p < 0.0001; Fig. 2). The lowest mortality rate for patients infected with one MDRO was 3% after appendectomy, rectal surgery, and small bowel surgery. Of dual co-diagnosis patients, those with MRSA and GNR were associated with a mortality rate of 17% (n = 20), whereas 14% mortality was noted for two groups: CDI and GNR and CDI and MRSA.

Trends in mortality among admitted patients undergoing specific general surgery procedures by co-diagnosis of one or more multi-drug–resistant organisms—United States, 2016.
Impact of Co-Diagnosis of Multi-Drug–Resistant Organism and Fatality after General Surgery Procedures—United States, 2016
Values <11 are not reported in accordance with HCUP data use agreement.
HCUP = Healthcare Cost and Utilization Project; MDRO = multi-drug–resistant organism.
On multivariable analysis, diagnosis with one MDRO was associated with increased odds of death by 2.9 (95% CI, 2.6–3.2; p < 0.0001), whereas co-diagnosis by two MDROs was associated with increased odds of death by 4.8 (95% CI, 3.1–7.2; p < 0.0001). Several comorbid diagnoses were also found to be associated with increased mortality. These included peripheral vascular disease (odds ratio [OR], 2.0; 95% CI, 1.8–2.2), congestive heart failure (OR, 1.6; 95% CI, 1.5–1.8), and metastatic cancer (OR, 1.3; 95% CI, 1.2–1.4; all p < 0.0001). Other associations of increased odds of death included increased age (OR, 1.5; 95% CI, 1.5–1.5) and higher Elixhauser comorbidities index (OR, 1.3; 95% CI, 1.2–1.3). The multivariable logistic regression model had an AIC of 51,569.86 and a BIC of 51,728.84. The area under the ROC curve was 0.8.
An ordered logistic regression was run to assess the impact of significant parameters from the univariable analysis on hospital length of stay. The odds of extending inpatient length of stay by two weeks increased by 5.7 (95% CI, 5.5–6.0) in patients with a single MDRO diagnosis, and by 18.6 (95% CI, 14.5–23.9) in patients with dual MDRO co-diagnoses. In addition, the odds of an extended hospitalization increased with increasing age (1.2; 95% CI, 1.2–1.2), presence of congestive heart failure (1.2; 95% CI, 1.1–1.2), and the composite Elixhauser Score (1.5; 95% CI, 1.5–1.5).
Discussion
Our study is the largest national evaluation of the epidemiology of hospitalized surgical patients diagnosed with MDROs and is the first study to analyze associations between MDRO co-diagnoses during hospitalization with a general surgery intervention and outcomes of mortality and length of stay. Most existing studies assessing impact of MDROs on patient outcomes, particularly among patients undergoing surgery, only focus on single-organism MDRO infections. For example, patients recovering from pancreaticobiliary surgery who developed surgical site infections had a longer length of stay than patients without infections (19 vs. 10 days; p < 0.0001) [16]. Similarly, patients with CDI had higher rates of post-operative 30-day mortality (5.2% vs. 1.0%; p < 0.001) as well as longer hospitalizations (17.9 vs. 3.6 days; p < 0.001) compared with patients without CDI [17]. In yet another example, patients with complicated intra-abdominal infections colonized by an MDRO had more than twice length of stay than patients without an MDRO infection (21 vs. 9 days; p < 0.001) [18]. Our national analysis of single and dual MDRO co-diagnoses in patients undergoing general surgery procedures support these prior findings. In addition, we conclude that diagnosis of one or more MDRO is strongly associated with increased odds of mortality.
Interactions between patient comorbidities and mortality associated with an MDRO infection are complex, and interpretations of the odds associated with presence of one or more MDRO should be made with caution. For example, increased age, peripheral vascular disease, congestive heart failure and metastatic cancer were found to be associated with increased mortality on multivariate analysis. However, each of these conditions may also independently increase the risk of death from MDRO. For example, patients with these comorbidities may have increased exposure to antibiotic agents or MDROs during frequent interactions with the healthcare system [19]. These comorbidities may additionally compromise innate ability to acutely respond to MDRO infection. Despite this potential for effect modification, the high odds of mortality associated with MDRO infections underscores the critical need for the development of an MDRO risk assessment tool. Future risk models, ideally established from prospective cohorts of surgical patients, should consider potential multiplicative and additive effects between MDROs, and potential for effect modification of medical comorbidities.
Length of stay in the hospital was dramatically increased among patients with MDRO infections. Our findings that patients diagnosed with one MDRO were hospitalized three times as long as patients without a MDRO diagnosis is comparable to a national case-control study in China that found on average, patients with one MDRO infection were hospitalized 14 days longer than patients without infections [2]. Length of stay is a complex measurement susceptible to confounding by a number of parameters: number of comorbidities, severity of condition, and intensive care unit admission, among others [20]. Consequences of staying in the hospital longer include greater exposure to antibiotic agents, environmental contagions, and bacterial transmission from healthcare workers [21,22]. Infection by an MDRO and subsequent need for treatment may prolong hospitalization, especially if patients are treated with agents ineffective against an MDRO. Delays in diagnosis of an MDRO can also prolong hospitalization [23]. Irrespective of the underlying etiology, it is clear that a diagnosis of an MDRO is a harbinger of prolonged hospitalization.
