
Abstract
Background:
Surgical site infections (SSIs) represent an economic burden to healthcare systems. The use of negative pressure wound therapy (NPWT) for SSI prophylaxis remains uncertain.
Methods:
A systematic literature search was conducted in Medline/PubMed, CINAHL, and Web of Science for relevant studies. The primary outcome was the evaluation of the effectiveness of NPWT for prophylaxis of SSI rates in general abdominal surgery. Secondary outcomes were rates of seroma and wound dehiscence, length of hospital stay, and re-admission rates. The statistical analysis was performed with random effect models.
Results:
A total of 3,193 patients from 20 articles (six randomized controlled trials [RCT], three prospective, eight retrospective, and three ambispective studies) were analyzed. Negative pressure wound therapy was associated with decreased rate of SSIs compared with standard dressing in a pooled analysis of non-randomized studies and RCTs (0.57; 95% confidence interval [CI], −0.4 to 0.8; p < 0.001). This result, however, needs to be challenged because of a significant statistical heterogeneity of the included studies (I2 = 71%; p < 0.01). A separate analysis of the six RCTs failed to confirm the superiority of NPWT (0.64; 95% CI, −0.4 to 1.04; p = 0.07), also disclosing significant heterogeneity. The analysis of secondary outcomes was only possible in combination of randomized and non-randomized studies because of incomplete datasets in RCTs. Re-admission rates were lower after NPWT and no difference was observed for the incidence of seroma, wound dehiscence, and length of hospital stay.
Conclusions:
Based on available evidence, the routine use of NPWT for SSI prophylaxis after laparotomy in general abdominal surgery cannot be generally recommended.
Surgical interventions are common with one estimated procedure for every 22 person each year worldwide, with even higher numbers in high-income countries [1]. Generation of a surgical incision is an unavoidable part of any surgical intervention. Development of post-operative infection of the surgical site is a common complication and causes considerable distress to patients and substantial cost to healthcare systems [1,2]. Surgical site infections (SSIs) are the most common type of hospital-acquired infections and cause more than $1.6 billion in hospital costs in the United States alone [3,4], whereas the likelihood of post-operative mortality rate more than doubles if an SSI is present. Rates vary between 0.01 and 0.45 depending on type of procedure [3–6]. High healthcare economic burden and the physical, social, and emotional aspects of patients suffering from SSIs prompted the surgical community to focus substantial effort and resources into prevention of SSIs in recent years.
The measures aimed at reducing SSIs can be divided into three phases including pre-operative, intra-operative, and post-operative. The value of pre-operative and intra-operative measures has been proven across studies and is well established in clinical settings. For the post-operative phase, prophylactic negative pressure wound therapy (NPWT) for closed wounds is emerging as a promising option to reduce SSIs. It has been proposed that NPWT prevents infection by potentially reducing seroma, excess exudate, and subsequent bacterial overgrowth [4], while at the same time assisting in wound healing by increasing microcirculation, improving lymph drainage, and the production of granulation tissue [1].
However, the current literature is not conclusive and has controversial results [1,2,4,7–9]. General abdominal surgery has higher rates of SSIs compared with orthopedic, cardiothoracic, and other types of interventions [3,6] and previous meta-analyses on abdominal surgery have also reported contradicting results [2,10,11]. As a result of new trial results, we conducted this updated systematic review and meta-analysis to re-evaluate the value of prophylactic NPWT in general abdominal surgery after primary wound closure.
Methods
Search strategy and study selection criteria
This systematic review was performed according to Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [12] and as previously reported [13–15]. A comprehensive systematic literature search of the Medline/PubMed, CINAHL and Web of Science databases was conducted in June 2019 with limitation to publications in English and Spanish. A focused updated manual search was conducted in August 2020. The complete search strategy is attached as Supplementary Appendix S1. The review protocol was CRD42020198386. Randomized control trials (RCTs) and non-randomized studies that reported NPWT for prophylaxis of SSI rates compared with standard dressing in general abdominal surgery with primary wound closure were included. Case series (<10), review articles, congress abstract, letters, editorials, or animal studies were excluded.
Data extraction and assessment of methodological quality
The titles and abstracts of the identified studies were screened by two independent researchers (S.A. and V.L.). Disagreements between investigators were resolved by discussion.
