
Abstract
Background:
To investigate the risk factors for enterococcal intra-abdominal infections (EIAIs) and the association between EIAIs and outcomes in intensive care unit (ICU) patients.
Methods:
We reviewed retrospectively the records of patients with intra-abdominal infections admitted to the Department of Critical Care Medicine at Nanfang Hospital, Southern Medical University, China, from January 2011 to December 2018. Patients with intra-abdominal infections were divided into enterococcal and non-enterococcal groups based on whether enterococci were isolated from intra-abdominal specimens.
Results:
A total of 431 patients with intra-abdominal infections were included, of whom 119 were infected with enterococci and 312 were infected with non-enterococci. Enterococci were isolated in 27.6% of patients, accounting for 24.5% (129/527) of all clinical bacterial isolates. Post-operative abdominal infection (adjusted odds ratio [OR], 2.361; p = 0.004), intestinal infection (adjusted OR, 2.703; p < 0.001), Mannheim Peritonitis Index score (MPI; adjusted OR, 1.052; p = 0.015), and use of antibiotic agents within the previous 90 days (adjusted OR, 1.880; p = 0.025) were associated with an increased risk of EIAIs. Compared with patients without enterococcal infection, ICU patients with enterococcal infection had a higher risk of failure of initial clinical therapy (49.6% vs. 24.2%; p < 0.001) and longer hospital stays (33 days [19, 48] vs. 18 days [12, 29]; p < 0.001). Enterococcal infection was associated with increased 28-day mortality, in-hospital mortality, and ICU mortality. However, no difference was found in length of ICU stay between the two groups. Additionally, there was no difference in ICU mortality, hospital mortality, or 28-day mortality in patients infected with enterococcus who did or did not receive empirical anti-enterococcal therapy.
Conclusion:
Post-operative abdominal infection, intestinal infection, MPI score, and use of antibiotic agents within the previous 90 days were independent risk factors for enterococcal infection. Enterococcal infection was associated with reduced short-term survival in ICU patients.
Intra-abdominal infections (IAIs) are the second most common infectious disease in the intensive care unit (ICU) after lung infection with an incidence of 20%–30% [1–3]. Intra-abdominal infections usually lead to high morbidity and mortality [4]. Early clinical diagnosis, adequate source control to stop ongoing contamination, and appropriate antimicrobial therapy guided by the results of microbiologic testing are essential for effective IAI treatment [5–7]. Enterococcal species are the most common gram-positive bacteria found in ICU patients with IAIs [8]. Post-operative IAI, chronic comorbidities, high Acute Physiology and Chronic Health Evaluation (APACHE) II score, male gender, source of infection, and hypoproteinemia were considered high-risk factors for enterococcal isolation in patients with IAIs [9–12]. However, there are differences between ICU patients and patients on the general ward in terms of disease severity, prevalence of chronic underlying diseases, immune status, and so forth, and there are few reports on ICU patients [13]. This study investigated the risk factors for enterococcal intra-abdominal infections (EIAIs) and the association between EIAIs and outcomes in ICU patients.
Patients and Methods
Study design and population
Patients with IAIs who were admitted to the ICU of Nanfang Hospital of Southern Medical University, Guangzhou, China, from January 1, 2011 to December 31, 2018 were included. Patients with IAI who were aged 18 years or older were consecutively included. Patients without intra-abdominal microbiologic culture results and patients who were discharged or died within 24 hours after ICU admission were excluded. This study was approved by the Ethics Committee of Nanfang Hospital of Southern Medical University (no. NFEC-2019-162).
Data collection and definitions
The data were extracted from the electronic medical record database of Nanfang Hospital and collected information included age, gender, IAI type, source of infection, comorbidities, Mannheim Peritonitis Index (MPI) score, APACHE II score, Sequential Organ Failure Assessment (SOFA) score, use of antibiotic agents and glucocorticoids within the previous 90 days, temperature, white blood cell (WBC) count, and results of microbial culture.
Patients meeting the criteria for IAI according to the 2005 International Sepsis Forum Consensus Conference [14] were considered eligible for inclusion in the study. Those criteria are clinical manifestations (including abdominal pain and systemic inflammatory response syndromes such as fever, tachycardia, and shortness of breath) that match the signs and symptoms of IAI and the laboratory examination of peritoneal specimens meets the criteria for infection or IAI confirmed by surgery or microbiologic culture of peritoneal specimens.