Prevalence of MDRO dual diagnoses in our study were validated by a multi-site German study with 896,822 patients that concluded similar results [24]. In that German study, 5% of patients with an MRSA diagnosis had a concomitant co-diagnosis of an MDRO, and 15% of patients with VRE has a concomitant co-diagnosis of an MDRO. Despite these similarities, there was a marked difference in mortality rate among patients co-diagnosed with MRSA and VRE. Compared with the 24% mortality rate (n = 16) observed in the German study, there were fewer than 11 deaths recorded in NIS. Our findings may be explained by three hypotheses. First, Germany may have different environmental and human-population conditions impacting antibiotic resistance. Among the factors that directly influence susceptibility to antibiotic resistance are antibiotic agent exposure [25,26], penicillin allergies [27,28], and food supply chain in the population [29]. Second, our study may underestimate the true burden of MDRO infections given our focus on payer data whereas the German study validated each diagnosis with microbial analysis. Third, our study population was observed almost a decade after the 2007–2009 German study, and it is possible that mortality from the combined impact of infection with MRSA and VRE has since decreased as a result of improved knowledge regarding diagnostics, treatment, and prevention.
Infection with Clostridioides difficile was the most common singular MDRO diagnosis, CDI and MRSA was most common co-diagnosis, and co-diagnoses of CDI with other pathogens were more common than any other dual pathogen combination. Of the 17,518 CDI patients, 944 patients had a secondary diagnosis of MRSA, GNR, or VRE. One potential explanation for CDI preponderance is the large number of colonized, but uninfected patients presenting for surgery. Once a surgical site is created and peri-operative antibiotic agents administered, drug-resistant Clostridioides difficile progresses from colonization to infection. In addition, this same antibiotic administration event may also increase likelihood of concomitant or parallel infections. A second possible explanation for the high CDI prevalence observed is that patients are developing infections during hospitalization. Clostridioides difficile spores are resistant against many commonly used disinfectants [30] and can survive for months to years in hospital environments [31,32]. Yet another explanation is that genetic variations favoring drug resistance can persist in CDI populations in the absence of antibiotic selective pressure [33].
Compared with all surgical patients, our study found that CDI and MRSA patients were more commonly white, and less commonly Hispanic (p < 0.0001). In contrast, GNR patients were more commonly black, and less commonly Hispanic. Studies have shown that racial and ethnic minorities face barriers to accessing care and as result, have worse health outcomes [34,35] and higher chronic disease burdens [36] than non-minority white patients. Although this study was not conducted with an intention to analyze race, a curious observation inverse of our expectations was decreased diagnostic prevalence of any MDRO in Hispanic patients, whereas the only MDRO diagnosed with higher prevalence in black patients was GNR. Further studies are needed to better characterize covariates potentially associated with race and ethnicity that may explain these findings.
This study has several limitations. First, this was a retrospective study so there may exist unknown potential confounders and causality cannot be assessed. Second, quality of diagnosis codes is dependent on the quality of coders at each institution which could introduce misclassification bias. In an effort to decrease the effect of coding errors, composite infection codes were created. By creating codes that were organism-specific versus disease-site specific, analytic emphasis was placed on the organism, while minimizing additional variance that could be introduced with site-specific (ie, pneumonia versus sepsis versus unspecified) coding errors. Third, as a cross-sectional study, there is potential for atomistic fallacy, where assumptions about populations are made based on aggregation of individual level data in a snapshot of time. In this population, association of susceptibility to infection with history of previous infection or antibiotic agent exposure is unknown. Fourth, temporality between intervention codes and diagnosis codes is not possible in this dataset. Fifth, lack of microbiologic data about pathogens limits more granular risk assessments. Sixth, there are also no follow-up data and thus, long-term differences between co-colonized patients and those with one or none MDRO infections are unknown. Finally, this study was unable to distinguish between hospital-acquired and community-acquired MDROs (or co-colonization of both).
Conclusion
Multi-drug–resistant organism diagnosis is the greatest predictor of increased odds of death and lengthened hospitalization in surgical patients over the age of 18. Association with an additional MDRO increases with age after 65 years, and in patients with peripheral vascular disease, congestive heart failure, and metastatic cancer. For every general surgical procedure, odds of death and length of stay increases with an MDRO diagnosis and increases even more with dual MDRO diagnoses. Among reported patients with dual co-diagnoses, CDI and VRE were associated with the highest mortality rate and CDI and GNR were associated with the longest length of stay. Interventions to decrease infection with MDRO may help reduce mortality and length of stay of patients undergoing surgery as an inpatient.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.