Data collection and measures
Descriptive data of the respective study populations were extracted, including dates of recruitment, number of patients, age, gender, body mass index (BMI), information on diabetes mellitus, arterial hypertension, and chronic obstructive pulmonary disease (COPD), American Society of Anesthesiologists (ASA) physical status classification system, cardiovascular comorbidities, history of nicotine abuse, type of surgery, pressure of NPWT, and application of neoadjuvant chemotherapy. Primary outcome was rates of SSI. Secondary outcomes included rates of seroma and dehiscence, length of hospital stay, and re-admission rates. Complications (seroma, dehiscence) were included based on the definitions used by authors of the individual articles. Results were first reported pooled for non-randomized studies and RCT and then separate for RCT.
Data synthesis
Missing mean and standard deviation data were calculated from reported median and range values as reported previously [16]. For quantitative synthesis of comparative studies, a random effects meta-analysis was used, with standardized mean differences reported for continuous outcomes and risk ratios (RRs) for binary outcomes, along with 95% confidence intervals (CI) and two-sided p values for each outcome. All analyses were carried out with rBiostatistics. Heterogeneity between studies in effect measures was assessed using both the χ2 test and the I2 statistic. To test for small-study effects or potential publication bias, the funnel plots were assessed.
Results
Study selection
The flow chart of the study selection is presented in Figure 1. After the initial search, 918 studies were identified. Two studies were added by manual search. After screening by duplicity, title, abstract, and type of study, 41 articles were selected for full-text recover. After the complete review 21 articles were excluded. Finally, a total of 3,193 patients from 20 articles (six RCTs, three prospective, eight retrospective, and three ambispective studies) were included in the meta-analysis [4,5,8,17–33]. The funnel plot disclosed the presence of asymmetry (Fig. 2).
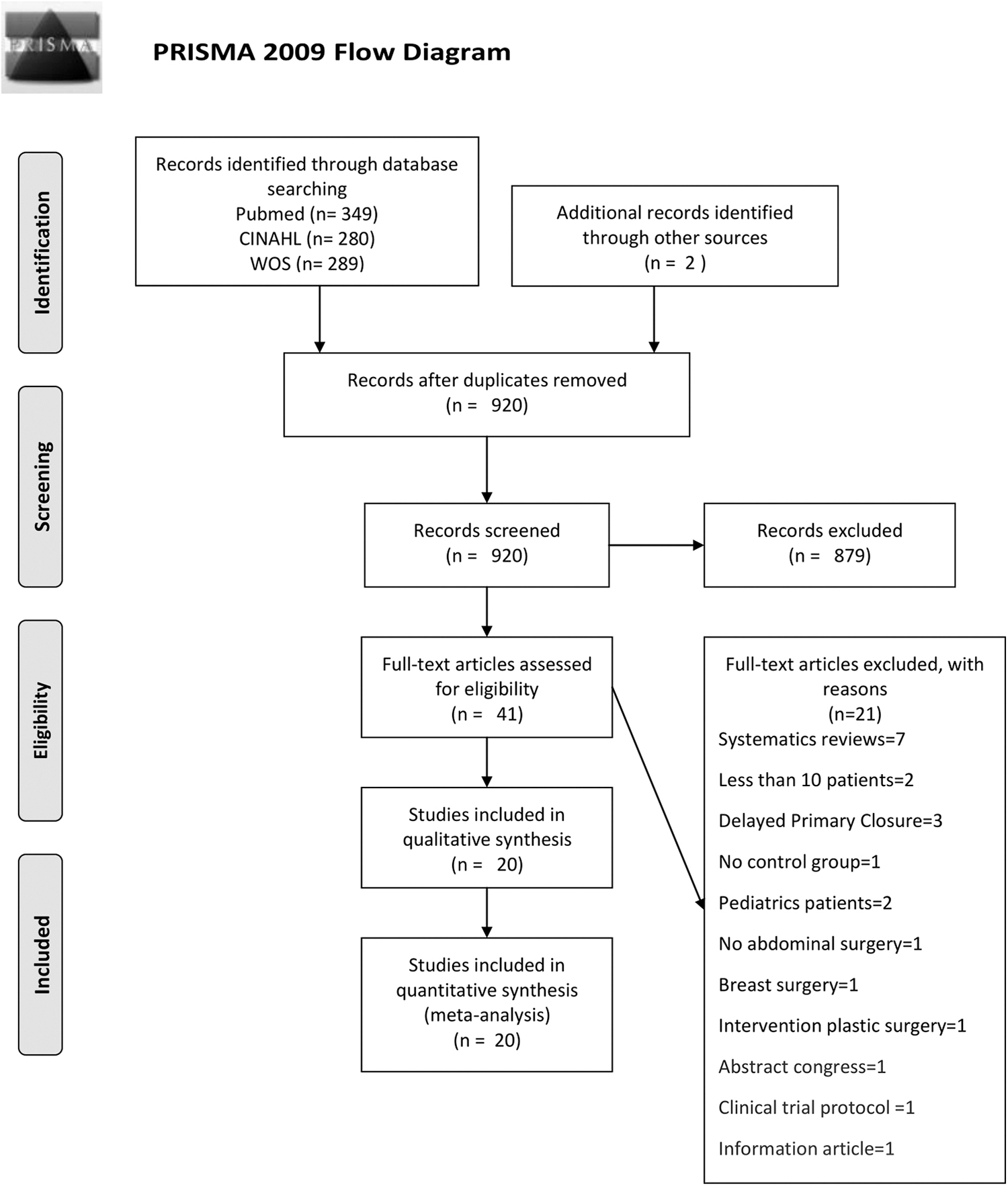
Flow chart of study selection for inclusion in meta-analysis. PRISMA = Preferred Reporting Items for Systematic reviews and Meta-Analyses; WOS = Web of Science.
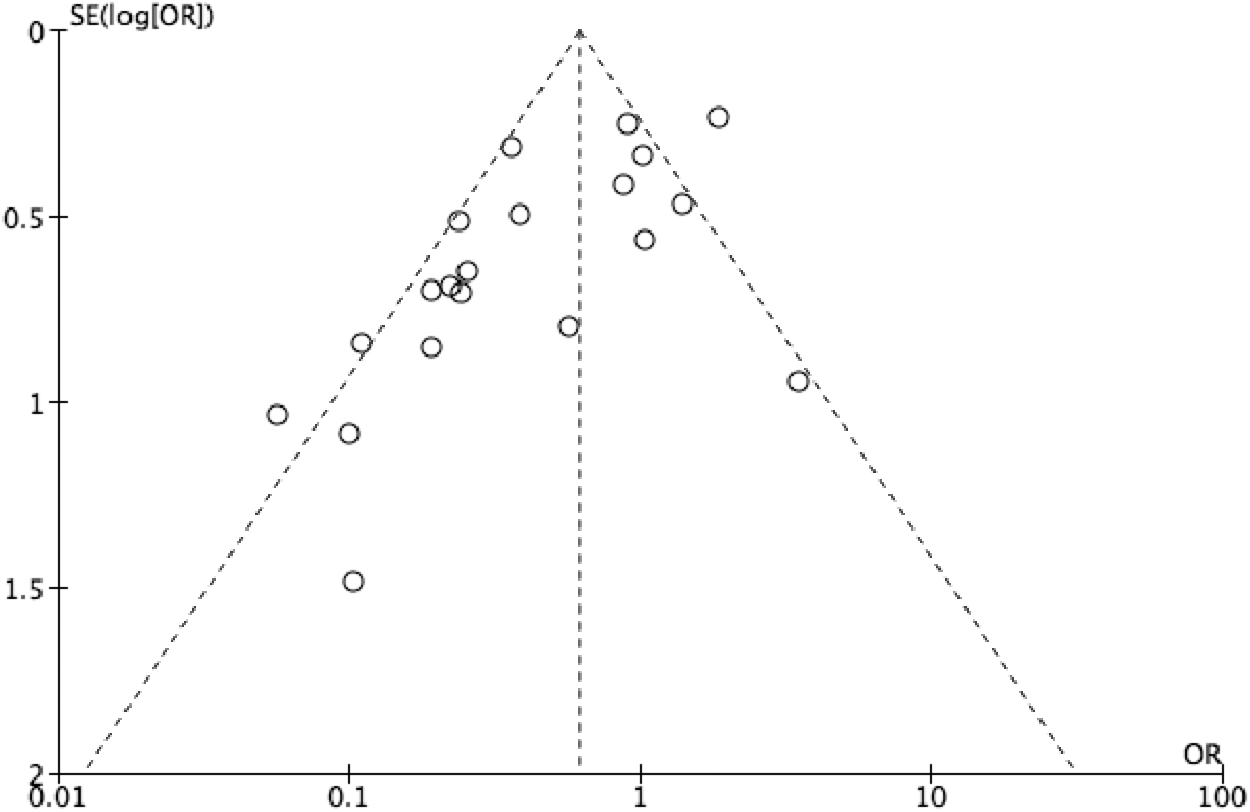
Funnel plot. Individual points correspond to published rates from individual studies. The wide distribution and asymmetry suggest the presence of a publication bias.