Community-acquired intra-abdominal infections (CA-IAIs) or healthcare or hospital-associated intra-abdominal infections (HA-IAIs) were defined according to the Surgical Infection Society's (SIS) definition [15,16]. Healthcare or hospital-associated IAIs are defined as follows: patients who have been hospitalized for at least 48 hours during the previous 90 days; patients residing in a skilled nursing or long-term care facility during the previous 30 days; patients who have received intravenous infusion therapy, wound care, or renal replacement therapy within the preceding 30 days; patients who have received several days of broad-spectrum antimicrobial therapy within the previous 90 days; patients who have post-operative infections; and patients known to have been colonized by or previously infected with a resistant pathogen. Patients not meeting those criteria were classified as CA-IAIs.
Hypotension was defined as a systolic arterial pressure <90 mm Hg, a mean arterial pressure <70 mm Hg [17], or a requirement for vasopressors to achieve a systolic arterial pressure ≥90 mm Hg.
Initial antibiotic treatment (IAT) failure was defined as discontinuation of the antibiotic regimen for reasons other than cure, de-escalation, or streamlining; a change in IAT because of perceived clinical failure; a dose increase or addition of another antibiotic agent after 48 hours of treatment; requiring an additional source control procedure >48 hours post-IAT; and in-hospital death from any cause [18].
Specimen, pathogen detection, and antibiotic sensitivity test
The intra-abdominal specimens were all obtained during surgery or within 24 hours after ICU admission and sent to the microbiology laboratory at Nanfang Hospital of Southern Medical University for processing. Isolated bacteria were identified using a Vitek® MS mass spectrometry microbial identification system (bioMérieux, Marcy-l'Étoile, France) or a BD PhoenixTM-100 automatic bacterial identification/drug susceptibility analyzer (Becton-Dickinson, Franklin Lakes, NJ).
End Points
Intensive care unit mortality, in-hospital mortality, ICU-free days, hospital-free days, and 28-day mortality were the primary end points. Initial antibiotic treatment failure, re-operation, length of hospital stay, and length of ICU stay were considered secondary outcomes.
Statistical analyses
Normally distributed continuous variables were expressed as the mean ± the standard deviation (SD), and the differences between groups were analyzed using a t-test or analysis of variance (ANOVA). Non-normally distributed continuous variables were expressed as the median [interquartile range [IQR]) and analyzed using the Mann-Whitney U test. Categorical variables were expressed as the number and percentage, and comparisons between groups were made using the χ2 test or Fisher exact test as appropriate. Multivariable log-binomial regression analysis was used to estimate the risk factors for enterococcal infection, adjusting for confounding variables that were selected based on a p value <0.10 in univariable analysis.
Statistical analysis was performed using Stata/MP version 15.0 (StataCorp, College Station, TX). A p value <0.05 was considered statistically significant.
Results
Patient characteristics
During the eight-year study period, 665 consecutive ICU admissions with IAIs were included. After excluding patients who met the exclusion criteria, 431 eligible patients were enrolled, of whom 181 (42%) were CA-IAIs and 250 (58%) were HA-IAIs (Fig. 1).
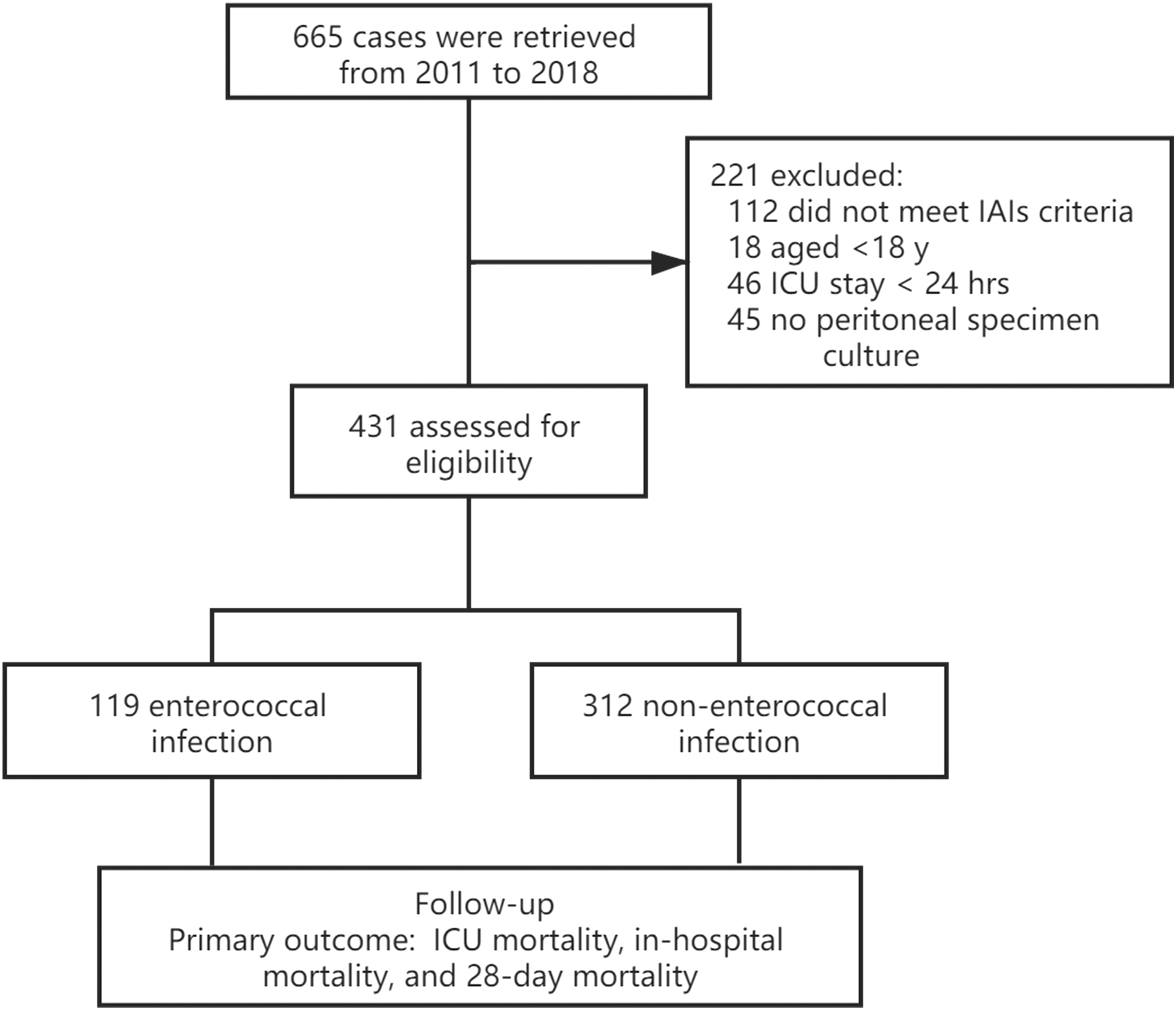
Flow chart of patients in the study. IAI = intra-abdominal infection; ICU = intensive care unit.
A total of 527 bacterial isolates were identified from 431 patients with IAIs. Of all these isolates, 48.2% (254/527) were gram-negative bacteria, 34.0% (179/527) were gram-positive bacteria, and 17.8% (94/527) were fungi. More specifically, 129 enterococci isolates were identified in 119 patients, with Enterococcus faecium 64 (49.6%) and Enterococcus faecalis 52 (40.3%), accounting for 24.5% (129/527) of all the clinical isolates. In this study, all of the enterococci isolates were sensitive to vancomycin, except for one isolate of Enterococcus casseliflavus that was intrinsically resistant.
There were no statistically significant differences in demographics, chronic underlying diseases, IAI type, glucocorticoid use, or WBC count in patients with enterococcal infection compared with those without. Compared with patients with non-enterococcal infection, patients with enterococcal infection more commonly had HA-IAIs, an intestinal source of infection and post-operative IAIs. The incidence of anastomotic leakage accounted for 47.5% among those with post-operative IAIs, which did not show a difference between the enterococcal and non-enterococcal groups. Enterococcal infection was strongly associated with an increased severity of disease, as reflected by higher APACHE II score, higher SOFA score, higher MPI score, more frequent occurrences of hypotension, and abnormalities in body temperature. When comparing the distribution of other organisms between the enterococcus group and the non-enterococcal group, there was no difference in the isolation rate of Enterobacteriaceae, streptococci, and fungus, whereas the isolation rate of non-fermenting bacteria in the enterococcus group was higher than that in the non-enterococcal group (Table 1).