Patient and NPWT characteristics
Five studies included patients undergoing colorectal surgery, three studies included those undergoing pancreatic surgery, two studies those only undergoing abdominoperineal resections, and two studies those undergoing diverting loop ileostomy reversal only. The remaining eight studies included open surgery for gastrointestinal, colorectal, pancreatic, and cytoreductive surgeries (Table 1). The parameters of NPWT varied across studies. The negative pressure applied during NPWT ranged between −80 mm Hg and −125 mm Hg, introducing a potential bias. The duration of NPWT varied from three to 10 days.
Summary of the Included Studies According to Demographic Characteristics, Abdominal Surgical Procedure, Type of Negative Pressure Wound Therapy, Complications of the Surgical Site, and Level of Evidence and Recommendation
NPWT = negative pressure wound therapy, SSI = surgical site infection; BMI = body mass index.
Primary outcome in pooled analysis of RCT and non-randomized studies
Twenty studies with n = 3,193 patients reported rates of SSI. In the NPWT group the SSI rate was 0.14 (95% CI, −0.10 to 0.19; n = 1,197) and 0.25 (95% CI, −0.20 to 0.29; n = 1,996) in the standard dressing group. The comparative analysis between NPWT and the standard dressing group demonstrated that NPWT was associated with decreased rates of SSIs compared with standard dressing (0.57; 95% CI, −0.4 to 0.8; p < 0.001; Fig. 3). There was significant statistical heterogeneity in included studies (I 2 = 71%; p < 0.01).

Meta-analysis polling randomized controlled trial (RCT) and non-randomized studies on surgical site infections. The final column represents the relative risk of each study, and the column size represents the study weight in the analysis. The segments represent the 95% confidence interval (CI) of each study. The diamonds represent the overall effect size and the diamond width represents the overall 95% CI.