Clinical Characteristics and Multivariable Analysis of ICU-IAI Patients in This Study
ICU = intensive care unit; IAI = intra-abdominal infection; OR = odds ratio; CI = confidence interval; HA = healthcare or hospital-associated; CA = community-acquired; COPD = chronic obstructive pulmonary disease; CKD = chronic kidney disease; AIDS = acquired immune deficiency syndrome; APACHE-II = Acute Physiology and Chronic Health Evaluation II; IQR = interquartile range; MPI = Mannheim Peritonitis Index; SOFA = Sequential Organ Failure Assessment; WBC = white blood cell count.
p: compared with the non-enterococcal infection group.
p: multivariable analysis by log-binomial regression of enterococcal and non-enterococcal infections.
Fever/hypothermia: temperature ≥38°C or ≤36°C.
Abnormal WBC: WBC ≥12 × 109/L or WBC <4 × 109/L.
Risk factors for enterococcal infection and outcomes
Enterococci were isolated in 27.6% (119/431) of ICU patients with IAI (ICU-IAI patients). The univariable analysis showed that HA-IAI, intestinal source of infection, post-operative IAI, chronic comorbidities, APACHE II score, SOFA score, MPI score, use of glucocorticoids and antibiotic agents within the previous 90 days, presence of shock, and abnormalities in body temperature were associated with an increased risk of enterococcal infection. The multivariable log-binomial regression analysis showed that post-operative abdominal infection (p = 0.004), intestinal source of infection (p < 0.001), MPI score (p = 0.015), and use of antibiotic agents within the previous 90 days (p = 0.025) were independent risk factors for enterococcal infection (Table 1). The enterococcal group had a higher rate of IAT failure and longer average in-hospital stay than the non-enterococcal group. Similarly, the enterococcal group had shorter hospital-free days within 28 days than the non-enterococcal group. However, there was no difference in re-operation rate between the two groups. In terms of mortality risks, ICU mortality, hospital mortality, and 28-day mortality were all higher in the enterococcal group than in the non-enterococcal group (Table 2).
Association between Enterococcal Infection and Clinical Outcomes in ICU-IAI Patients
ICU = intensive care unit; IAI = intra-abdominal infection; IQR = interquartile range.
Analysis of the effect of anti-enterococcal therapy on prognosis in the enterococcal infection group
According to the susceptibility results of Enterococcus, the empirical anti-enterococcal therapy was defined as at least one type of antibiotic agent in the initial anti-infection regimen that was sensitive to the isolated enterococci, otherwise, it is not. After enterococci were isolated, targeted anti-enterococcal therapy was given based on drug susceptibility, which was defined as transferred target anti-enterococcal therapy.
According to drug susceptibility results, 119 patients in the enterococcal infection group were divided into two subgroups, one group received empirical anti-enterococcal therapy (82 cases) whereas the other did not (37 cases). There was no difference in ICU mortality, in-hospital mortality, or 28-day mortality between the two subgroups. Twenty-one patients (56.8%) in the non-empirical anti-enterococcal subgroup received targeted enterococcal therapy after the culture results were obtained (Table 3). Compared with the empirical enterococcal therapy group and the transferred target anti-enterococcal therapy group, there was no difference in severity with similar APCHE II and SOFA scores, whereas patients in the transferred target enterococcal therapy group had a higher mortality rate, with ICU mortality, in-hospital mortality, and 28-day mortality all exceeding 40% (Table 4).
Prognosis of Subgroups Received or Did Not Receive Empirical Anti-Enterococcal Therapy in Enterococcal Infection Group
ICU = intensive care unit.
Prognosis of Anti-Enterococcal Therapy in Enterococcal Infection Group
ICU = intensive care unit; APACH -II = Acute Physiology and Chronic Health Evaluation II; SOFA = Sequential Organ Failure Assessment.