Secondary outcomes in pooled analysis of RCT and non-randomized studies
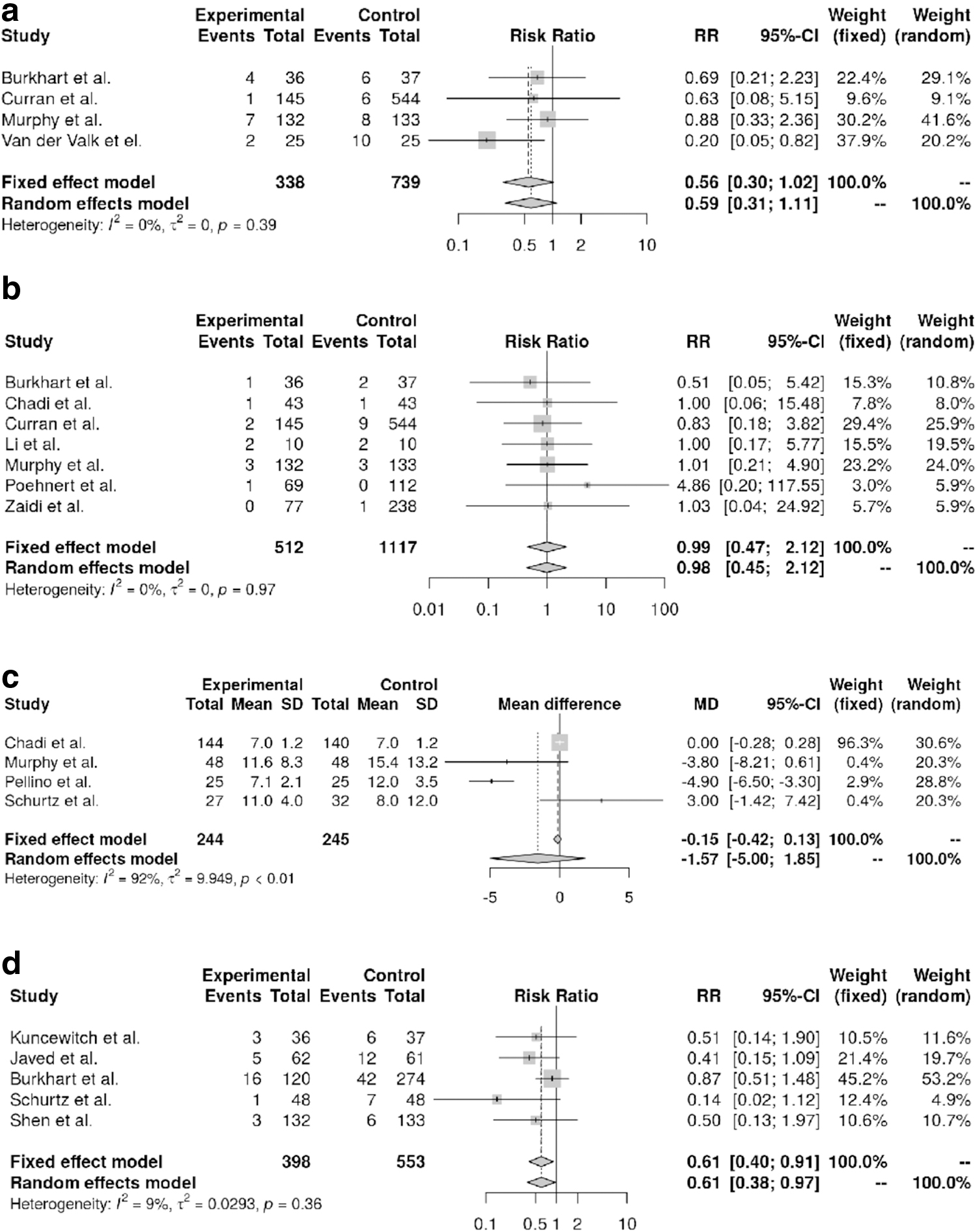
Four studies with n = 1,077 patients reported on seroma rates. In the NPWT group the seroma rate was 0.05 (95% CI, −0.02 to 0.12; n = 338), and 0.09 (95% CI, −0.02 to 0.34; n = 739) in the standard dressing group. The comparative analysis between those in the NPWT and standard dressing groups demonstrated no difference (0.59; 95% CI, 0.31–1.11; p = 0.1; Fig. 4a). There was no significant statistical heterogeneity in included studies (I2 = 0; p = 0.39).
Meta-analysis pooling randomized controlled trial (RCT) and nonrandomized study data on
Seven studies with n = 1,629 patients reported a wound dehiscence rate of 0.03 (95% CI, −0.01 to 0.06; n = 512) in the NPWT group and 0.02 (95% CI, −0.01 to 0.06; n = 1,117) in the standard dressing group. The comparison of NPWT and standard dressing demonstrated no difference in wound dehiscence rates (0.97; 95% CI, 0.98–2.12; p = 0.95; Fig. 4b). There was no heterogeneity in included studies (I2 = 0%; p = 0.97).
Four studies with n = 489 patients reported the length of hospital stay, without difference between NPWT and standard dressing groups (mean difference [MD] −1.57; 95% CI, −5 to 1.85; p = 0.37). Significant heterogeneity was observed in included studies (I2 = 92%; p < 0.01; Fig. 4c). The length of hospital stay was 7.3 (95% CI, −5.4 to 9.3; n = 244) days in the NPWT group and 7.6 (95% CI, −5.4 to 9.8; n = 245) days in the standard dressing group.
The only difference regarding secondary outcomes was observed for re-admission rates. Here, five studies including n = 951 patients, showed a re-admission rate of 0.07 (95% CI, −0.03 to 0.13; n = 398) in the NPWT group and 0.13 (95% CI, −0.09 to 0.20; n = 553) in the standard dressing group. The difference was statistically significant in the comparative analysis (0.61; 95% CI, −0.38 to 0.97; p = 0.035) without significant heterogeneity in included studies (I2 = 9%; p = 0.36; Fig. 4d).