Discussion
Enterococci are the most common gram-positive bacterial cause of IAIs [8,9,13,19]. However, because of the high heterogeneity of these patients, there is a wide range of previously reported enterococcal infection rates in IAIs (from 4.5%–56.0%) [8,19–21]. In this study, 431 ICU-IAI cases were recorded, and the incidence of enterococcal isolates was 27.6%. Some prior studies have reported that enterococci are rarely isolated in CA-IAIs [19,20], a finding inconsistent with other previous reports. We found the rate of isolation of enterococci from CA-IAI patient samples was as high as 14.4% at our center, which was considerably higher than that in non-ICU IAI patients. Different sections of the digestive tract are colonized by different pathogenic bacteria, and the ICU-IAI population is different from the IAI population on general wards; perhaps disease severity should be considered when examining differences in enterococcal isolation. Enterococcal infection rates tended to vary between specific types of IAI patients. Prior subgroup analyses showed rates of approximately 50.0% in post-operative IAI patients [9,12]. In our study, the post-operative IAI enterococcal infection rate was 45.0% (54/120), which is concordant with the results of other studies. Patients with IAIs caused by digestive tract perforation have a high probability of enterococcal infection, at 56% as reported by Nichols et al. [22]. However, for further analysis of anastomotic leakage among post-operative IAI patients, no difference was shown between the enterococcal group and the non-enterococcal group, which is inconsistent with previous research [23].
These data suggest that once the structure of the gastrointestinal tract is compromised, the risk of enterococcal infection is increased. In addition, we found that the enterococcal group had higher coinfection rate of nonfermenting bacteria, which may be related to the difference in disease severity between the two groups.
Enterococci are part of the normal human microbial flora and have been ignored for a long time because of their relatively low virulence and the belief that this organism represents a non-pathogen or a co-pathogen [9,24]. With an increasing number of reported enterococcal infections [25], scholars and clinicians have begun to pay more attention to the high-risk profile of enterococci [9–11]. Post-operative IAI, chronic comorbidities, APACHE II score, male gender, source of infection, and hypoproteinemia were considered to be risk factors for enterococcal infection [9–12]. Inconsistent with previous studies, we found that post-operative abdominal infection, intestinal source of infection, MPI score, and prior antibiotic use were risk factors for enterococcal infection.
Previous studies have confirmed that post-operative IAIs and intestinal perforation lead to secondary IAIs related to enterococcal infection [12,22]. Destruction of the digestive tract allows Enterococcus to spread to the peritoneal cavity. When other antibiotic-sensitive micro-organisms are eliminated, Enterococcus can colonize and proliferate ectopically in the peritoneal cavity, leading to IAIs. Receiving antimicrobial therapy within the previous 90 days can increase the risk of EIAI in ICU patients by 88.0%. Because of the widespread use, and even abuse, of β-lactams, the growth of normally dominant bacterial species in the digestive tract, such as Enterobacteriaceae, is severely inhibited, and inferior bacteria, such as Enterococcus species, and fungi have the opportunity to multiply rapidly. Once intestinal perforation occurs, those patients are more likely to be infected with Enterococcus species or fungi. In addition, the higher rate of antibiotic use suggests that patients may have more chronic underlying diseases, which have also been found to be risk factors for enterococcal infection in previous studies [26].
Immunosuppression is more likely to be seen in enterococcal infection [11]. In our study, we found that immunosuppression is a risk factor for Enterococcus infection on univariable analysis, but no statistically significant differences were found on multivariable analysis. This may because of the small number of immunosuppressed patients (only 32 cases). Of note, the impact of immunosuppression as a potential risk factor needs to be confirmed by future studies.
The MPI is recommended by several guidelines for assessing IAI severity and prognosis [16,27]. The MPI incorporates the patient's demographics, pathophysiologic characteristics, and the severity of abdominal infection. The input parameters for the MPI are easy to acquire. The MPI score is closely associated with outcomes and is superior to the APACHE II and SOFA scores [16]. In our multivariable log-binomial regression analysis, the MPI score was found to be an independent risk factor for enterococcal infection. A recent study on damage control strategy found that high MPI scores were associated with ongoing peritonitis, and ongoing peritonitis was more common in enterococcal and fungal infections, and enterococcal infections were associated with high mortality and anastomotic leakage [23]. However, the causal relation between high MPI scores and enterococci is currently unclear; perhaps high MPI scores may be the result of the virulent effect of EIAIs. In any case, it appears that high MPI scores have a higher risk of enterococcal infection.