Primary outcome in RCTs
Six studies with n = 980 patients reported rates of SSIs. In the NPWT group the SSI rate was 0.14 (95% CI, −0.8 to 0.24; n = 491). In the standard dressing group, the SSI rate was 0.24 (95% CI, −0.17 to 0.33; n = 489; Fig. 5). The comparative analysis between those in the NPWT and the standard dressing groups demonstrated no difference (0.64; 95% CI, 0.4–1.04; p = 0.071) with significant statistical heterogeneity of included studies (I2 = 59%; p = 0.03).
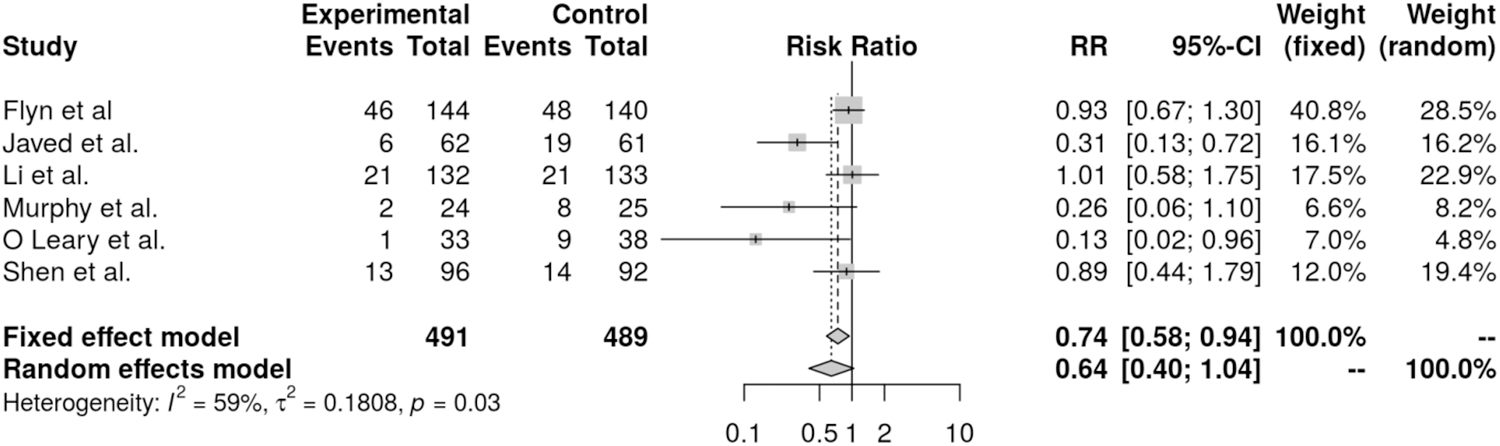
Meta-analysis of six randomized controlled trials (RCT) on surgical site infections.
Secondary outcome in RCTs
There were not sufficient data to perform meta-analysis for secondary outcome in RCTs.
Discussion
In this systematic review, the prophylactic use of NPWT was associated with decreased SSI rates compared with standard dressing in pooled analysis of data from RCTs and non-randomized studies. However, this positive effect of NPWT in SSI prophylaxis is challenged by the observed significant heterogeneity across studies and could not be confirmed in a separate analysis compromising RCTs only.
Surgical site infection constitutes a relevant morbidity in clinical practice, and the importance of this issue is reflected by the RCTs underway [34]. The recent increase of publications in the field created a justification to perform an updated systematic review with meta-analysis. Generally accepted, a systematic review and meta-analysis provides the best available evidence in health care management. Thus, results of systematic reviews are often incorporated into clinical practice guidelines [35]. Regarding the prevention of SSIs by NPWT, three meta-analysis have been reported so far [2,10,11]. In 2018, Sahebally et al. [10] reported a meta-analysis on NPWT for SSI prophylaxis, pooling six observational studies and three RCTs. They concluded that the use of NPWT is associated with reduced SSI rates in general abdominal surgery, despite significant heterogeneity across studies. In a later meta-analysis, Boland et al. [5] included five RCTs, favoring NPWT in their final conclusion despite significant heterogeneity across studies. The sample sizes in the studies included are mostly small and comprise different patient populations, thus the significant heterogeneity in the effect sizes as reflected by the I2 value in summary make the data uninterpretable. Another report from Kuper et al. [2], including five RCTs, concluded that the adoption of NPWT for routine SSI prophylaxis after laparotomy is currently not supported by the available evidence. This report also criticized previous studies regarding their study design, and the inclusion of six observational studies in a meta-analysis.
In our opinion, the topic of SSI after laparotomy is highly relevant, representing a relevant surgical problem and adding a significant load on healthcare costs and patient suffering. Before advocating for the routine use of NPWT, its benefits need to be clarified. The contradictory reports so far motivated us to conduct an updated meta-analysis, including more studies and patients. We indeed identified and included more studies (n = 20) compared with previous meta-analyses. We acknowledge that a meta-analysis pooling observational studies and RCTs may have an inherent bias of non-randomized trials, and such approach is therefore discouraged [36]. Nevertheless, we did so for two reasons. First, the pioneering meta-analysis favoring NPWT reported a similar approach [10]. Second, such meta-analysis is still valuable if no or only few RCTs are available [16].
Significant heterogeneity has been reported consistently by all authors and was also observed in this report. In our view, this finding is worrisome and introduces a dilemma for a meaningful interpretation of available data [37]. Statistical heterogeneity in a meta-analysis can be related to clinical or methodological differences between trials or unreported trial characteristics [38]. In the present report, the included studies presented different study populations with specific and outcome-relevant risk factors. For example, Burkhart et al. [21] divided their patients into two groups based on the presence or absence of two risk factors. These factors were neoadjuvant treatment with chemotherapy prior to surgery and the presence of pre-operative biliary drainage. In patients with no risk factors, rate of infection was 0.04 in the NPWT group and 0.16 in the control group (p = 0.027), whereas in patients with risk factors, infection rates were 0.19 in the NPWT group and 0.5 in the control group (p = 0.015). Similarly, Ocaña et al. [32] highlighted mechanical colonic preparation, Li et al. [5] an incision larger than 20 cm, and Poehnert et al. [23] previous chemotherapy as risk factors for the development of SSIs. Some authors [5,20,28,31] included patients with a higher body mass index or other risk factors (malignancy, tobacco use, diabetes mellitus, immunosuppression, obstructive pulmonary disease, surgery longer than three hours; volume loss >300 mL, malnutrition, emergency surgery, or diffuse arteriosclerosis) that may influence the risk of SSI regardless of the use of NPWT.
In contrast, there are authors who included only clean-contaminated or contaminated and dirty surgeries. Furthermore, some authors did use drains in their interventions, whereas others excluded patients with drains [26,39]. In the trials analyzed in this meta-analysis, there is also a wide margin of lengths of treatment with NPWT, which is another limitation when interpreting the results. Finally, the NPWT method varied also across studies as stated above. Taken together, a general conclusion or recommendation to use NPWT in clinical practice cannot be made based on the available evidence.
The reported significant heterogeneity in non-randomized studies and RCTs prevents reliable interpretation of NPWT in SSI prophylaxis. To address such heterogeneity, we performed a subgroup analysis grouping studies depending on type of surgery. Sufficient data were available only for non-randomized studies with colorectal surgery, pancreatic head resection, and emergency surgery. Whereas studies with colorectal surgery still disclosed a significant heterogeneity (I2 = 81%; p < 0.01; five studies), pancreatic head resection and emergency surgery did not (I2 = 48%; p = 0.14 three studies, and I2 = 0, p = 0.49; five studies, respectively). Note that colorectal surgery included studies with elective and emergency surgery [20,31–33] and also included contaminated and clean wounds, which may explain the observed heterogeneity across studies.
Conclusions
Negative pressure wound therapy is gaining widespread use in surgery for SSI prophylaxis. Several studies have reported promising results. The indication on NPWT use is subjective and depends on each surgeon's preference without unified criteria. However, the current literature does not generally support the routine use of NPWT for SSI prophylaxis after laparotomy, mostly because of the significant heterogeneity across studies, which precludes a meaningful interpretation of the available data. Finally, additional studies, preferably RCTs, are required prior to recommendation of NPWT as a routine in general abdominal surgery. Future studies should be conducted with homogeneous selection criteria to conclude in which study population the prophylactic use of NPWT would be beneficial to reduce the SSI rate.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.