Enterococci can act as opportunistic pathogens, particularly in elderly patients with serious underlying diseases and other immunocompromised patients who have been hospitalized for prolonged periods, been treated with invasive devices, or received broad-spectrum antimicrobial therapy, all of which are common in the ICU. It has long been controversial whether patient outcomes depend on the enterococcal infection or the underlying disease itself [9,12,28,29]. In these studies, patients with enterococcal infection had a higher IAT failure rate and longer in-hospital stay compared with patients without enterococcal infection, even though the two groups were similar in age, chronic underlying disease status, and disease severity. Enterococcus species, especially Enterococcus faecium, are broadly resistant to β-lactams, quinolones, aminoglycosides, and other antibiotic agents. In addition, IAT often fails to provide effective enterococcal coverage, which leads to IAT failure, longer antibiotic use, and a longer in-hospital stay.
Whether patients with enterococcal infection received empirical anti-enterococcal therapy, there was no difference in ICU mortality, in-hospital mortality, or 28-day mortality. This may be because more than half of the patients who did not receive the empirical anti-enterococcal therapy received targeted anti-enterococcal therapy. In addition, some of the isolated enterococci may not be pathogenic bacteria. In comparing the empirical anti-enterococcal therapy subgroup and the transferred target anti-enterococcal therapy subgroup, we found that ICU mortality, in-hospital mortality, and 28-day mortality were higher in patients who were transferred to targeted anti-enterococcal therapy after the isolation of enterococci, which is consistent with previous research [21], but there was no statistically significant difference in patients who were transferred to targeted anti-enterococcal therapy after the isolation of enterococci. Although no statistical significance was observed in this study, we still recommend empirical anti-enterococcal treatment for IAI patients at high risk of enterococcal infection, and targeted anti-enterococcal therapy should be administered imminently upon detection of Enterococcus.
Consistent with several previous studies [8,13,30], we found that patients in the enterococcal group showed increased ICU mortality, hospital mortality, and 28-day mortality compared with those in the non-enterococcal group. Theunissen et al. [30] reviewed the records of 119 patients with an IAI with positive abdominal specimen cultures and illustrated that enterococcal infection (adjusted odds ratio [OR], 3.88; 95% confidence interval [CI], 1.05–14.28; p = 0.044) and APACHE II score were independent predictors of mortality. A retrospective study in France examined 160 elderly (≥75 years old) ICU IAI patients and found that Enterococcus positivity was an independent risk factor for ICU death (adjusted OR, 2.24; 95% CI, 1.06–4.75; p = 0.04) [13].
However, there have been different findings in other studies [10,29]. In a postmortem analysis of the Study to Optimize Peritoneal Infection Therapy (STOP-IT) research, Sanders et al. [29] found that enterococcal infection was not associated with increased mortality in patients with IAI. Nevertheless, in this study, the mortality of patients in the enterococcal and non-enterococcal groups was only 2% (1/50) and 1% (4/468), respectively, vastly different from the high mortality of IAIs, indicating that the condition of the patients in this study group was generally mild. Although there are no comparable data directly examining the ICU patient population, we have reason to believe that enterococcal infection is a predictor of poor outcomes in patients with IAI given that these patients have varying degrees of chronic underlying disease or organ dysfunction and more often receive broad-spectrum antibiotics. Therefore, for ICU-IAIs, it is recommended that empirical anti-infective treatment to cover enterococci be considered in patients with risk factors for enterococcal infection, especially following abdominal surgery in patients with chronic underlying diseases, although this needs further investigation.
Our study has some limitations. First, it was a single-center retrospective observational study. These results need to be validated with multicenter trials. Second, ICU IAIs are conceptually ambiguous and could be easily taken to include ICU-acquired IAIs and severe IAIs. Our research subjects represented both CA-IAIs and HA-IAIs, critically ill IAIs, and IAIs in the setting of other critical conditions. When drawing conclusions from this study, the context of our data should be recognized. Third, it still needs to be further investigated in randomized controlled trial to verify whether or not empirical anti-enterococcal treatment should be applied for IAIs patients at high risk of enterococcal infection.
Conclusions
Post-operative abdominal infection, intestinal source of infection, MPI score, and history of antibiotic use were found to be independent risk factors for enterococcal infection. Patients with enterococcal infection have a higher in-hospital mortality and 28-day mortality. Clinicians should evaluate for enterococcal infections to adopt appropriate antibiotic treatment strategies.
Footnotes
Funding Information
This work was supported by the Natural Science Foundation of China [Grant Number 81871604], and the Natural Science Foundation of Guangdong Province, China [Grant Numbers 2017A030313590, 2016A030313561].
Author Disclosure Statement
The authors declare no conflicts of interest.